Fill Out Your Aflac Wellness Form
When navigating the process of utilizing wellness benefits, the Aflac Wellness form plays a crucial role in simplifying claims related to health screenings and wellness activities. This form is designed specifically for individuals who have undergone various health assessments, ranging from routine annual physicals to specialized tests like colonoscopies and mammograms. It requires the submission of personal information about the policyholder and the patient, along with details regarding the specific health screening conducted. The form includes an authorization section, where the signer certifies the accuracy of the information provided and grants permission for medical professionals to share relevant health data with Aflac. This is vital for determining eligibility for benefits under the policy. Moreover, it is essential for users to complete all sections of the form accurately, as missing information can lead to delays in processing claims. There are also details about communication preferences and how the collected data will be handled, ensuring that privacy is respected throughout the claims process. Understanding these key components will help individuals effectively utilize their wellness benefits.
Aflac Wellness Example
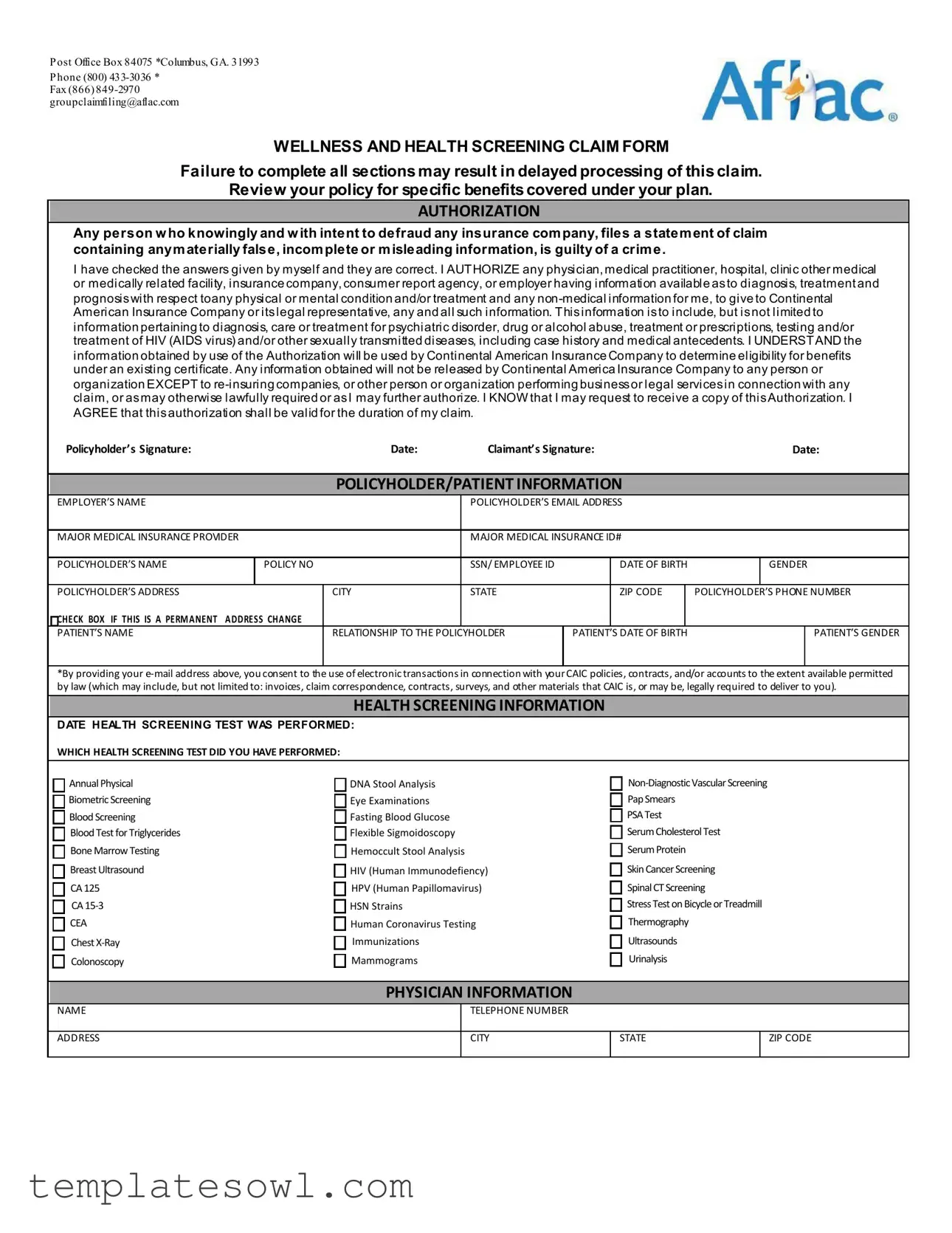
Post Office Box 84075 *Columbus, GA. 31993 Phone (800)
Fax (866)
WELLNESS AND HEALTH SCREENING CLAIM FORM
Failure to complete all sections may result in delayed processing of this claim.
