Fill Out Your Aetna Eoi Form
The Aetna Evidence of Insurability (EOI) form is a critical document utilized for applying for life and disability insurance coverage. It necessitates comprehensive information from both the plan sponsor and the employee or member seeking coverage. By following detailed instructions, the plan sponsor begins the process by completing Section A, ensuring all necessary items are filled out accurately, including social security numbers, contact information, and coverage details. Employees or members must then complete Section B, answering health-related questions that assess their insurability. Key components include reporting any existing health conditions, medication usage, and any medical history that may be relevant to the insurance application. The form also emphasizes the importance of privacy, noting that the information provided will remain confidential and only disclosed as necessary for business purposes or as required by law. Upon submission, Aetna may reach out for further information if necessary, and any incomplete forms will be returned unprocessed. It is vital for all parties to read through the entire form thoroughly to ensure accurate completion; misrepresentation or incomplete information could lead to denied claims or voided insurance coverage.
Aetna Eoi Example
Evidence of Insurability Statement
Life and Disability Coverage
Aetna Life Insurance Company
Read This Instruction Page Carefully.
Aetna may contact you directly to request additional information upon receipt of this completed Statement.
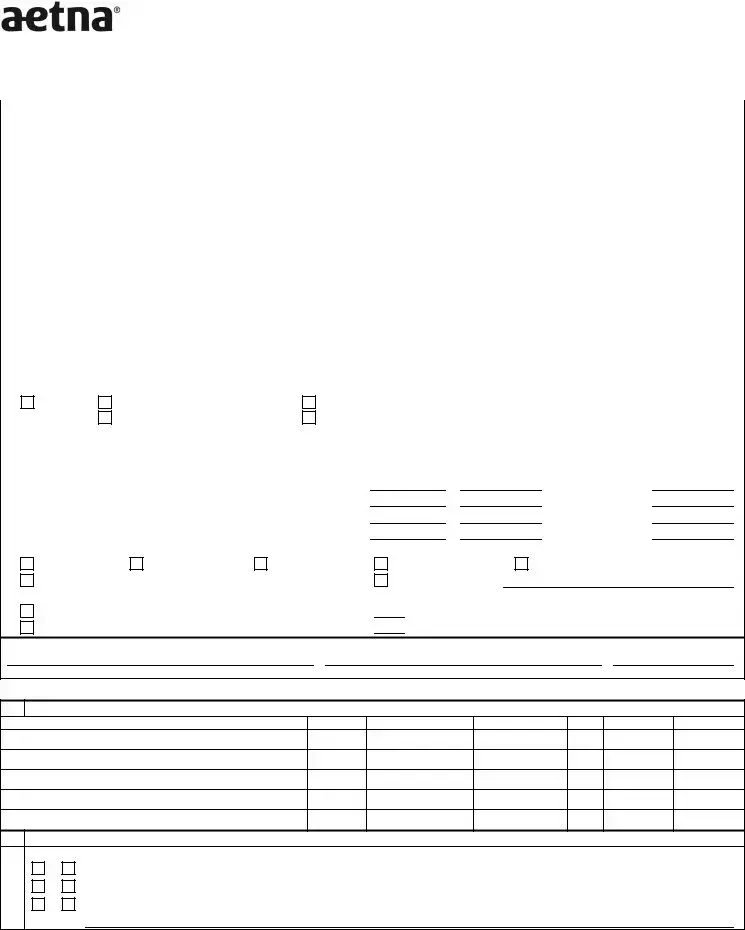
Instructions
Plan Sponsor
Please Print
Complete Section A in its entirety. Be sure that:
•All items are completed.
•The Control Number, Suffix and Account numbers are provided (A1).
•The Employee/Member’s Social Security Number is provided (A2).
•Both the Employee/Member’s and your name and address are shown in the spaces provided (A3 and A4).
•The telephone number of your authorized representative (A5), Employee/Member’s date of hire (A6) and Employee/Member’s home and work telephone numbers (A7) are provided.
•Your Employee/Member’s and your
•Employee/Member’s Annual Earnings is completed (A10).
•You check the appropriate box(es) for individual(s) requesting Life coverage. Provide the current (existing) amount of coverage, requested additional (new) amount of coverage, resulting total amount of coverage and Guarantee Issue amount for each individual for whom coverage is being requested (A11).
•You check the reason for requested life coverage (A11).
•You check the appropriate Disability box(es) and provide current and requested amounts or percentage of coverage (A11).
•Section A is signed by your Authorized Representative (A12).
Give the form to your Employee/Member for his/her confidential submission to Aetna.
Aetna will advise you of its coverage decision. Employee/Member will be notified directly if coverage is denied.
Employee/Member
Read the Privacy Notice and Misrepresentation section on “Page 2 of 4” of the Insurability Statement before completing.
Please Print
Verify that your name, address and Social Security Number as shown in Section A are complete and accurate. We may need to direct additional inquiries to your attention.
Complete Section B. Be sure that:
•All items are completed.
•Only the names of individuals requesting coverage at this time are listed (B1).
