Fill Out Your Alabama Medicaid Referral Form
The Alabama Medicaid Referral Form (Form 362) is a critical document designed to facilitate communication between primary care physicians, consultants, and Medicaid recipients. It begins with necessary information such as the recipient's name, Medicaid number, and contact details, ensuring a quick connection to the individual involved. The form requires the designation of the primary physician, accompanied by a mandatory original signature, which confirms the authenticity of the referral. In instances where the screening provider differs from the primary physician, their information must also be included. Different categories of referrals are clearly defined, ranging from Patient 1st referrals, EPSDT screenings for children, to case management services. The length and validity of the referral, specifying the number of visits or duration, must be indicated to ensure clarity on the extent of care authorized. Notably, the form stipulates distinct options for referral purpose, whether it be for evaluation, treatment, or outpatient hospital care, and it requires the primary physician to state the reason for the referral. The process is not complete without detailing the consultant’s information and specifying how findings will be communicated back to the primary physician. This structured approach streamlines access to specialized care while upholding the highest standards for patient information management.
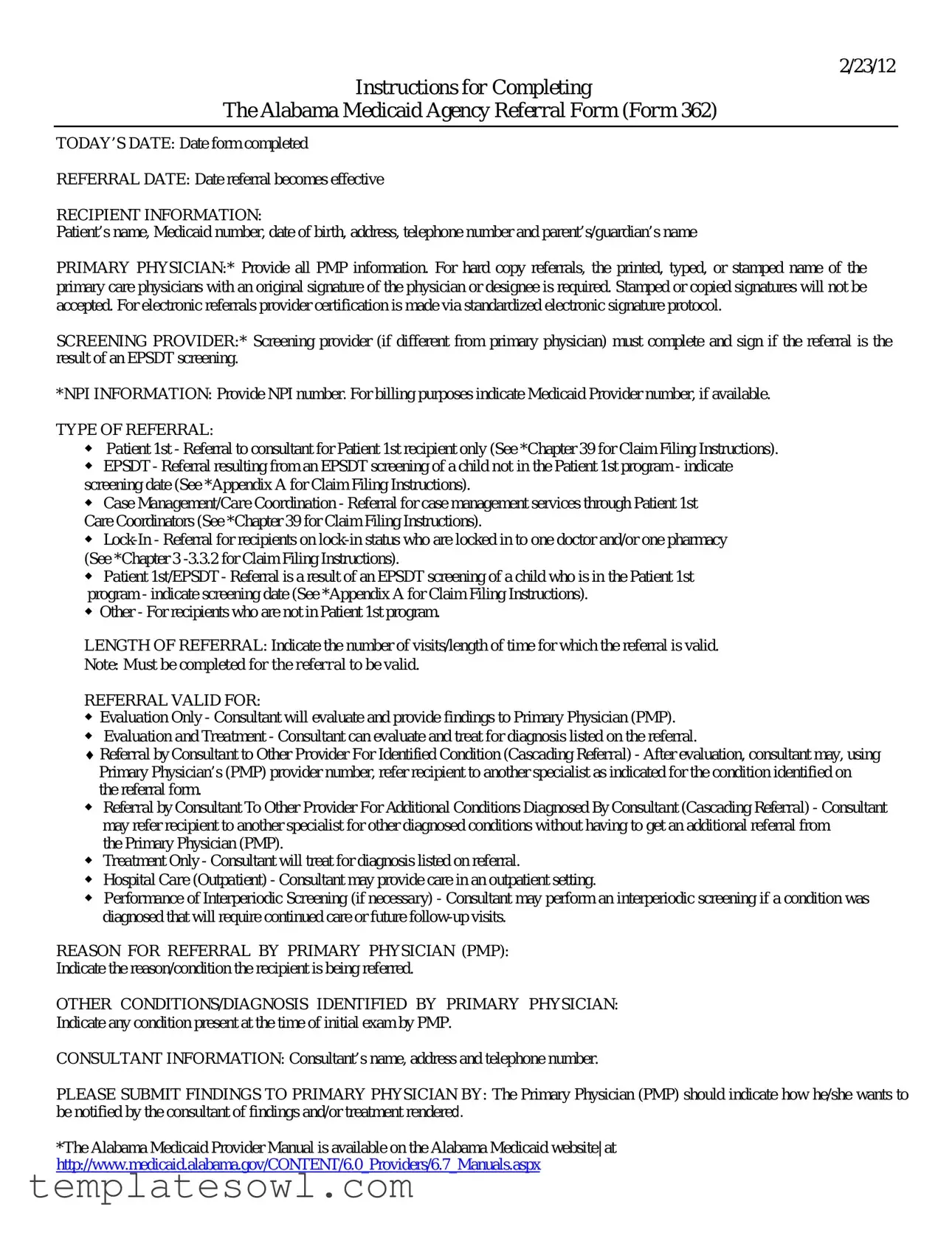
Alabama Medicaid Referral Example
2/23/12
Instructions for Completing
The Alabama Medicaid Agency Referral Form (Form 362)
TODAY’S DATE: Date form completed
REFERRAL DATE: Date referral becomes effective
RECIPIENT INFORMATION:
Patient’s name, Medicaid number, date of birth, address, telephone number and parent’s/guardian’s name
PRIMARY PHYSICIAN:* Provide all PMP information. For hard copy referrals, the printed, typed, or stamped name of the primary care physicians with an original signature of the physician or designee is required. Stamped or copied signatures will not be accepted. For electronic referrals provider certification is made via standardized electronic signature protocol.