Review your policy for specific benefits covered under your plan.
AUTHORIZATION
Any person who knowingly and with intent to defraud any insurance company, files a statement of claim containing anymaterially false, incomplete or misleading information, is guilty of a crime.
Ihave checked the answers given by myself and they are correct. I AUTHORIZE any physician, medical practitioner, hospital, clinic other medical or medically related facility, insurance company, consumer report agency, or employer having information available asto diagnosis, treatment and prognosiswith respect toany physical or mental condition and/or treatment and any
Policyholder’s Signature:Date:Claimant’s Signature:Date:
POLICYHOLDER/PATIENT INFORMATION
EMPLOYER’S NAME |
|
|
|
POLICYHOLDER’S EMAIL ADDRESS |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
MAJOR MEDICAL INSURANCE PROVIDER |
|
MAJOR MEDICAL INSURANCE ID# |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
POLICYHOLDER’S NAME |
|
POLICY NO |
|
SSN/ EMPLOYEE ID |
|
DATE OF BIRTH |
|
GENDER |
||
|
|
|
|
|
|
|
|
|
|
|
POLICYHOLDER’S ADDRESS |
|
|
CITY |
STATE |
|
ZIP CODE |
|
POLICYHOLDER’S |
PHONE NUMBER |
|
CHECK BOX IF THIS IS A PERMANENT |
ADDRESS CHANGE |
|
|
|
|
|
|
|
|
|
PATIENT’S NAME |
|
|
RELATIONSHIP TO THE POLICYHOLDER |
PATIENT’S DATE OF BIRTH |
|
|
PATIENT’S GENDER |
|||
|
|
|
|
|
|
|
|
|
|
|
*By providing your
HEALTH SCREENING INFORMATION
DATE HEALTH SCREENING TEST WAS PERFORMED:
WHICH HEALTH SCREENING TEST DID YOU HAVE PERFORMED:
Annual Physical
Biometric Screening
Blood Screening
Blood Test for Triglycerides
Bone Marrow Testing
Breast Ultrasound
CA 125
CA
CEA
Chest
Colonoscopy
DNA Stool Analysis |
|
Eye Examinations |
Pap Smears |
Fasting Blood Glucose |
PSA Test |
Flexible Sigmoidoscopy |
Serum Cholesterol Test |
Hemoccult Stool Analysis |
Serum Protein |
HIV (Human Immunodefiency) |
Skin Cancer Screening |
HPV (Human Papillomavirus) |
Spinal CT Screening |
HSN Strains |
Stress Test on Bicycle or Treadmill |
Human Coronavirus Testing |
Thermography |
Immunizations |
Ultrasounds |
Mammograms |
Urinalysis |
PHYSICIAN INFORMATION
NAME
ADDRESS
TELEPHONE NUMBER
CITY
STATE
ZIP CODE
Form Characteristics
| Fact Name | Description |
|---|---|
| Contact Information | The Aflac Wellness form can be submitted via fax at (866) 849-2970 or by email at groupclaimfiling@aflac.com. |
| Submission Address | Send completed forms to Post Office Box 84075, Columbus, GA 31993. |
| Claim Processing | Failure to complete all sections of the form may delay claim processing. |
| Authorization Requirement | Applicants must sign an authorization allowing Aflac to obtain necessary medical information. |
| Legal Compliance | Completing the form accurately is essential to avoid committing potential fraud. |
| State-Specific Regulations | Forms are governed by state insurance laws, which may vary; check local requirements for compliance. |
Guidelines on Utilizing Aflac Wellness
Once you have the Aflac Wellness form, completing it accurately is crucial for efficient processing. Each section requires your attention, from personal details to health screening information. Take your time to fill out all necessary components to ensure timely claims processing.
- Begin by entering the policyholder's name.
- Provide the policyholder’s email address.
- Fill in the employer's name.
- Include the major medical insurance provider and their ID number.
- Input the policy number and social security number or employee ID.
- Enter the date of birth and gender of the policyholder.
- Complete the policyholder’s address, including city, state, and ZIP code.
- List the policyholder’s phone number. If this is a permanent address change, check the appropriate box.
- Next, provide the patient’s name (if different from the policyholder).
- Fill in the patient’s relationship to the policyholder.
