Fill Out Your Aetna Attending Physician Statement Form
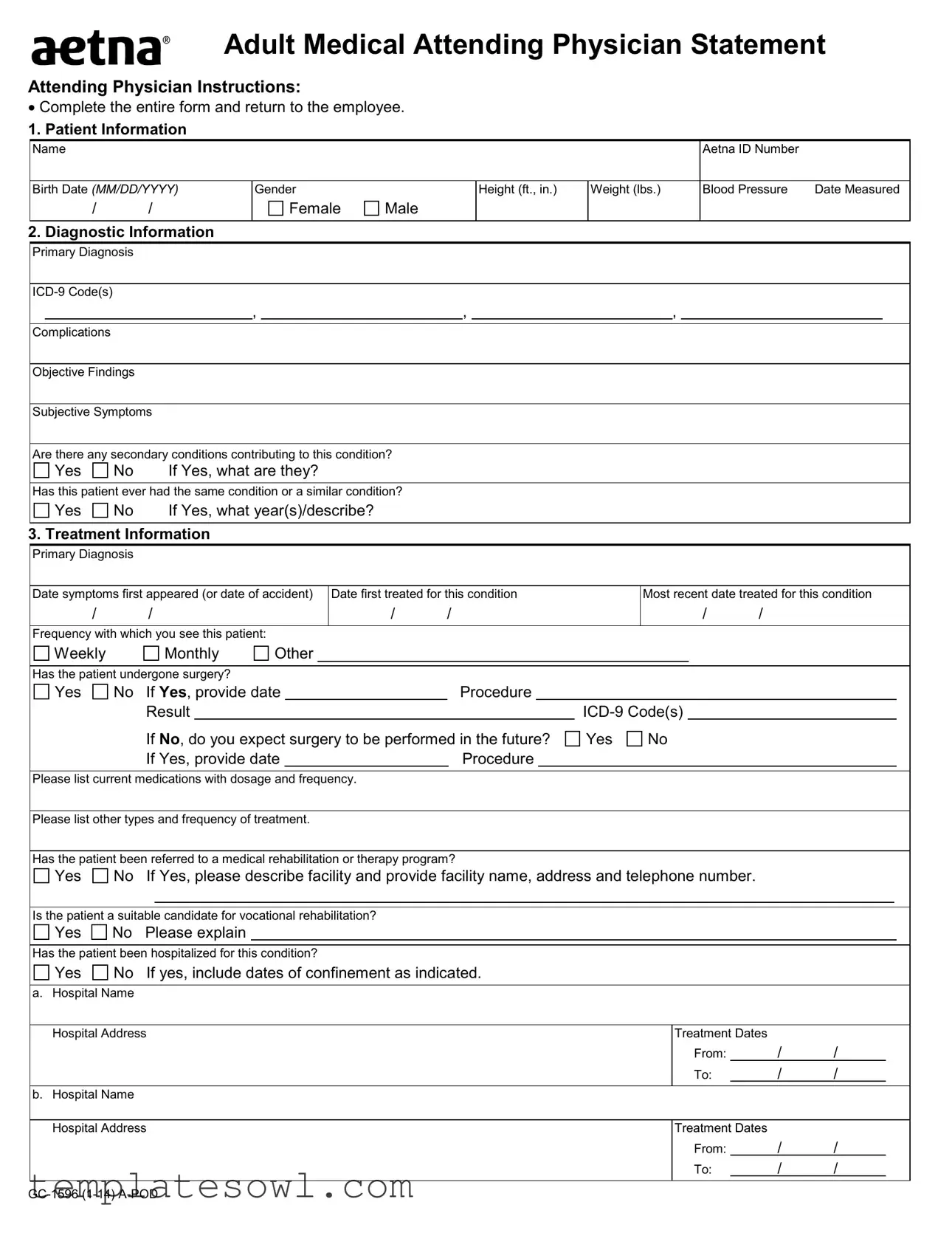
The Aetna Attending Physician Statement (APS) form serves a crucial role in the healthcare and insurance landscape, allowing for communication between healthcare providers and insurance companies regarding a patient’s health status and treatment plan. This form captures a comprehensive overview of the patient's medical history and current condition, beginning with essential patient information such as name, date of birth, and Aetna ID number. Following this, the primary diagnosis, along with relevant ICD-9 codes, must be documented alongside any complications that may arise from the condition. The form requires attending physicians to outline both objective findings—observable medical facts—and subjective symptoms reported by the patient, while also inquiring about any previous occurrences of similar conditions or secondary contributing factors. Treatment details are meticulously outlined, including dates of first and most recent treatments, surgical history, medications being taken, and any referrals made for rehabilitation. Progress indicators and assessments of the patient's current status are also critical parts of the form, providing a snapshot of recovery and ongoing challenges. Furthermore, the attending physician must evaluate the patient's level of impairment in physical and mental capacities, offering insight into how these limitations may impact their ability to work or perform daily activities. Lastly, the physician's information, including their degree and board certification status, is crucial for validating the credibility of the medical evaluation provided. Completing this form accurately not only ensures compliance with regulatory standards but also facilitates appropriate care and support for the patient, making it a vital tool in the intersection of healthcare and insurance services.
