Fill Out Your Af 4380 Form
The AF 4380 form, also known as the Air Force Special Needs Screener, plays a vital role in the relocation process for military personnel and their families. This form must be completed by sponsors who have family members with potential medical or educational requirements. The information collected serves multiple purposes: it documents the health care needs of family members, determines eligibility for special programs, and assists in planning and coordination of care during relocation. By providing insights into the special needs of family members, the AF 4380 form facilitates the Air Force's commitment to ensuring that essential medical and educational services are available. Completing this form is not only a requirement but also a means to support families in the military community. It is critical for sponsors to answer all relevant questions accurately and comprehensively, including inquiries about enrollment in the Exceptional Family Member Program and any ongoing medical services that family members may be receiving. Though the disclosure of personal information is voluntary, it is essential to understand that providing insufficient data can lead to delays in the screening process and affect the issuance of Permanent Change of Station (PCS) orders. Completing the AF 4380 helps ensure that families receive the appropriate support and services they may need as they transition to new locations.
Af 4380 Example
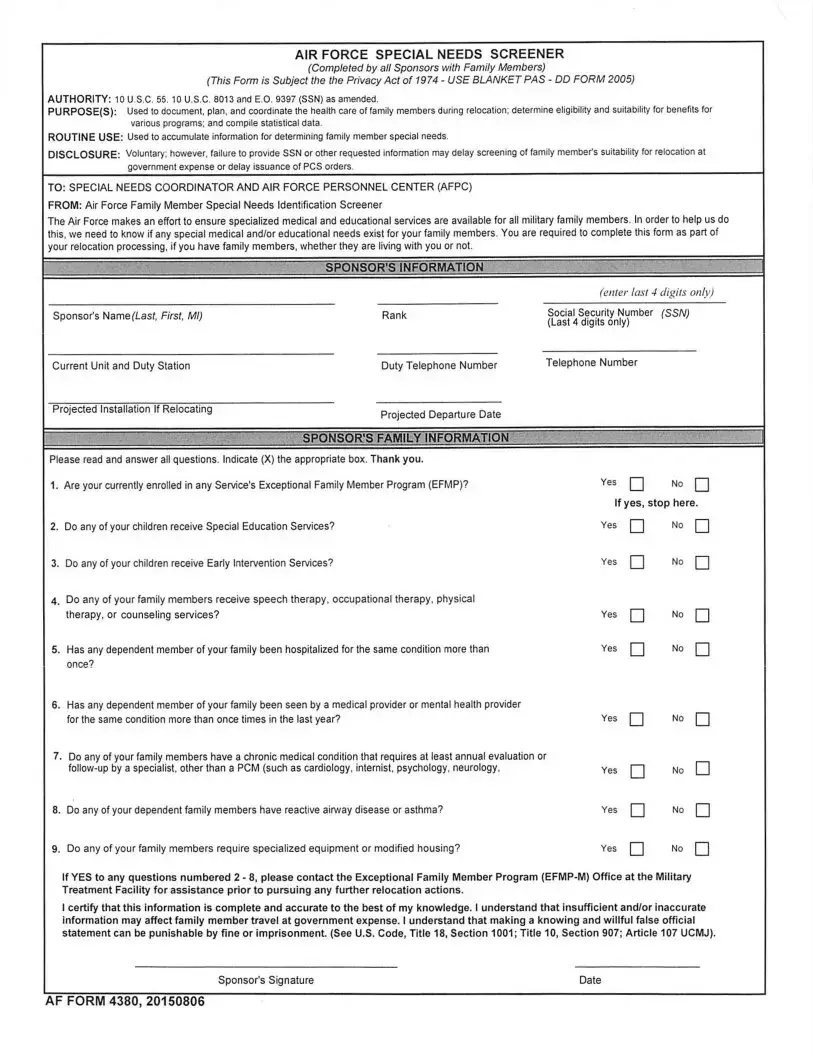
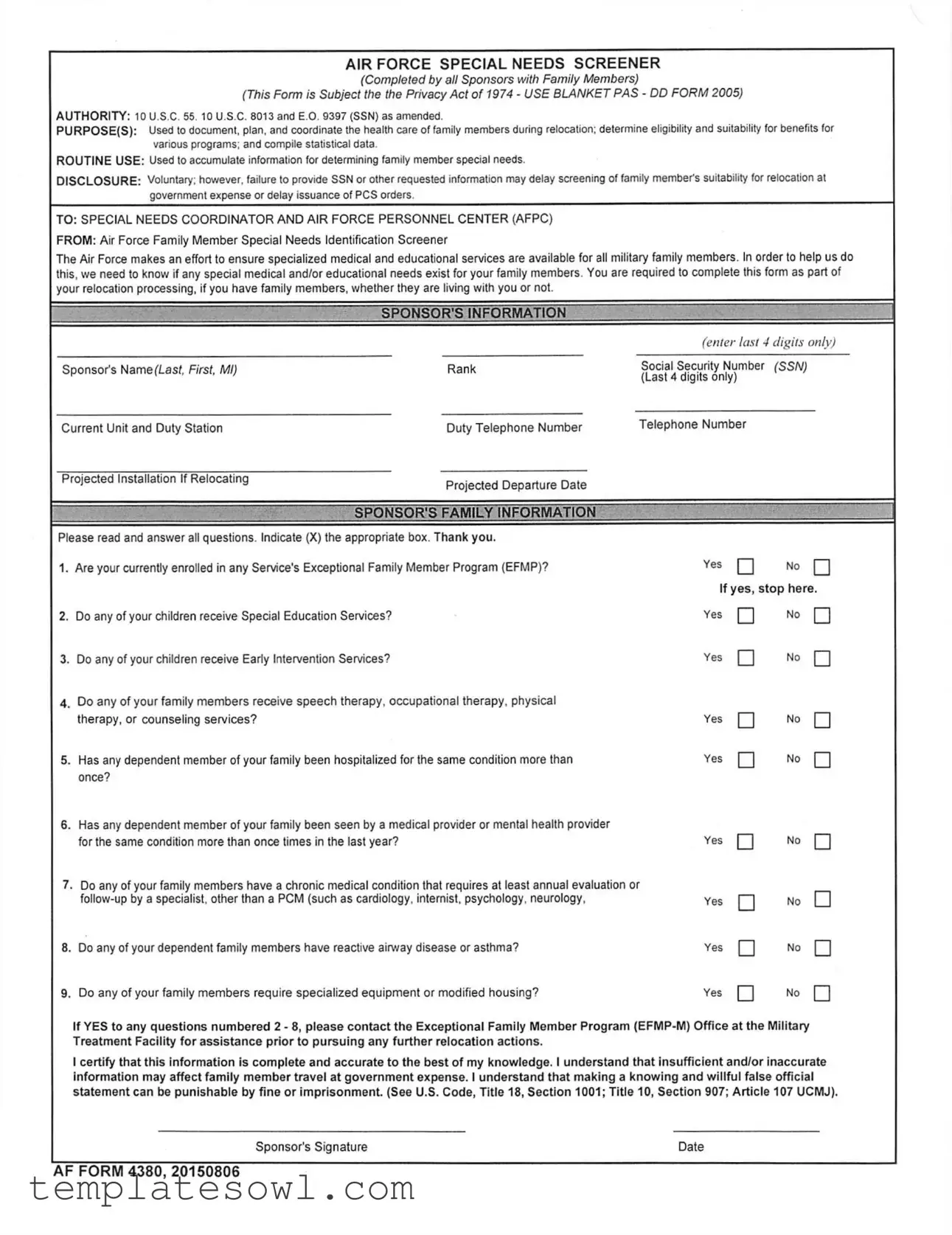
AIRFORCE SPECIAL NEEDS SCREENER
(Completed by all Sponsors with Family Members)
(This Form is Subject the the Privacy Act of 1974 - USE BLANKET PAS - DD FORM 2005)
AUTHORITY: 10 U.S.C. 55. 10 U.S.C. 8013 and E.O. 9397 (SSN) as amended.