•Height and Weight must be provided or this form will be returned unprocessed for your completion (B1).
•The appropriate boxes regarding dependent child coverage are checked, if applicable (B2a, B2b, and B2c).
•Complete dates and details are given for all conditions checked in B3g, (B4).
•The form is signed by you. If you are requesting spouse coverage, the spouse’s signature is also required. Read the Certification, Acknowledgment and Authorization prior to signing the form (bottom of Section B).
Make a copy for your records. If a final underwriting decision cannot be made within six months, Aetna reserves the right to request a new Evidence of Insurability Statement.
Please Note: If this form is not completed in its entirety and signed, it will be returned unprocessed for your completion.
EOI |
|
Small Group |
Make a copy for your records. |
Privacy Notice
In evaluating your insurability, we (Aetna) will rely primarily on the health information you furnish to us in this Evidence of Insurability Statement. In addition, however, we may ask you to take a physical examination, or request additional medical information about you from any of the sources specified in the authorization on Page 4 of 4 of this form.
Disclosure of Information to Others
All of this information will be treated as confidential and will not be disclosed to others without your authorization, except to the extent necessary for the conduct of our business and not contrary to any law. For example, Aetna Life Insurance Company may also release information in its file to its reinsurer(s) and to other life insurance companies to whom you may apply for coverage, or to whom a claim for benefits may be submitted. In addition, information may be furnished to regulators of our business and to others as may be required by law, and to law enforcement authorities when necessary to prevent or prosecute fraud or other illegal activities.
Your Right of Access & Correction
In general, you have a right to learn the nature and substance of any information in our files about you. You also have a right of access to such files (except information which relates to a claim or a civil or criminal proceeding), and to request correction, amendment or deletion of recorded personal information in states which provide such rights and grant immunity to insurers providing such access. We may elect, however, to disclose details of any medical information you request to your (attending) physician. If you wish to exercise this right, or if you wish to have a more detailed explanation of our information practices, please contact:
Aetna Life Insurance Company, Medical Underwriting Department, 151 Farmington Avenue, Hartford, CT
Under New Mexico law, a resident of New Mexico has the right to register as a "protected person" in connection with disclosure of confidential domestic abuse information. If you wish to exercise this right, write to the address shown above.
Misrepresentation
Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.
Attention Alabama Residents: Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefit or who knowingly presents false information in an application for insurance is guilty of a crime and may be subject to restitution fines or confinement in prison, or any combination thereof. Attention Arkansas, District of Columbia, Rhode Island and West Virginia Residents: Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefit or knowingly presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison. Attention California Residents: For your protection, California law requires notice of the following to appear on this form: Any person who knowingly presents a false or fraudulent claim for the payment of a loss is guilty of a crime and may be subject to fines and confinement in state prison. Attention Colorado Residents: It is unlawful to knowingly provide false, incomplete, or misleading facts or information to an insurance company for the purpose of defrauding or attempting to defraud the company. Penalties may include imprisonment, fines, denial of insurance and civil damages. Any insurance company or agent of an insurance company who knowingly provides false, incomplete, or misleading facts or information to a policyholder or claimant for the purpose of defrauding or attempting to defraud the policyholder or claimant with regard to a settlement or award payable from insurance proceeds shall be reported to the Colorado division of insurance within the department of regulatory agencies. Attention Florida Residents: Any person who knowingly and with intent to injure, defraud, or deceive any insurer files a statement of claim or an application containing any false, incomplete or misleading information is guilty of a felony of the third degree. Attention Kansas and Missouri Residents: Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person submits an enrollment form for insurance or statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto may have violated state law. Attention Kentucky Residents: Any person who knowingly and with intent to defraud any insurance company or other person files a statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and may subject such person to criminal and civil penalties. Attention Louisiana Residents: Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefit or knowingly presents false information in an application is guilty of a crime and may be subject to fines and confinement in prison. Attention Maine and Tennessee Residents: It is a crime to knowingly provide false, incomplete or misleading information to an insurance company for the purpose of defrauding the company. Penalties may include imprisonment, fines or denial of insurance benefits. Attention Maryland Residents: Any person who knowingly or willfully presents a false or fraudulent claim for payment of a loss or benefit or who knowingly or willfully presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison. Attention New Jersey Residents: Any person who includes any false or misleading information on an application for an insurance policy is subject to criminal and civil penalties. Attention North Carolina Residents: Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which may be a crime and subjects such person to criminal and civil penalties. Attention Ohio Residents: Any person who, with intent