Aetna Attending Physician Statement Example
Adult Medical Attending Physician Statement
Attending Physician Instructions:
•Complete the entire form and return to the employee.
1. Patient Information
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Aetna ID Number |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Birth Date (MM/DD/YYYY) |
Gender |
|
|
|
|
|
Height (ft., in.) |
|
Weight (lbs.) |
|
|
|
|
Blood Pressure |
Date Measured |
|||||||||||||||||||
|
/ |
|
/ |
|
|
|
|
|
Female |
Male |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
2. Diagnostic Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Primary Diagnosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
, |
|
|
|
|
|
, |
|
|
|
|
|
|
|
, |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Complications |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Objective Findings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Subjective Symptoms |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Are there any secondary conditions contributing to this condition? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Yes |
No |
|
If Yes, what are they? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Has this patient ever had the same condition or a similar condition? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Yes |
No |
|
If Yes, what year(s)/describe? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
3. Treatment Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Primary Diagnosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Date symptoms first appeared (or date of accident) |
Date first treated for this condition |
|
|
Most recent date treated for this condition |
||||||||||||||||||||||||||||||
|
/ |
|
/ |
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
|
|
|
|
/ |
|
/ |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Frequency with which you see this patient: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Weekly |
|
|
Monthly |
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Has the patient undergone surgery? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Yes |
No |
If Yes, provide date |
|
|
Procedure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
Result |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
If No, do you expect surgery to be performed in the future? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
If Yes, provide date |
|
|
|
Procedure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Please list current medications with dosage and frequency. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Please list other types and frequency of treatment. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
Has the patient been referred to a medical rehabilitation or therapy program? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
Yes |
No |
If Yes, please describe facility and provide facility name, address and telephone number. |
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Is the patient a suitable candidate for vocational rehabilitation? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Yes |
No |
Please explain |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Has the patient been hospitalized for this condition? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Yes |
No |
If yes, include dates of confinement as indicated. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
a. |
Hospital Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Hospital Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treatment Dates |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
From: |
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To: |
/ |
/ |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. |
Hospital Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Hospital Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treatment Dates |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
From: |
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To: |
/ |
/ |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Adult Medical Attending Physician Statement
Page 2
Name |
|
|
|
|
|
|
|
|
|
|
|
Birth Date (MM/DD/YYYY) |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
4. Progress |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Status |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Recovered |
|
Improved |
Unchanged |
|
Retrogressed |
|
|
|
|||||||
Ambulatory |
|
Home Bound |
Bed Confined |
|
Hospitalized |
|
|
|
|||||||
What is the prognosis? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Has the patient achieved Maximum Medical Improvement? |
If No, how soon do you expect fundamental changes in the patient’s medical condition? |
||||||||||||||
Yes |
No |
|
|
|
More than 6 months |
||||||||||
Please note any restrictions (activities your patient should not do). |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
Please note any limitations (activities your patient cannot do). |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
What is the patient’s current work status? |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
Please describe any physical and/or mental impairments. |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
||||||||
Date patient released from your care (if applicable) |
|
Date patient able to return to full duty |
|
|
|
||||||||||
|
/ |
/ |
|
|
|
|
/ |
|
/ |
|
|
|
|
|
|
5. Level of Impairment |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Physical Impairment (if applicable): |
|
Does this patient have a mental/nervous impairment |
|||||||||||||