- Enter the patient’s date of birth and gender.
- Now, move to the health screening information section. Document the date the health screening test was performed.
- Select the health screening test performed from the provided list.
- Provide the physician’s name.
- Enter the physician’s address, including city, state, and ZIP code.
- Finally, include the physician's telephone number.
What You Should Know About This Form
What is the purpose of the Aflac Wellness form?
The Aflac Wellness form is designed to facilitate the filing of claims for wellness and health screenings under your Aflac insurance policy. By completing this form, policyholders can seek reimbursement for a variety of health screening tests, which may be eligible for benefits based on their specific insurance plan. Ensuring that the form is filled out completely and accurately is critical for timely processing of your claim.
What information do I need to provide on the form?
When filling out the Aflac Wellness form, you must provide comprehensive information about yourself and your health screening. This includes your personal information, such as name, address, and insurance details. You'll also need to indicate the type of health screening you had and the date it was performed. It's important to remember that incomplete sections can lead to delays, so be meticulous in your responses.
How does the authorization section work?
The authorization section grants Aflac permission to access your medical records. By signing this section, you allow physicians, hospitals, and other medical facilities to provide relevant health information to Aflac. This information helps determine your eligibility for benefits. It’s crucial to understand that your medical information will be treated confidentially and shared only with authorized entities involved in processing your claim.
What if I file a claim and fail to provide accurate information?
Filing a claim with inaccurate or misleading information can result in serious consequences, including denial of the claim or potential legal ramifications. Aflac emphasizes the importance of honesty when completing the form. If you realize that you have made an error after submitting a claim, it is advisable to contact Aflac immediately to correct the information and avoid complications.
How can I contact Aflac for assistance with the Wellness form?
If you have questions or need assistance while completing the Aflac Wellness form, you can reach out to Aflac customer service. You can call them at (800) 433-3036 or send a fax to (866) 849-2970. Additionally, for any inquiries via email, contact groupclaimfiling@aflac.com. Aflac representatives are available to help ensure that you successfully submit your claim.
Common mistakes
Completing the Aflac Wellness form correctly is crucial for timely processing of claims. One common mistake individuals make is not filling out all required sections. Each section plays a vital role in substantiating the claim. Missing information can lead to delays or even outright denials of benefit requests.
Another frequent error occurs when individuals omit their policyholder’s information. It is essential to provide accurate details such as the policyholder's name, address, and insurance ID number. Omitting or inaccurately reporting these details can create confusion and complicate the claims process.
People often misstate the health screening information, particularly the date or type of test performed. This section must be precise. Inaccurate dates or incorrect test names lead to misunderstandings that result in delayed processing. It is advisable to double-check this information before submission.
In addition, individuals frequently neglect to sign and date the form properly. Both the policyholder and the claimant must provide their signatures along with the corresponding dates. An unsigned or improperly dated form may be considered incomplete, thus hindering the progress of the claim.
Providing an incorrect email address is another common mistake. The form indicates that the policyholder’s email can be used for electronic transactions. If a wrong email is provided, important communications regarding the claim may be missed, complicating the process further.
Lastly, many people fail to review their policy for specific coverage details. Knowing what benefits are available under the existing plan will help in accurately completing the claim form. It is essential to review the policy to ensure the claimed services are covered.
Documents used along the form
The Aflac Wellness form is an important document for claiming wellness benefits. Several other forms can accompany it to ensure a smooth claim process. Below is a list of common forms and documents often used alongside the Aflac Wellness form.
- Claim Submission Form: This form is used to provide details about the claim being submitted. It includes information about the services received and the expenses involved.
- Authorization to Release Information: This document allows healthcare providers to share a claimant’s medical information with Aflac for processing claims.
- Patient Privacy Notice: This statement outlines how personal health information may be used and disclosed. Claimants receive it from healthcare providers.
- Medical Records Request Form: Patients use this form to request their medical records from healthcare providers or facilities needed for the claim.
- Evidence of Coverage Document: This is an informational document that details the coverage provided by the Aflac plan, including benefits and limitations.
- Healthcare Provider Invoice: This is a detailed statement from a healthcare provider outlining the costs associated with the services rendered.
- Appointment Verification Form: This document verifies attendance at appointments relevant to the wellness claim and may include dates and services performed.
- Diagnosis Certificate: This form provides confirmation of a diagnosis from a healthcare provider and is necessary for some claims.
- Supplemental Insurance Claim Form: If a policyholder has multiple insurance policies, this form helps claim additional benefits directly from another insurance provider.
- Dependent Verification Form: This document verifies eligibility for dependents covered under the policyholder’s Aflac plan, if applicable.