to defraud or knowing he is facilitating a fraud against an insurer, submits an application or files a claim containing a false or deceptive statement is guilty of insurance fraud. Attention Oklahoma Residents: WARNING: Any person who knowingly, and with intent to injure, defraud or deceive any insurer, makes any claim for the proceeds of an insurance policy containing any false, incomplete or misleading information is guilty of a felony. Attention Oregon Residents: Any person who with intent to injure, defraud or deceive any insurance company or other person submits an enrollment form for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto may have violated state law. Attention Pennsylvania Residents: Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties. Attention Puerto Rico Residents: Any person who knowingly and with the intention to defraud includes false information in an application for insurance or file, assist or abet in the filing of a fraudulent claim to obtain payment of a loss or other benefit, or files more than one claim for the same loss or damage, commits a felony and if found guilty shall be punished for each violation with a fine of no less than five thousand dollars ($5,000), not to exceed ten thousand dollars ($10,000); or imprisoned for a fixed term of three (3) years, or both. If aggravating circumstances exist, the fixed jail term may be increased to a maximum of five (5) years; and if mitigating circumstances are present, the jail term may be reduced to a minimum of two (2) years. Attention Texas Residents: Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person files an application for insurance or statement of claim containing any intentional misrepresentation of material fact or conceals, for the purpose of misleading, information concerning any fact material thereto may commit a fraudulent insurance act, which may be a crime and may subject such person to criminal and civil penalties. Attention Vermont Residents: Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which may be a crime and may subject such person to criminal and civil penalties. Attention Virginia Residents: Any person who knowingly and with intent to injure, defraud or deceive any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent act, which is a crime and subjects such person to criminal and civil penalties. Attention Washington Residents: It is a crime to knowingly provide false, incomplete, or misleading information to an insurance company for the purpose of defrauding the company. Penalties include imprisonment, fines, and denial of insurance benefits. Attention New York Residents, the following statement applies only to your AD&D and Disability coverage: Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information, or conceals for the purpose of misleading, information concerning any fact material thereto, commits a fraudulent insurance act, which is a crime, and shall be subject to a civil penalty not to exceed five thousand dollars and the stated value of the claim for each violation.
Employee/Member’s or Authorized Person’s Signature: |
Date: |
|
|
Submission and Approval
The requested coverage will not be in effect unless and until evidence of insurability is submitted as required and is approved by Aetna.
Small Group Page 2 of 8 |
Evidence of Insurability Statement
Life and Disability Coverage
Aetna Life Insurance Company
A. Plan Sponsor: Complete this Section - Please print.
Make a copy for your records. Mail the original to:
Aetna Small Group
Underwriting
1. |
|
Control Number |
Suffix |
|
|
Account |
|
2. Employee/Member Social Security Number |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
3. |
Plan Sponsor Name & Address |
|
|
|
|
|
4. Employee/Member Name & Address |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ATTN: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street |
|
|
|
|
|
|
Street |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
State |
ZIP Code |
|
|
City |
|
|
State |
ZIP Code |
|
|||
|
|
|
|
|
|
|
|
|
||||||||
5. |
Plan Sponsor - Authorized Rep. Telephone Number |
|
6. Employee/Member Date of Hire |
|
7. Employee/Member Telephone Numbers (Including Area Code) |
|
|
|
||||||||
|
( |
) |
|
|
(MM/DD/YYYY) |
|
|
Work |
( |
) |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
Home |
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
8. |
Plan Sponsor |
|
|
|
|
|
9. Employee/Member |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
10. |
Employee/Member’s Annual Earnings $ |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
11. |
Coverage(s) Applied for: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Life*
Employee/Member Basic Life Spouse
Employee/Member Supplemental, Optional or Voluntary Life Child(ren)
|
Employee/Member |
|
|
|
Supplemental, |
|
|
Employee/Member |
Optional or |
Spouse |
Child(ren) |
Basic Life |
Voluntary Life |
Life |
Life |
a. Current (Existing) Amount of Life Insurance Coverage? |
$ |
||
b. Additional (New) Amount of Life Insurance Coverage requested? $ |
|||
c. Resulting Total Life Insurance Amount if Approved (a + b)? |
$ |
||
d. Guarantee Issue Amount of Life Insurance? |
|
$ |
|
*Reason for Requested Coverage (indicate all that apply). |
|
||
Salary Increase |
Change in Multiple |
Late Applicant |
|
Requesting an Amount in Excess of Plan’s Guaranteed Issue Limit |
|
||
Disability Coverages (Employee/Member Only): |
|
|
|
$
$
$
$
Change in Increments Other (Please explain)
$ |
|
$ |
$ |
|
$ |
$ |
|
$ |
$ |
|
$ |
Life Event/Status Change
Short Term Disability: |
Current Amount $ |
|
or |
Long Term Disability: |
Current Amount $ |
|
or |
% |
Requested Amount $ |
|
or |
|
% |
% |
Requested Amount $ |
|
or |
|
% |
12. I certify the above information is correct.
Plan Sponsor - Authorized Representative Signature |
Plan Sponsor - Authorized Representative Name (Please print) |
Date Signed (MM/DD/YYYY) |
B.Employee/Member: Complete this Section - Please print. All questions must be answered. Incomplete forms cannot be processed.
1.Only the Names of Individual(s) Requesting Coverage at this Time Should be Listed
Name
Employee:
Spouse:
Child(ren):
Relationship Birthdate (MM/DD/YYYY) Birthplace (City/State) Gender Height (ft., in.) Weight (lbs.)
Self
2.Complete these questions if dependent children are listed above. Use Number 4 if additional space is needed.