Class 1. No limitation of functional capacity/capable of |
impacting his/her level of functioning? |
|
|
||||||||||||
heavy work. |
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
Class 2. Slight limitation of functional capacity/capable of |
If Yes, provide diagnosis |
|
|
|
|
||||||||||
medium manual work |
|
|
|
Mental/Nervous Impairment (if applicable): |
|
|
|||||||||
Class 3. Moderate limitation of functional capacity/capable |
No limitation: able to function under stress and engage in |
||||||||||||||
of light work. |
|
|
|
|
interpersonal relationships. |
|
|
|
|||||||
Class 4. Marked limitation of functional capacity/capable |
Slight limitation: able to function in most stress situations |
||||||||||||||
of sedentary work. |
|
|
|
|
and engage in most interpersonal relationships. |
||||||||||
Class 5. Severe limitation of functional capacity/incapable |
Moderate limitation: able to engage in only limited stress |
||||||||||||||
of sedentary work. |
|
|
|
|
and limited interpersonal relationships. |
|
|
||||||||
|
|
|
|
|
|
Marked limitation: unable to engage in stress or |
|||||||||
|
|
|
|
|
|
interpersonal relationships. |
|
|
|
||||||
|
|
|
|
|
|
Severe limitation: has significant loss of psychological, |
|||||||||
|
|
|
|
|
|
physiological, personal and social adjustment. |
|||||||||
Cardiac Functional Capacity – NY Heart Association: |
|
|
|
|
|
|
|
|
|
|
|
||||
Class 1. No limitation |
Class 2. Slight limitation |
Class 3. Moderate limitation |
|
Class 4. Complete limitation |
|||||||||||
Do you believe your patient is competent to endorse checks and direct the use of the proceeds thereof? |
|
|
|
|
|
|
|
||||||||
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional Comments/Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||||
6. Attending Physician Information |
|
|
|
|
|
|
|
|
|
|
|
||||
Name |
|
|
|
|
|
|
|
|
|
|
Degree/Specialty |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Complete Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Telephone Number |
|
|
Fax Number |
|
|
|
|
|
|
Board Certified |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
Physician’s Signature |
|
|
|
|
|
|
|
|
|
|
Date (MM/DD/YYYY) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
The Genetic Information
Adult Medical Attending Physician Statement
Page 3
Name
8. Misrepresentation
Birth Date (MM/DD/YYYY)
/ /
Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.
Attention Alabama Residents: Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefit or who knowingly presents false information in an application for insurance is guilty of a crime and may be subject to restitution fines or confinement in prison, or any combination thereof.
Attention Arkansas, District of Columbia, Rhode Island and West Virginia Residents: Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefit or knowingly presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison.
Attention California Residents: For your protection California law requires notice of the following to appear on this form: Any person who knowingly presents a false or fraudulent claim for the payment of a loss is guilty of a crime and may be subject to fines and confinement in state prison. Attention Colorado Residents: It is unlawful to knowingly provide false, incomplete, or misleading facts or information to an insurance company for the purpose of defrauding or attempting to defraud the company. Penalties may include imprisonment, fines, denial of insurance and civil damages. Any insurance company or agent of an insurance company who knowingly provides false, incomplete, or misleading facts or information to a policyholder or claimant for the purpose of defrauding or attempting to defraud the policyholder or claimant with regard to a settlement or award payable from insurance proceeds shall be reported to the Colorado division of insurance within the department of regulatory agencies.
Attention Florida Residents: Any person who knowingly and with intent to injure, defraud, or deceive any insurer files a statement of claim or an application containing any false, incomplete or misleading information is guilty of a felony of the third degree.
Attention Kansas and Missouri Residents: Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person submits an enrollment form for insurance or statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto may have violated state law.
Attention Kentucky Residents: Any person who knowingly and with intent to defraud any insurance company or other person files a statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime.
Attention Louisiana Residents: Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefit or knowingly presents false information in an application is guilty of a crime and may be subject to fines and confinement in prison. Attention Maine and Tennessee Residents: It is a crime to knowingly provide false, incomplete, or misleading information to an insurance company for the purpose of defrauding the company. Penalties may include imprisonment, fines, or denial of insurance benefits.
Attention Maryland Residents: Any person who knowingly or willfully presents a false or fraudulent claim for payment of a loss or benefit or who knowingly or willfully presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison. Attention New Jersey Residents: Any person who includes any false or misleading information on an application for an insurance policy or knowingly files a statement of claim containing any false or misleading information is subject to criminal and civil penalties.