PURPOSE(S): Used to document, plan, and coordinate the health care of family members during relocation; determine eligibility and suitability for benefits for various programs; and compile statistical data.
ROUTINE USE: Used to accumulate information for determining family member special needs.
DISCLOSURE: Voluntary; however, failure to provide SSN or other requested information may delay screening of family member's suitability for relocation at
government expense or delay issuance of PCS orders.
TO: SPECIAL NEEDS COORDINATOR AND AIR FORCE PERSONNEL CENTER (AFPC)
FROM: Air Force Family Member Special Needs Identification Screener
The Air Force makes an effort to ensure specialized medical and educational services are available for all military family members. In order to help us do this, we need to know if any special medical and/or educational needs exist for your family members. You are required to complete this form as part of
your relocation processing, if you have family members, whether they are living with you or not.
|
SPONSOR’S INFORMATION |
= |
|
|
(enter last 4 digits only) |
Sponsor’s Name (Last, First, Ml) |
Rank |
Social Security Number (SSN) |
|
|
(Last 4 digits only) |
Current Unit and Duty Station |
Duty Telephone Number |
Telephone Number |
Projected Installation If Relocating |
Projected Departure Date |
|
|
|
|
|
SPONSOR'S FAMILY INFORMATION |
|
Please read and answer all questions. Indicate (X) the appropriate box. Thank you.
1. Are your currently enrolled in any Service's Exceptional Family Member Program (EFMP)? |
Yes Q |
No | |
If yes, stop here.
2. |
Do any of your children receive Special Education Services? |
Yes |
3. |
Do any of your children receive Early Intervention Services? |
Yes |
4. Do any of your family members receive speech therapy, occupational therapy, physical |
|
|
|
therapy, or counseling services? |
Yes |
5. |
Has any dependent member of your family been hospitalized for the same condition more than |
Yes |
|
once? |
|
6. Has any dependent member of your family been seen by a medical provider or mental health provider |
|
|
|
for the same condition more than once times in the last year? |
Yes |
7. Do any of your family members have a chronic medical condition that requires at least annual evaluation or |
|
|
|
Yes |
|
8. |
Do any of your dependent family members have reactive airway disease or asthma? |
Yes |
9. |
Do any of your family members require specialized equipment or modified housing? |
Yes |
□
□
□
□
□
□
□
□
No
No
No
No
No
No
No
No
□
□
□
□
□
□
□
□
If YES to any questions numbered 2 - 8, please contact the Exceptional Family Member Program
I certify that this information is complete and accurate to the best of my knowledge. I understand that insufficient and/or inaccurate information may affect family member travel at government expense. I understand that making a knowing and willful false official statement can be punishable by fine or imprisonment. (See U.S. Code, Title 18, Section 1001; Title 10, Section 907; Article 107 UCMJ).
Sponsor's Signature |
Date |
AF FORM 4380, 20150806
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Title | The AF 4380 is titled "Airforce Special Needs Screener" and is designed for sponsors with family members during relocation. |
| Legal Authority | This form is governed by multiple laws including 10 U.S.C. 55, 10 U.S.C. 8013, and E.O. 9397 (SSN) as amended. |
| Privacy Act | The form is subject to the Privacy Act of 1974, underscoring the importance of safeguarding personal information. |
| Purpose | The AF 4380 serves several purposes such as documenting, planning, and coordinating the health care of family members and assessing eligibility for benefits. |
| Routine Use | The information collected is routinely used to determine special needs of family members and informs relevant programs. |
| Voluntary Disclosure | The disclosure of information is voluntary. However, lack of information may delay relocation screenings and issuance of PCS orders. |
| Required Completion | Sponsors must complete this form during relocation processing if they have family members, regardless of cohabitation. |
| Family Member Inquiries | The form includes inquiries about family members' involvement in special education, therapies, and chronic medical conditions. |
| Special Needs Coordinator | Information gathered is sent to the Special Needs Coordinator and the Air Force Personnel Center (AFPC) for further processing. |
| Signature Requirement | Completion of the form requires the sponsor’s signature, affirming that the information provided is complete and accurate. |
Guidelines on Utilizing Af 4380
To ensure a smooth relocation process, completing the AF 4380 form accurately is crucial. This step-by-step guide will help you fill out the form effectively, making sure all necessary information is provided.