Yes |
No |
||
a. |
Do all dependent children live in your household? If No, please explain: |
|
|
b. |
Do all dependent children depend solely on you for support? If No, please explain: |
|
|
c. |
If any dependent child is age 19 or older, is/are they regularly attending school? If No, please explain: |
||
continued
EOI
Small Group Page 3 of 8 |
Employee/Member Social Security Number
B.Employee/Member: Complete this Section - Please print. (Continued)
3.Statement of Health for Individual(s) Listed Above. Please answer the following questions to the best of your knowledge and belief.
If any of the following questions are checked “Yes”, you must provide details in Number 4 below.
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
a. |
Is any individual pregnant? If Yes, |
Who: |
|
|
|
|
|
|
|
Date Due: |
|
|
|
|||||||
|
|
Any complications or problems? If Yes, explain: |
|
|
|
|
|
|
|
|||||||||||
b. |
Has any individual used tobacco products in the last 12 months (cigarettes, cigar, pipe, chewing tobacco)? |
|||||||||||||||||||
|
|
If Yes, Who: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
c. |
Are any inpatient or outpatient medical, surgical or diagnostic procedures recommended or contemplated: If Yes, When: |
|
||||||||||||||||||
|
|
Individual: |
|
|
|
|
|
|
|
|
|
|
|
Name of procedure: |
|
|||||
|
|
Reason for procedure: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
d. |
In the past 7 years, has any individual been confined to a hospital, clinic, sanatorium, rehabilitation or other treatment facility? |
|||||||||||||||||||
|
|
If Yes, Who: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Why: |
|
|
|
|
|
|
|
|
|
|
|
When: |
|
|||||
e. |
In the past 7 years, has any individual been examined, monitored or received medical treatment from any doctor, practitioner or |
|||||||||||||||||||
|
|
counselor for any condition other than minor illnesses (cold, flu, etc.)? |
|
|
|
|
|
|
||||||||||||
|
|
If Yes, Who: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Why: |
|
|
|
|
|
|
|
|
|
|
|
When: |
|
|||||
f. |
Is any individual(s) currently taking medication(s)? If Yes, complete the following information: |
|
|
|
|
|
|
|||||||||||||
|
Name of Individual |
|
Medication |
|
|
|
Dosage/Frequency |
Diagnosis |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
g.Within the past 10 years have you, your spouse or child(ren) had any disease, impairment of or treatment (other than minor illnesses) for any of the following? If Yes, check the appropriate box(es) and describe in Number 4.
AIDS* |
Cancer |
Immune System Disorder |
Nervous System |
||||
Arthritis Type: |
|
|
Carpal Tunnel Syndrome |
Intestine/Stomach/Ulcer |
Paralysis/Paresis |
||
Asthma/Emphysema/COPD |
Chest Pain |
Kidney/Bladder |
Reproductive System |
||||
Back/Spine/Neck |
Chronic Fatigue/Fibromyalgia |
Liver/Spleen/Pancreas |
Skin Disorder |
||||
Blood Disorder/Bleeding/Blood Clot |
Diabetes/Metabolic |
Lungs/Breathing |
Stroke |
||||
Blood Pressure/Hypertension |
Ears/Eyes |
Lupus Type: |
|
|
Substance Abuse (Alcohol/Drug) |
||
Blood Vessels/Circulation |
Epilepsy/Seizure |
Mental/Emotional Condition |
Throat/Tonsils/Swallowing |
||||
Bones/Joints |
Esophagus/Digestion/GERD |
Multiple Sclerosis |
Thyroid/Pituitary/Adrenal |
||||
Brain |
Heart |
Muscular Condition |
Tumor/Growth |
||||
Other
*AIDS (Acquired Immune Deficiency Syndrome) is a serious disease. It is caused by a virus called HIV (Human Immunodeficiency Virus). The virus is found in some human body fluids of infected people, most notably in semen and blood. If the AIDS virus finds its way into the bloodstream, it can damage the body’s defenses against disease, resulting in life- threatening diseases. There is no known cure.
4.In the space below, describe all conditions checked in 3g above and provide additional information for questions
Ques. |
Name of |
|
|
Date of |
Details/ |
Treatments |
Full Recovery Date |
|||||
No. |
Individual |
Diagnosis |
Onset |
Symptoms |
Received |
or is condition ongoing |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Check here if you are providing additional information on a separate attachment.
Certification: I certify these answers and statements are complete and true to the best of my knowledge and belief. I will inform Aetna of any material changes to the information provided which take place between the time the form is completed and the time coverage becomes effective. I agree that this document shall become a part of my request for group coverage and I acknowledge that I have retained a copy of this document as completed by me.
Acknowledgment: I understand that, to the extent permitted by state law, false statements may result in the denial of claims or in my insurance coverage being void as of its effective date with no benefits payable. I understand that conditions which are disclosed on this form may be subject to all conditions of my Plan Sponsor’s Plan including any preexisting condition limitations, fraud provisions and employee actively at work and dependent health condition requirements. My signature indicates that I have reviewed all information and statements on this form for completeness and accuracy.