Attention New York Residents: Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information, or conceals for the purpose of misleading, information concerning any fact material thereto, commits a fraudulent insurance act, which is a crime, and shall be subject to a civil penalty not to exceed five thousand dollars and the stated value of the claim for each violation.
Attention North Carolina Residents: Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which may be a crime and subjects such person to criminal and civil penalties. Attention Ohio Residents: Any person who, with intent to defraud or knowing that he is facilitating a fraud against an insurer, submits an application or files a claim containing a false or deceptive statement is guilty of insurance fraud.
Attention Oklahoma Residents: WARNING: Any person who knowingly, and with intent to injure, defraud or deceive any insurer, makes any claim for the proceeds of an insurance policy containing any false, incomplete or misleading information is guilty of a felony.
Attention Oregon Residents: Any person who with intent to injure, defraud, or deceive any insurance company or other person submits an enrollment form for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto may have violated state law.
Attention Pennsylvania Residents: Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.
Attention Puerto Rico Residents: Any person who knowingly and with the intention to defraud includes false information in an application for insurance or file, assist or abet in the filing of a fraudulent claim to obtain payment of a loss or other benefit, or files more than one claim for the same loss or damage, commits a felony and if found guilty shall be punished for each violation with a fine of no less than five thousand dollars ($5,000), not to exceed ten thousand dollars ($10,000); or imprisoned for a fixed term of three (3) years, or both. If aggravating circumstances exist, the fixed jail term may be increased to a maximum of five (5) years; and if mitigating circumstances are present, the jail term may be reduced to a minimum of two (2) years.
Attention Texas Residents: Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person files an application for insurance or statement of claim containing any intentional misrepresentation of material fact or conceals, for the purpose of misleading, information concerning any fact material thereto may commit a fraudulent insurance act, which may be a crime and may subject such person to criminal and civil penalties.
Attention Vermont Residents: Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which may be a crime and may subject such person to criminal and civil penalties.
Attention Virginia Residents: Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent act, which is a crime and subjects such person to criminal and civil penalties.
Attention Washington Residents: It is a crime to knowingly provide false, incomplete, or misleading information to an insurance company for the purpose of defrauding the company. Penalties include imprisonment, fines, and denial of insurance benefits.
Page 4
Capabilities and Limitations Worksheet
Complete and sign the form using BLUE or BLACK ink.
Employee Name (Last, First, Middle Initial) |
Aetna ID Number |
Birth Date (MM/DD/YYYY) |
||||||
|
|
|
|
|
|
|
|
|
Gender |
|
Job Title |
|
|
|
|
||
|
Male |
Female |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Current Diagnosis |
|
|
|
Medications |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Indicate the percent of the day the following activities can be performed:
(Occasional
O F C N
Climbing
Crawling
Kneeling
Lifting
Pulling
Pushing
Reaching above shoulder
Forward reaching
Carrying
Bending
Twisting
O F C N
Hand grasping |
|
|
|
|
R |
|
L |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Firm hand grasping |
|
|
R |
|
|
L |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fine manipulation |
|
|
R |
|
L |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
L |
|
Gross manipulation |
|
|
|
|
|||||||||||||||
Repetitive motion |
|
|
R |
|
|
L |
|
||||||||||||
Sitting |
|
R |
L |
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Standing |
|
|
R |
|
|
|
L |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Stooping |
|
|
R |
|
|
|
L |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Walking |
|
|
R |
|
|
L |
|
|
|
|
|
|
|||||||
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Maximum weight patient is capable of lifting: |
|
|
|
Approved head and neck movements: |
|
|
|
|||||||||
|
|
|
|
|
|
Yes |
No |
|||||||||
|
1 - 5 lbs. |
O |
F |
C |
N |
|
Static position |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
Frequent flexing |
|
|
|
|
|
||||
|
6 - 10 lbs. |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
Frequent rotation |
|
|
|
||||||
|
11 - 20 lbs. |
|
|
|
|
|
|
|
|
|
||||||
|
21 - 35 lbs. |
|
|
|
|
|
Can the patient operate: |
|
|
|
|
|
||||
|
36 - 50 lbs. |
|
|
|
|
|
|
Yes |
No |
|||||||
|
|
|
|
|
|
|
|
|
||||||||
|
51 - 75 lbs. |
|
|
|
|
|
|
A motor vehicle? |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