- Begin by entering the last four digits of your social security number in the designated field labeled "Sponsor's Information."
- Type your full name in the format of Last, First, Middle Initial in the "Sponsor's Name" section.
- Fill in your current unit and duty station where you are currently assigned.
- Input the projected installation if you are relocating.
- Indicate your rank in the corresponding field.
- Provide your telephone number so the necessary contacts can reach you.
- List the projected departure date from your current location.
- Enter your full social security number again, limiting to the last four digits.
- Re-enter your telephone number for consistency.
In the "Sponsor's Family Information" section, read each question carefully and respond appropriately.
- For the first question, indicate if you are currently enrolled in any Service's Exceptional Family Member Program (EFMP) by marking the applicable box.
- Answer whether any of your children receive Special Education Services.
- State if any of your children receive Early Intervention Services.
- Indicate if any family members receive speech therapy, occupational therapy, physical therapy, or counseling services.
- Mark yes or no for whether a dependent has been hospitalized for the same condition more than once.
- Answer if any family member has seen a medical or mental health provider for the same condition more than once in the last year.
- Respond if any dependent has a chronic medical condition requiring at least annual evaluation or follow-up by a specialist.
- Indicate if any of your family members have reactive airway disease or asthma.
- Note if any family members require specialized equipment or modified housing. If yes, you will stop here and should reach out to the EFMP-M Office.
At the end of the form, certify the accuracy of the provided information. Sign and date the document to finalize it. This will confirm that your information is complete and truthful, helping streamline your relocation process.
What You Should Know About This Form
What is the purpose of the AF 4380 form?
The AF 4380 form, known as the Air Force Special Needs Screener, helps document, plan, and coordinate health care for family members during relocation. It is essential for determining eligibility and suitability for various benefits. Completing this form provides critical information that allows the Air Force to assess special needs, ensuring that specialized medical and educational services are available for military families.
Who is required to complete the AF 4380 form?
All sponsors with family members are required to complete the AF 4380 form. This includes anyone relocating with dependents, regardless of whether those dependents live with them or not. The completion of this form is a crucial part of the relocation processing and allows the Air Force to provide appropriate support for family members' needs.
What happens if I do not provide my Social Security Number or other requested information?
While providing your Social Security Number and other information on the AF 4380 form is voluntary, failing to do so may result in delays. Specifically, incomplete information can postpone the screening of your family members' suitability for relocation at government expense and may affect the issuance of Permanent Change of Station (PCS) orders.
What should I do if my family has special needs?
If any of your family members have special needs, it's essential to indicate this on the AF 4380 form. You should answer all relevant questions honestly. If you answer “yes” to any questions regarding special educational or medical services, reach out to the Exceptional Family Member Program (EFMP-M) Office at the Military Treatment Facility for assistance before proceeding with any further relocation actions. This step can help ensure your family's needs are met during the transition.
Common mistakes
When filling out the AF 4380 form, people often make mistakes that can lead to complications in the special needs screening process. One common error is not providing complete information. It’s important to answer all questions fully. Any unanswered sections can result in delays or confusion regarding your family's needs.
Another mistake involves inaccurate information. Misinformation or typos can lead to significant problems later. Double-checking your details and ensuring accuracy is crucial for proper screening.
Some sponsors fail to include the required last four digits of their Social Security Number. This number is necessary for identification purposes. Without it, processing the form may be delayed.
Many people neglect to indicate whether their family members are currently enrolled in any services or programs. This oversight can prevent the Air Force from providing essential support that matches your family's specific needs.
Another frequent mistake is not stopping the process when indicated. If you answer "yes" to any of the questions related to special needs, you should follow the instructions given and contact the relevant EFMP office. Ignoring this step can complicate your relocation process.