Authorization: To all physicians and other health professionals, hospitals and other health care institutions, insurers, medical or hospital service and prepaid health plans, employers and
the Medical Information Bureau: You are authorized to provide Aetna Life Insurance Company (Aetna) information concerning healthcare, advice, treatment or supplies (including those related to mental illness and/or AIDS/ARC/HIV) provided me or any members of my family for whom coverage has been requested. (Minnesota residents are not required to provide information concerning results of AIDS/ARC/HIV tests performed on a criminal offender or a crime victim.) I acknowledge that information obtained from any or all of the above may result in further underwriting investigation. This information will be used for the purpose of determining eligibility for coverage. This authorization will be valid for twelve (12) months from the date signed. I acknowledge that I have read the Privacy Notice and Misrepresentation section shown on “Page 2 of 4” of this form and know that I have a right to receive a copy of this authorization upon request. I agree that a photographic copy of this authorization is as valid as the original.
Employee/Member’s or Authorized Person’s Signature (Required at all |
Date |
Spouse’s or Authorized Person’s Signature (Required if spouse |
Date |
times) |
|
coverage is requested) |
|
|
|
|
|
Small Group Page 4 of 8 |
Aetna complies with applicable Federal civil rights laws and does not discriminate, exclude or treat people differently based on their race, color, national origin, sex, age, or disability.
Aetna provides free aids / services to people with disabilities and to people who need language assistance.
If you are an existing Aetna member and need a qualified interpreter, written information in other formats, translation or other services, please call the number on your member ID card. If you are a prospective Aetna member, please call
If you believe we have failed to provide these services or otherwise discriminated based on a protected class noted above, you can also file a grievance with the Civil Rights Coordinator by contacting:
Civil Rights Coordinator,
PO Box 14462, Lexington, KY 40512 (CA HMO customers: PO Box 24030 Fresno, CA 93779),
Fax:
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf,
or at: U.S. Department of Health and Human Services, 200 Independence Avenue SW, Room 509F, HHH Building, Washington, DC 20201, or at
Aetna is the brand name used for products and services provided by one or more of the Aetna group of subsidiary companies, including Aetna Life Insurance Company, Coventry Health Care plans and their affiliates (Aetna).
Small Group Page 5 of 8 |
TTY: 711
To access language services at no cost to you, call
Para acceder a los servicios de idiomas sin costo, llame al
Afin d'accéder aux services langagiers sans frais, composez le
Para
Um auf für Sie kostenlose Sprachdienstleistungen zuzugreifen, rufen Sie
የቋንቋ አገልግሎቶችን ያለክፍያ ለማግኘት፣ በ
Անվճար լեզվական ծառայություններից օգտվելու համար զանգահարեք
Kugira uronke serivisi z’indimi atakiguzi, hamagara
Ngadto maakses ang mga serbisyo sa pinulongan alang libre, tawagan sa
Per accedir a serveis lingüístics sense cap cost per vostè, telefoni al
Para un hago' i setbision lengguåhi ni dibåtde para hågu, ågang
ᏩᎩᏍᏗ ᏚᏬᏂᎯᏍᏗ ᎤᏳᎾᏓᏛᏁᏗ Ꮭ ᎪᎱᏍᏗ ᏗᏣᎬᏩᎳᏁᏗ ᏱᎩ, ᏫᎨᎯᏏᎳᏛᏏ
Tajaajiiloota afaanii garuu bilisaa ati argaachuuf,bilbili
Voor gratis toegang tot taaldiensten, bell
Pou jwenn sèvis lang gratis, rele
Small Group Page 6 of 8 |
Για να επικοινωνήσετε χωρίς χρέωση με το κέντρο υποστήριξης πελατών στη γλώσσα σας, τηλεφωνήστε στον αριθμό
No ka walaʻau ʻana me ka lawelawe ʻōlelo e kahea aku i kēia helu kelepona
Xav tau kev pab txhais lus tsis muaj nqi them rau koj, hu
Iji nwetaòhèrè na ọrụ gasị asụsụ n'efu, kpọọ
Tapno maaksesyo dagiti serbisio maipapan iti pagsasao nga awan ti bayadanyo, tawagan ti
Untuk mengakses layanan bahasa tanpa dikenakan biaya, hubungi
무료 언어 서비스를 이용하려면
|
|
|
|||||
່ |
້ |
|
|
່ |
່ |
|
|
ເພອເຂາໃຊການບລການພາສາໂດຍບເສຍຄາຕກບທານ, ໃຫໂທຫາເບ |
|||||||
ື |
ົ |
້ |
ໍິ |
ໍ |
່ ໍັ ່ |
້ |
ີ |
Nan etal nan jikin jiban ikijen Kajin ilo an ejelok onen nan kwe, kirlok
េដមបទទលបានេសវាកមភាសាែដលឥតគតៃថសរមាបេលាកអកើីួិ សមេហៅទរសពេទៅកាន់ូន័ូេលខ់
Të kɔɔr yïn wɛɛr̈ ̈de thokic ke cïn wëu kɔr keek tënɔŋ yïn. Ke cɔl kɔc ye kɔc kuɔny ne nɔmba
For tilgang til kostnadsfri språktjenester, ring
Um Schprooch Services zu griege mitaus Koscht, ruff
Small Group Page 7 of 8 |
Para acessar os serviços de idiomas sem custo para você, ligue para
Pentru a accesa gratuit serviciile de limbă, apelați