75 - 100 lbs. |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
Hazardous machine? |
|
|
|
||||||
|
100 lbs. + |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
Power tools? |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Limitations to: |
|
|
|
|
|
Exposure limitations: Yes |
No |
Yes No |
|||||||
|
Speaking |
|
|
hrs. |
|
|
|
|
|
Heat |
|
|
Dust |
|||
|
Vision (explain) |
|
|
|
|
|
|
|
Cold |
|
|
Fumes |
||||
|
Depth perception |
|
|
|
|
|
|
|
Dampness |
|
|
Chemicals |
||||
|
Hearing (explain) |
|
|
|
|
|
|
|
Noise |
|
|
Radiation |
||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
Total # of hours patient is capable of working per day: |
12 |
8 |
6 |
4 |
|
2 |
|
|
|||||||
|
Duration of restrictions |
|
|
Care complete: Yes |
No |
Next appointment |
|
|
|
|||||||
|
Additional Comments: |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician’s Signature |
Date (MM/DD/YYYY) |
Form Characteristics
| Fact Name | Details |
|---|---|
| Purpose of the Form | The Aetna Attending Physician Statement form is designed to collect essential medical information about a patient from their physician, which supports claims processing and benefit determinations. |
| Patient Information Section | This section captures critical details about the patient, including their name, Aetna ID number, date of birth, gender, height, weight, and blood pressure. |
| Diagnostic Information Requirements | Physicians must provide a primary diagnosis, relevant ICD-9 codes, and any complications or secondary conditions that may be affecting the patient’s health. |
| Treatment Information Collection | Details regarding treatment frequency, surgeries, and current medications are required. This assists in understanding the patient's ongoing medical needs. |
| Progress Monitoring | The form includes a section to assess patient progress, indicating whether the patient has recovered, improved, or requires continued care, including expected timelines for improvement. |
| State-Specific Legal Considerations | Each state has unique laws governing insurance fraud and medical information handling. For instance, Alabama and California note the legal penalties for submitting false information. |
Guidelines on Utilizing Aetna Attending Physician Statement
Filling out the Aetna Attending Physician Statement form requires careful attention to detail. This will ensure that all necessary information is accurately provided. Follow the steps below to complete the form correctly.
- Patient Information: Enter the patient's name, Aetna ID number, birth date, gender, height, weight, and blood pressure. Include the date the blood pressure was measured.
- Diagnostic Information: Provide the primary diagnosis and corresponding ICD-9 codes. Note any complications, objective findings, and subjective symptoms. Indicate if there are any secondary conditions and whether the patient has had the same or similar condition previously.
- Treatment Information: Fill in the date symptoms first appeared, the date of the first treatment, and the most recent treatment date. Specify the frequency of patient visits. Note any surgeries or future surgery expectations, including relevant details. List current medications and any other treatments the patient is receiving. Include information about any rehabilitation or therapy referrals.
- Progress: Assess the patient's status, prognosis, and whether they have achieved Maximum Medical Improvement. Document any activity restrictions or limitations, their current work status, and any physical or mental impairments. Include dates the patient was released from care or is expected to return to full duty.
- Level of Impairment: Evaluate any physical or mental impairments by classifying their limitations. Confirm whether the patient is competent to endorse checks related to proceeds from this claim.
- Attending Physician Information: Complete your name, degree/specialty, address, phone number, and fax number. Confirm if you are board certified. Sign and date the form.
Once completed, ensure that the form is returned to the employee. It is crucial to avoid any false information, as this could lead to severe penalties. Be meticulous in checking all input before submission.
What You Should Know About This Form
What is the purpose of the Aetna Attending Physician Statement form?
The Aetna Attending Physician Statement form serves as a comprehensive medical report that provides relevant information about a patient's health status. This form is designed to aid in the processing of insurance claims by detailing the patient's diagnosis, treatment history, and current medical condition. It includes sections for documenting important patient information, such as previous medical history, any diagnoses with corresponding ICD-9 codes, surgeries, medications, and the patient's current work capability. By filling out this form accurately, physicians help ensure that claims are appropriately evaluated and that patients receive the benefits they are entitled to.
Who is required to complete the Aetna Attending Physician Statement form?