Some sponsors also forget about the importance of timeliness. Submitting the AF 4380 form late can affect your family's relocation schedule. Filling it out promptly ensures that necessary resources are available on time.
Failing to sign the form is another common error. A signature is crucial as it certifies that the information provided is accurate. Missing a signature can lead to the form being rejected.
People often rush through the form, which can result in illegible handwriting. If the information cannot be read clearly, it may lead to misunderstandings about your family's needs.
Improperly filling out the family information section is also a mistake to watch for. All family members should be accurately represented to provide a clear picture of their needs.
Finally, some individuals do not seek help when unsure. If there are questions or uncertainties about the form, reaching out for assistance is vital. Not doing so can lead to incomplete or incorrect submissions, which ultimately hinders the screening process.
Documents used along the form
The AF 4380 form is an important document used by Air Force sponsors to report any special medical or educational needs of their family members during relocation. It helps ensure that the necessary resources and support are available, making the transition smoother. In addition to this form, several other documents and forms are typically used in conjunction with the AF 4380 to provide comprehensive care and assistance. Below are nine key documents often needed in this context.
- AF Form 594: This form is used for requests for the assignment of military members, ensuring they are stationed in locations that can accommodate the needs of their families.
- DD Form 2792: The Exceptional Family Member Medical Summary provides a thorough overview of a family member's medical condition. It helps determine eligibility for benefits and services.
- DD Form 2792-1: This is the Exceptional Family Member Educational Summary, which documents the educational needs of exceptional family members, ensuring appropriate services are in place.
- AF Form 350: The Family Member Exceptional Needs Index helps categorize and identify family members who require specialized services or support, facilitating better planning and coordination.
- AF Form 3883: This form is used for the Individual Education Plan (IEP) for exceptional family members in educational settings, detailing required services and accommodations.
- DD Form 214: After leaving service, this document outlines a member's military service record, which is often required for accessing certain benefits, including those related to family needs.
- AF Form 353: The Family Advocacy Program (FAP) provides resources and support for families facing difficulties, ensuring they receive the help needed.
- AF Form 228: The Child Development Program application to enroll children in quality childcare services, accommodating their developmental and special needs.
- EFMP Enrollment Information: This ongoing enrollment process ensures family members with special needs are recognized in the system, allowing for better service coordination and access.
Each of these forms plays a crucial role in strengthening the support network for military families, ensuring that any special needs are identified and met during relocation. Proper attention to these documents helps facilitate a smoother transition for service members and their families, ultimately enhancing their overall well-being.
Similar forms
- DD Form 2792 - Exceptional Family Member Medical Summary: This form is used to provide a detailed medical summary of family members with special needs. Both forms aim to ensure appropriate medical and educational services for military families by documenting specific needs.
- DD Form 2792-1 - Exceptional Family Member Program (EFMP) Special Education/Early Intervention Summary: Similar to the AF 4380, this document focuses on the needs of family members requiring special education or early intervention services. It addresses the educational aspect, complementing the AF 4380’s medical focus.
- AF Form 1180 - Application for Air Force Sponsorship: While this form is primarily used for applying for sponsorship, it also identifies family member needs. Like the AF 4380, it is crucial for relocation and ensures that families receive the necessary support during their transition.
- AF Form 1300 - Approved Leave or Pass Application: This document details leave requests, but also may take into account the family’s special needs during approval. Both forms intersect on the need for awareness of family circumstances that may affect travel and relocation.
- AF Form 422 - Physical Profile Serial Report: The AF 422 tracks fitness and health details of military personnel, including dependents' special needs. This ensures all medical backgrounds are considered in the relocation process.
- DA Form 3349 - Physical Profile: Similar to the AF 422, this form provides information regarding the profiles of family members that may affect military duties. Understanding the health status aids in planning accommodations during relocations.
- DD Form 2958 - Child Development Program (CDP) Enrollment Application: This document helps in enrolling children who may require special educational services. Its goal, like the AF 4380, is to streamline the process for families needing additional support.