Для того чтобы бесплатно получить помощь переводчика, позвоните по телефону
Za besplatne prevodilačke usluge pozovite
Heeba a nasta jangirde djey wolde wola chede bo apelou lamba
ܿ |
|
|
ܵ |
ܵܿ |
ܵ |
|
ܵ |
ܿܿ |
ܿ |
ܿ |
|
ܵ |
|
:ܢܘܡܝܪ |
|
|
ܵ |
|
|
|
|||||||
ܬܝܐܢܓܡ ܐܢܫܠܒ ܐܬܪܝܗܕ ܐ̈ܬܡܠܚ ܠܥ |
ܢܘܬܝ̄ ܐܩܝܢܣ ܢܐ |
||||||||||||
|
ܼ |
ܼ |
|
ܼ |
|
ܸ |
|
ܼܼ |
ܹ ܼ ܸ ܼ |
ܼ |
ܼ |
ܸ |
|
หากทานตองการเขาถงการบรการทางดานภาษาโดยไมมคาใชจาย่้ ้ ึ ิ ้่ ีโปรดโทร่ ้
Kapau ‘oku ke fiema’u ta’etōtōngi ‘a e ngaahi sēvesi kotoa pē he ngaahi lea kotoa, telefoni ki he
Ren omw kopwe angei aninisin eman chon awewei (ese kamo), kopwe kori
Щоб отримати безкоштовний доступ до мовних послуг, задзвоніть за номером
Nếu quý vị muốn sử dụng miễn phí các dịch vụ ngôn ngữ, hãy gọi tới số
Small Group Page 8 of 8 |
Form Characteristics
| Fact | Description |
|---|---|
| General Purpose | The Aetna Evidence of Insurability (EOI) form is used to assess an employee's eligibility for life and disability insurance coverage. |
| Submission Requirement | Both the employee/member and the authorized representative must complete their respective sections before submission to Aetna. |
| Incompleteness | If the form is incomplete or unsigned, Aetna will return it unprocessed, delaying coverage decisions. |
| Privacy Notice | Aetna maintains confidentiality of all personal health information provided within the form, complying with privacy laws. |
| State-Specific Laws | Misrepresentation laws vary by state; for example, New York imposes penalties for fraudulent claims under civil law. |
| Signature Requirement | Both the employee/member and authorized representative must sign the form to validate the provided information. |
| Eligibility Inquiry | Aetna may request additional medical information after receiving the EOI form to finalize the insurance coverage decision. |
| Final Approval | Coverage will not take effect until Aetna approves the Evidence of Insurability following their underwriting process. |
Guidelines on Utilizing Aetna Eoi
Filling out the Aetna Evidence of Insurability (EOI) form is a critical process that requires careful attention to detail. Once completed, the form will be reviewed by Aetna, and you will be notified about the coverage decision. To ensure a smooth submission, follow these detailed instructions.
- Plan Sponsor Section: In Section A, carefully print your information, including the Control Number, Suffix, and Account numbers, ensuring all fields are filled in completely.
- Provide the Employee/Member's Social Security Number in Part 2.
- Complete names and addresses for both the Plan Sponsor and the Employee/Member in Parts 3 and 4.
- List the telephone number of the authorized representative in Part 5, as well as the Employee/Member's date of hire (Part 6) and home and work telephone numbers (Part 7).
- Fill out email addresses for both the Plan Sponsor and the Employee/Member in Parts 8 and 9.
- Enter the Employee/Member's Annual Earnings in Part 10.
- In Part 11, check the appropriate boxes regarding the types of Life coverage applicable, and provide existing and requested coverage amounts.
- Check the appropriate Disability coverage boxes and indicate current and requested amounts in Part 11.
- Ensure the Authorized Representative signs Section A in Part 12.
- Give the completed form to your Employee/Member for submission to Aetna.
- Employee/Member Section: Begin Section B by verifying that your name, address, and Social Security Number are accurate and complete.
- List only the names of individuals requesting coverage in Part 1, including their relationships and demographic information.
- In Part 2, address any specific questions regarding dependent children by checking 'Yes' or 'No' and providing explanations as necessary.
- Answer the questions in Part 3 regarding individual health status to the best of your knowledge, marking each as 'Yes' or 'No.' If any response is 'Yes,' provide details in Part 4.
- For each condition checked in Part 3, describe the circumstances, including dates and treatments, as applicable.
- Ensure the certification is signed, acknowledging the completeness and accuracy of the statements provided.
- If coverage for a spouse is requested, obtain the necessity signature from the spouse.
- Make a copy of the completed EOI form for your records before submission.
After these steps are completed, the Aetna team will review the form. They might reach out for further clarification or paperwork if necessary.
What You Should Know About This Form
What is the Aetna EOI form?