This form must be completed by the attending physician responsible for the patient’s care. It is important for the physician to fill out every section, providing as much detail as possible. This includes the patient’s medical history, treatments received, and any limitations or capabilities that the patient may currently have. Once completed, the physician should return the form to the patient, who will then submit it to Aetna as part of their insurance documentation.
What information must be provided within this form?
Several critical pieces of information are necessary for appropriate processing. First, patient identification details, like name, Aetna ID number, birth date, and physical measurements, must be recorded. Second, the physician must specify the primary diagnosis along with any complication codes. The treatment section requires history regarding the onset of symptoms, previous treatments, surgeries, medications, and any referrals to therapy or rehabilitation programs. Finally, the physician should provide a prognosis along with any observed limitations regarding the patient’s physical or mental capabilities.
How does the Aetna Attending Physician Statement form impact an insurance claim?
The completion of this form can significantly influence the outcome of an insurance claim by providing essential documentation that supports the patient's medical condition. A thorough and accurate statement from the attending physician helps Aetna assess the claim with clarity. It can also influence decisions regarding eligibility for benefits, coverage of treatments, and, if applicable, vocational rehabilitation options. Thus, the form plays a critical role in the claims process, and accuracy is paramount to ensure that the patient's needs are met.
Common mistakes
Filling out the Aetna Attending Physician Statement form can be complex, and it's essential to avoid common mistakes that could delay processing or compromise the accuracy of information. One frequent error involves incomplete patient information. Without providing the patient's full name, Aetna ID number, and date of birth, the processing team may face difficulties in accurately identifying the patient and linking the claim to the correct records.
Another mistake occurs when entering diagnosis codes. The form requires specific ICD-9 codes for the primary diagnosis, along with any complications and secondary conditions. Commonly, physicians may forget to include these codes or may mistakenly enter outdated ones. This can lead to misunderstandings regarding the patient's medical situation, impacting the subsequent decisions about treatment and care.
Additionally, inconsistencies in reporting treatment dates pose a significant issue. Accurate dates for when symptoms first appeared, when the patient was first treated, and the most recent treatment date are crucial. Misstating these timelines can create confusion about the progression of the patient's condition, leading to inappropriate treatment recommendations.
The frequency of visits can also be incorrectly reported. Some might list an inconsistent follow-up schedule or fail to specify if it is weekly, monthly, or otherwise. This information is vital for assessing the continuity of care. A lapse in understanding how often the patient has been seen can hinder the evaluation of their response to treatment.
Moreover, failing to provide information on current medications can have serious implications. The form requires a comprehensive list of any medications the patient is taking, including dosages and frequency. Missing this information may result in Aetna lacking crucial data needed for assessing treatment efficacy and safety.
Finally, comments about the patient's work status and any restrictions should be clearly articulated. Not specifying whether the patient is suited for vocational rehabilitation or failing to outline limitations in activities can lead to misconceptions regarding the patient's capacity to return to work. Clear communication in these areas helps ensure that all parties involved in care can make informed decisions.
Documents used along the form
The Aetna Attending Physician Statement form is often accompanied by several key documents and forms that provide further clarity about a patient's health and treatment status. Each of these documents serves a specific purpose and can be critical for accurate insurance processing and patient care.
- Medical History Report: This document outlines the patient’s past medical conditions, treatments, surgeries, and other relevant health information. It is crucial for understanding the patient’s overall health.
- Disability Claim Form: Used to request disability benefits, this form requires detailed information about the patient’s condition and how it affects their ability to work and perform daily activities.
- Work Status Update: This form provides current insights into the patient's work capabilities, detailing any restrictions or accommodations that may be necessary.
- Progress Notes: These notes are kept by the attending physician during follow-up visits. They detail the patient's recovery progress and any changes in treatment or condition.
- Request for Health Information: This form is used to obtain additional health-related information from other healthcare providers to ensure a comprehensive understanding of the patient’s medical history.
- Independent Medical Examination (IME) Report: An IME report provides an objective assessment of the patient’s medical condition by a third-party physician, often required by insurance companies for claims verification.
- Authorization for Release of Medical Information: This document allows the sharing of the patient’s medical records with insurance companies or other relevant parties, ensuring compliance with privacy regulations.
In conclusion, these accompanying forms play a vital role in the medical and insurance processes. They enhance communication and help ensure that all parties involved have the necessary information for decision-making regarding the patient's care and insurance claims. Timely completion and submission of these documents can significantly impact the efficiency of claims processing.