These documents facilitate efficient processing of wellness claims under the Aflac policy. Ensuring these forms are completed accurately can help avoid delays in receiving benefits.
Similar forms
The Aflac Wellness form shares similarities with several other documents commonly used in healthcare and insurance contexts. Each of these documents serves a specific purpose in gathering information relevant to health screenings and claims. Below is a list of documents that are similar in nature:
- Health Insurance Claim Form: Like the Aflac Wellness form, this document collects information about medical services provided to a patient. Both forms require patient information, provider details, and date of service to facilitate accurate processing of claims.
- Patient Authorization Form: This form is similar as it requires a patient’s consent to release medical information. Just as the Aflac Wellness form includes an authorization section for sharing health information, the Patient Authorization Form enables healthcare providers to disclose sensitive patient data to insurance companies.
- Wellness Screening Report: This report is akin to the Aflac Wellness form in that it documents the results of various health screenings. Both emphasize the importance of preventive health measures and contain details about the specific tests performed.
- Medical Records Release Form: Both forms entitle insurance companies or providers to access medical information. The Medical Records Release Form is explicitly designed for this purpose, while the Aflac Wellness form implies a similar access authorization through its language regarding sharing and obtaining medical information.
- Claim Submission Form: This document serves to formally submit a claim for reimbursement. The Aflac Wellness form requires specific health screening information, similar to a Claim Submission Form where details about the medical services or diagnoses are recorded for processing.
Dos and Don'ts
When filling out the Aflac Wellness form, keep the following guidelines in mind:
- Double-check that all sections of the form are completed. Incomplete forms can delay processing.
- Use clear and concise language. This helps avoid misunderstandings.
- Provide accurate personal information, including your Social Security number and birth date.
- Review your policy for specific benefits to ensure you're claiming what you’re entitled to.
- Keep copies of the completed form for your records.
There are also things to avoid when filling out the form:
- Do not submit the form without signing it. Your signature is essential for processing.
- Avoid providing any false or misleading information. This could be considered fraud.
- Do not forget to check your email for correspondence related to your claim.
- Do not leave blank sections, even if the information seems irrelevant. Every section should be completed.
Misconceptions
Understanding the Aflac Wellness form can be tricky. Several misconceptions often arise that can lead to confusion about its purpose and use. Here’s a breakdown of eight common misconceptions:
- The Aflac Wellness form is only for serious illnesses. In reality, this form covers a broad range of health screenings and preventative services. It’s meant to encourage regular health check-ups, not just for serious conditions.
- Filling out the form is optional. While it may seem like a choice, submitting the form is necessary to access specific wellness benefits outlined in your policy. Without it, claims may be delayed or denied.
- You can submit the form any time. Timeliness matters. There are limits on when you can submit a claim after a health screening. Check your plan details for specific deadlines.
- The Aflac Wellness form requires a physician's signature. No signature is needed. Just complete the relevant sections with your information and submit it. However, health provider documentation may be required.
- Aflac automatically processes my claims. Claims processing requires you to proactively submit the wellness form along with any necessary documentation. Make sure all sections are filled out correctly to avoid delays.
- Only the policyholder can fill out the form. Any eligible dependents who undergo health screenings can have their information included. This encourages families to prioritize health care.
- All screenings are covered without exception. Coverage varies based on your specific plan. Always review your benefits to ensure that the tests you receive are eligible for reimbursement.
- Your information is widely shared. The Aflac Wellness form includes a privacy policy to protect your information. It will not be released to unauthorized parties, ensuring confidentiality.
Clearing up these misconceptions can help you and your family make the most of your Aflac benefits. Always refer to your specific policy for the most accurate information regarding coverage.
Key takeaways
Understanding how to successfully fill out and use the Aflac Wellness form can make a significant difference in your claims experience. Here are some essential takeaways:
- Complete All Sections: Ensure every section of the form is filled out completely. Incomplete forms can lead to delays in processing your claims.
- Authorization is Key: You must authorize the release of your medical information. This includes data from your healthcare providers related to physical or mental health.
- Policy Details Matter: Familiarize yourself with your specific policy to understand the benefits that are covered. Knowing this will help you accurately complete the form.
- Keep a Record: A signed copy of the Authorization should be retained for your records. Having this can provide clarity and peace of mind during the claims process.
By keeping these points in mind, you can navigate the claims process more efficiently and make the most of your wellness benefits.
Browse Other Templates
Ss Forms - Abdominal palpation results assist in evaluating fetal positioning.
Audition Forms - Be prepared to share information about your training and instructors.