- AF Form 194 - Family Care Plan: This plan is required for military members with dependents and focuses on their care needs when they are unavailable. Like the AF 4380, it prioritizes the well-being of family members during the sponsor's deployment.
- DD Form 1300 - Report of Casualty: Although it deals with casualties, it can document special needs emerging from critical medical issues. Awareness of special requirements continues to be vital, much like in the relocation process covered by the AF 4380.
Dos and Don'ts
Filling out the AF 4380 form can feel overwhelming, but it’s an essential step for military families with special needs. To ensure you complete it accurately, here’s a simple list of things to do and avoid:
- Do read the entire form carefully before starting.
- Do double-check your family member's information for accuracy.
- Do provide the last four digits of your Social Security Number (SSN) as requested.
- Do answer all questions honestly, especially regarding your family's needs.
- Do sign and date the form once it's completed.
- Don't leave any questions unanswered; this could delay your processing.
- Don't provide incorrect or outdated information about your family members.
- Don't ignore the importance of contacting the Exceptional Family Member Program if applicable.
- Don't forget that any inaccuracies could have consequences for your family's relocation benefits.
By following these guidelines, you can help ensure a smoother process for your military family's special needs screening.
Misconceptions
Understanding the AF 4380 form is vital for military sponsors with family members who have special needs. However, some misconceptions may cause confusion. Here are seven common misconceptions and clarifications about the AF 4380 form:
- It’s optional to complete the form. Many believe that filling out the AF 4380 is optional. In reality, if you have family members, completing this form is required as part of your relocation processing.
- Only families currently enrolled in EFMP need to fill it out. Some think that only families already in the Exceptional Family Member Program (EFMP) need to submit this form. However, it applies to all families with members who may have special medical or educational needs, regardless of current enrollment.
- The form is only for families relocating. Many assume the AF 4380 is solely for families during relocation. While it is used in that context, it is also important for documenting ongoing special needs for all military family members.
- Providing Social Security Numbers (SSNs) is mandatory. Some individuals believe that they must provide full SSNs on the form. Although disclosing SSNs is necessary, you can provide just the last four digits.
- Filling out the form has no consequences. A misconception exists that the form is harmless. In fact, not providing accurate information can delay you and your family’s relocation and benefits.
- The information will be shared openly. Some people worry that the information will be widely shared. The AF 4380 is protected under the Privacy Act of 1974, meaning it’s used only for official purposes.
- Completing the form doesn't impact benefits. Many think the completion of the form has no bearing on eligibility for benefits. However, it actually helps determine eligibility for programs and services that support families with special needs.
By understanding these misconceptions, sponsors can better navigate the AF 4380 form and ensure that their families receive the necessary support during relocation.
Key takeaways
Completing the AF 4380 form is an important step for military families with special needs. Understanding its requirements can ensure a smooth relocation process. Here are some key takeaways on filling out and using this form:
- Mandatory Completion: All sponsors with family members must complete the AF 4380 form as part of the relocation process, regardless of whether the family members live with them.
- Privacy Protection: The information provided is protected under the Privacy Act of 1974, ensuring confidentiality and proper handling of sensitive data.
- Eligibility and Benefits: This form helps determine eligibility for health care benefits and services for family members with special needs.
- Detail Requirements: Accurate and complete information is required for all questions to facilitate appropriate medical and educational services.
- Voluntary Disclosure: While providing a Social Security Number (SSN) is voluntary, omitting it may delay the screening process and affect relocation orders.
- Support Services: If any questions regarding medical or educational services receive an affirmative response, sponsors should contact the Exceptional Family Member Program (EFMP) for guidance.
- Legal Implications: Sponsors must certify that the information is accurate. Providing false information can lead to fines or imprisonment under U.S. law.
By carefully completing the AF 4380 form, military families can ensure that their specific needs are recognized and addressed during moves. This proactive approach enhances the support available to them at their new location.
Browse Other Templates
Member Register Format - Verify your information before handing in the completed registration form.
Donor Profile - Recognition preferences for public acknowledgment of donations.
Mn State Tax Payment - Interest applies to late payments, calculated on the number of days overdue.