Similar forms
-
Patient Health Questionnaire (PHQ): Similar to the Aetna Attending Physician Statement, the PHQ gathers comprehensive medical history and symptom details, aiding in the diagnosis and treatment planning process.
-
Disability Claim Forms: These forms require detailed medical information about the claimant's health status and impairment, similar to the Aetna form. They ensure that the claims are assessed accurately based on the patient’s medical condition.
-
Functional Capacity Evaluation (FCE): Like the Aetna form, the FCE assesses an individual's physical capabilities and limitations. It provides documentation on what a person can perform in terms of work-related activities.
-
Workers' Compensation Medical Report: This document outlines an injured worker's medical history, current condition, and treatment plan, just as the Aetna form does for employees seeking insurance benefits.
-
Insurance Policy Medical Questionnaire: This questionnaire collects essential health information from applicants. Its purpose parallels the Aetna form’s goal of evaluating the medical status of patients applying for benefits.
-
Medical Treatment Plans: These documents outline the proposed medical interventions. They share a common goal with the Aetna form: to provide a clear picture of the patient's treatment journey and expected outcomes.
Dos and Don'ts
- Do complete the entire form thoroughly before returning it to the employee.
- Do ensure that patient information, including diagnosis and treatment details, is accurate and up to date.
- Do communicate any expected changes in the patient's condition clearly.
- Do sign and date the form using blue or black ink.
- Don’t leave any sections blank unless instructed otherwise.
- Don’t provide genetic information, as it is not allowed by law.
- Don’t include any misleading or false information, as this could lead to serious penalties.
- Don’t forget to provide your contact information for any follow-up questions.
Misconceptions
- Misconception 1: The Aetna Attending Physician Statement form is only for patients with serious conditions.
- Misconception 2: Filling out this form is optional for physicians.
- Misconception 3: The form requires extensive and unnecessary information.
- Misconception 4: Only the primary diagnosis needs to be reported.
- Misconception 5: The form can be submitted without the physician's signature.
- Misconception 6: Once submitted, the form can't be updated or changed.
- Misconception 7: There are no legal repercussions related to the information provided.
- Misconception 8: The patient must be present for the physician to fill out the form.
- Misconception 9: The form will automatically guarantee benefits.
This form applies to all types of medical conditions, not just serious ones. It is designed to gather relevant medical information regardless of the diagnosis.
Completing this form is mandatory for physicians when requested. It ensures that all necessary information is provided to support the patient’s insurance claim.
Each section of the form is essential for understanding the patient's medical status and needs. This information is crucial for determining the appropriate benefits and care.
Both primary and any secondary diagnoses should be mentioned. This comprehensive approach provides a clearer picture of the patient’s overall health.
A physician’s signature is required for validation. This signature confirms that the information reported has been reviewed and is accurate.
If new information arises or corrections are necessary, modifications can be made before the review process is finalized. Communication with Aetna may allow necessary changes to be submitted.
It is important to provide accurate information. Misrepresentation can lead to legal consequences, including fines or loss of coverage.
Patients do not need to be present for physicians to complete the form. Physicians can provide information based on their medical history and ongoing treatment.
Filling out the form does not guarantee benefits. Aetna will review the form along with the patient's insurance policy to determine eligibility.
Key takeaways
- Always complete the entire Aetna Attending Physician Statement form before submission.
- Clearly provide patient information, including name, Aetna ID number, and birth date.
- Ensure accurate diagnostic information by including primary diagnosis, ICD-9 codes, and any complications.
- Input subjective symptoms and objective findings to give a fuller picture of the patient's condition.
- Indicate whether the patient has any secondary conditions and provide details if applicable.
- List all treatments and medications, specifying dosages and treatment frequencies.
- Document any surgeries the patient has undergone, including dates and procedures.
- Assess and note the patient's current status and prognosis, including any expected changes.
- Consider the patient's work status and ability to participate in vocational rehabilitation.
- Sign and date the form to validate the information provided.
Browse Other Templates
Injury Assistance Request,Compensation Claim Update,Medical Issue Notification,Injured Worker Support Form,Reimbursement Request Document,Disability Status Update,Claim Inquiry Form,Medical Treatment Appeal,Transportation Reimbursement Request,Worker - Workers have the right to request information updates and necessary support.
Lic 995 - Parents have the right to review reports of licensing visits and complaints from the last three years.