The Aetna Evidence of Insurability (EOI) form is a document that employees and members complete to apply for life and disability insurance coverage. It requires detailed health information and personal data to assess eligibility. The EOI process ensures that insurance coverage can be determined accurately based on each individual's health status and history.
Who needs to complete the EOI form?
The EOI form must be completed by any employee or member who is requesting additional life or disability insurance coverage beyond the amounts automatically provided by the employer’s group plan. If an employee is adding coverage for a spouse or dependent, those individuals should also be included in the application.
What information is required on the EOI form?
Completing the EOI form requires various types of information. Employees must provide personal details, such as their name, address, Social Security Number, date of hire, and annual earnings. Health-related questions about current medical conditions, medications, and any relevant medical history must also be answered. This data helps Aetna assess the risk and decide on coverage.
What happens if the EOI form is incomplete?
If any section of the EOI form is left incomplete or if signatures are missing, Aetna will return the form unprocessed. This means the employee will need to provide the necessary information and submit the form again for it to be reviewed for coverage approval.
How is my health information handled by Aetna?
Aetna treats the health information provided in the EOI form as confidential. It will not disclose this information without authorization, except under circumstances necessary for conducting business and as mandated by law. Individuals have the right to access and request corrections to their health information in Aetna's files.
What should I do if I do not receive a decision on my EOI form?
If a decision regarding coverage has not been made within six months, Aetna may require a new EOI form to be submitted. It’s important to stay proactive and keep Aetna informed about any changes in health or circumstances during this time, as it may affect the coverage decision.
What are the consequences of providing false information on the EOI form?
Submitting false information on the EOI form can lead to serious consequences, such as denial of claims or cancellation of coverage. States have specific laws outlining penalties for insurance fraud, which may include fines and imprisonment. It is essential to provide accurate and truthful information to avoid these serious repercussions.
Common mistakes
Filling out the Aetna Evidence of Insurability (EOI) form can be a straightforward process, but certain common mistakes can lead to delays or outright denials of coverage. One major mistake is leaving sections incomplete. It is essential that all items are filled out in their entirety. Fields concerning personal details like your Social Security Number or contact information must not be overlooked, as any missing information could result in your form being returned.
Another common error is failing to provide the required Control Number, Suffix, and Account numbers. This specific information is critical for Aetna to process the request quickly and accurately. If these identifiers are absent, it may lead to confusion and delay in the insurance review process.
Many people forget to check the appropriate boxes for the coverage they are requesting. Skipping this step means that Aetna might not properly understand the extent of coverage you need, which can affect the decision on your insurability. Ensuring that the correct boxes are checked for Life and Disability coverage is crucial.
Additionally, inaccuracies regarding height and weight can also lead to complications. These details must be filled out correctly. If the figures do not match up with Aetna’s standards or records, the form may be returned unprocessed. Make sure these measurements are both precise and honest.
Failing to sign the form is another critical oversight. Signature requirements are not merely procedural; they are legally mandated confirmations of the information provided. Whether it’s the plan sponsor’s signature or the employee’s, missing signatures will render the application incomplete.
Lastly, it is vital to read the Privacy Notice and Misrepresentation section carefully. Understanding these terms ensures that all disclosures are made accurately and honestly. Misrepresentation, whether intentional or accidental, can lead to severe consequences, including denial of coverage. Taking the time to understand these guidelines not only protects your interests but also fosters a smoother application process.
Documents used along the form
When submitting an Aetna Evidence of Insurability (EOI) form, various accompanying documents may enhance the application’s completeness and facilitate a smoother approval process. Below are several common forms often used alongside the Aetna EOI form.
- Life Insurance Application Form: This form captures specific details about the individual applying for life insurance. It typically includes vital statistics, beneficiary designations, and policy selections.
- Health Questionnaire: Applicants provide more extensive medical history and current health status. This may include information on pre-existing conditions, medications, and any recent medical treatments.
- Authorization for Release of Medical Records: This document allows Aetna to obtain relevant medical information from the applicant's healthcare providers, ensuring that a thorough evaluation can be conducted.
- Dependent Information Form: If coverage is sought for dependents, this form details the names, dates of birth, and health information for each dependent, necessary for underwriting purposes.
- Policy Change Request Form: Should an existing policyholder wish to modify current coverage, this form specifies the desired changes to coverage amounts, beneficiaries, or classifications.
- Waiver of Premium Form: This document is used by applicants who wish to apply for a waiver of premium while disabled. It typically requires medical documentation of the disability.
- Accidental Death & Dismemberment (AD&D) Form: When applying for AD&D coverage, this form gathers details about potential risks or activities that may influence the underwriting decision.
- Notice of Insurance Information Practices: This explains how the insurance company collects, uses, and protects personal information. It reassures applicants that their data will be handled with confidentiality.
Providing these additional documents can help streamline the application process and improve the chances of approval for life and disability coverage through Aetna. Ensure that all forms are completed accurately to avoid delays in processing.
Similar forms
- Medical History Questionnaire: Similar to the Aetna EOI form, a Medical History Questionnaire collects health information from applicants seeking life or disability insurance. It typically requires detailed health questions and may also ask for lifestyle habits, like smoking or exercise, to assess risk for underwriting purposes.
- Health Insurance Application: An insurance application also gathers personal and health information. It serves as the initial request for coverage and often demands similar details, such as social security numbers and employment history, making it crucial for processing health insurance requests.
- Claims Form: Like the EOI form, a claims form necessitates personal information from the policyholder and might involve medical history to process claims regarding life or disability benefits. Accuracy is vital in both documents to ensure proper coverage evaluation and claims handling.
- Personal Health Statement: A Personal Health Statement is used in similar contexts to gather detailed health backgrounds. It often serves the same purpose in reviewing eligibility for insurance coverage and may ask similar medical questions to evaluate risk.
- Enrollment Form: Enrollment forms typically enroll individuals in a specific insurance plan and parallel the data gathering seen in the Aetna EOI form. They collect personal details, including dates of employment and existing coverage, to facilitate coverage decisions.
- Eligibility Verification Form: This form is often used to confirm a person's health insurance eligibility, requesting personal and health information akin to the Aetna EOI form. Its importance lies in validating insurance status before processing further applications.
Dos and Don'ts
When filling out the Aetna Evidence of Insurability (EOI) form, it is essential to proceed carefully to ensure that the application is processed smoothly. Here are nine guidelines to help you avoid common pitfalls.
- Ensure all sections are completely filled out. Incomplete forms will be returned for completion.
- Double-check the identification numbers. This includes the Control Number, Suffix, Account numbers, and your Social Security Number.
- Provide accurate contact information. This should include both the Employee/Member’s and the Authorized Representative’s names, addresses, and email addresses.
- Indicate the reason for requesting coverage. Clearly check the appropriate boxes for life and disability coverage.
- Sign the document. Ensure both the Employee/Member and the Authorized Representative have signed where necessary.
- Do not skip any questions or sections. Each question is vital for determining eligibility.
- Avoid using abbreviations. Write out all necessary information clearly to prevent misunderstandings.
- Refrain from leaving out medical history details. Omitting relevant health information can lead to complications with coverage.
- Do not rush the process. Take the time needed to review everything before submission to avoid errors.
By adhering to these guidelines, you can facilitate a smoother application process with Aetna. Properly completed forms and thorough checks can make a significant difference in how quickly and effectively your submission is handled.
Misconceptions
-
Misconception 1: The EOI form is only necessary for new applicants.
Many individuals mistakenly believe that the Evidence of Insurability (EOI) form is only required when applying for coverage for the first time. In reality, even existing members may need to submit the EOI form when requesting an increase in coverage or when applying for coverage for dependents. It's important to review coverage needs regularly.
-
Misconception 2: Completion of the EOI form guarantees approval.
Some may think that filling out the EOI form guarantees that their coverage will be approved. However, Aetna must evaluate the information provided, including health details and other factors, before a final decision is made. Approval is not automatic and relies on a review process.
-
Misconception 3: The EOI form can be submitted without all details filled in.
A common belief is that the form can simply be submitted without complete information. This is not true. If all required sections of the form are not filled out properly, Aetna will return the form unprocessed, causing delays in coverage. It's essential to ensure that all information is accurate and complete.
-
Misconception 4: Privacy is not a concern when submitting the EOI form.
Many people may think that their personal information is not protected when they submit the EOI. On the contrary, Aetna takes privacy seriously. All information provided in the EOI form is treated confidentially and will only be disclosed as permitted by law. Understanding privacy rights is crucial before submitting any form.
Key takeaways
- Accurate Details Matter: Ensure that all personal information, including names, addresses, and Social Security Numbers, are complete and accurate on the Aetna Evidence of Insurability (EOI) form.
- Complete All Sections: Every section of the form must be filled out completely. Incomplete forms can lead to delays or rejection.
- Understand Coverage Types: Familiarize yourself with the different types of coverage being requested, such as life and disability coverage, and the specific amounts needed.
- Providing Health Information: Be prepared to disclose detailed health history. Any conditions checked ‘yes’ on the form will require further explanation.
- Signatures Are Crucial: Both the plan sponsor and the employee/member must sign appropriate sections of the form. Missing signatures will result in the form being unprocessed.
- Keep a Copy: Always make a copy of the completed EOI form for your records before submitting it to Aetna. This ensures you have a reference for any future inquiries.
- Follow-Up on Requests: After submission, Aetna may contact the employee/member directly for further information. Stay vigilant for any communications from them.
- Disclosure Policies: Understand how your information will be shared. Aetna treats the submitted information confidentially, sharing it only in cases required by law or necessary for business operations.
- Watch for Misrepresentation: Misleading or incomplete information can lead to denial of claims or cancellation of coverage. Always provide truthful and complete answers.
Browse Other Templates
Application for Safelink Wireless - Be aware that providing false information can result in penalties, including fines or imprisonment.
Zaxby's Application - Bottled water is available throughout our locations for your convenience.
Certificate of Residency Form - Be prepared to present two different pieces of evidence when applying for the certificate.