SCREENING PROVIDER:* Screening provider (if different from primary physician) must complete and sign if the referral is the result of an EPSDT screening.
*NPI INFORMATION: Provide NPI number. For billing purposes indicate Medicaid Provider number, if available.
TYPE OF REFERRAL:
◆Patient 1st - Referral to consultant for Patient 1st recipient only (See *Chapter 39 for Claim Filing Instructions).
◆EPSDT - Referral resulting from an EPSDT screening of a child not in the Patient 1st program - indicate screening date (See *Appendix A for Claim Filing Instructions).
◆Case Management/Care Coordination - Referral for case management services through Patient 1st
Care Coordinators (See *Chapter 39 for Claim Filing Instructions).
◆
◆Patient 1st/EPSDT - Referral is a result of an EPSDT screening of a child who is in the Patient 1st program - indicate screening date (See *Appendix A for Claim Filing Instructions).
◆Other - For recipients who are not in Patient 1st program.
LENGTH OF REFERRAL: Indicate the number of visits/length of time for which the referral is valid.
Note: Must be completed for the referral to be valid.
REFERRAL VALID FOR:
◆Evaluation Only - Consultant will evaluate and provide findings to Primary Physician (PMP).
◆Evaluation and Treatment - Consultant can evaluate and treat for diagnosis listed on the referral.
♦Referral by Consultant to Other Provider For Identified Condition (Cascading Referral) - After evaluation, consultant may, using
Primary Physician’s (PMP) provider number, refer recipient to another specialist as indicated for the condition identified on the referral form.
◆Referral by Consultant To Other Provider For Additional Conditions Diagnosed By Consultant (Cascading Referral) - Consultant may refer recipient to another specialist for other diagnosed conditions without having to get an additional referral from
the Primary Physician (PMP).
◆Treatment Only - Consultant will treat for diagnosis listed on referral.
◆Hospital Care (Outpatient) - Consultant may provide care in an outpatient setting.
◆Performance of Interperiodic Screening (if necessary) - Consultant may perform an interperiodic screening if a condition was diagnosed that will require continued care or future
REASON FOR REFERRAL BY PRIMARY PHYSICIAN (PMP):
Indicate the reason/condition the recipient is being referred.
OTHER CONDITIONS/DIAGNOSIS IDENTIFIED BY PRIMARY PHYSICIAN:
Indicate any condition present at the time of initial exam by PMP.
CONSULTANT INFORMATION: Consultant’s name, address and telephone number.
PLEASE SUBMIT FINDINGS TO PRIMARY PHYSICIAN BY: The Primary Physician (PMP) should indicate how he/she wants to be notified by the consultant of findings and/or treatment rendered.
*The Alabama Medicaid Provider Manual is available on the Alabama Medicaid website| at http://www.medicaid.alabama.gov/CONTENT/6.0_Providers/6.7_Manuals.aspx

|
|
|
|
ALABAMA MEDICAID REFERRAL FORM |
|
|
Today’s Date _________________ |
|||||||||||||||
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
Date Referral Begins _________________ |
|||||||||||||||||
|
|
|
|
|
Important NPI Information |
|||||||||||||||||
|
|
|
|
|
|
(If different from above) |
||||||||||||||||
MEDICAID RECIPIENT INFORMATION |
See Instructions |
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Recipient Name |
|
|
|
|
Recipient # |
|
|
|
Recipient DOB |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
Telephone # with Area Code |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
Name of Parent/Guardian |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRIMARY PHYSICIAN (PMP) INFORMATION |
|
|
|
|
SCREENING PROVIDER IF DIFFERENT FROM PRIMARY PHYSICIAN (PMP) |
|||||||||||||||||
Name |
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Telephone # with Area Code |
|
|
|
|
|
Telephone # with Area Code |
|
|
||||||||||||||
Fax # with Area Code |
|
|
|
|
|
Fax # with Area Code |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
NPI # |
|
|
|
|
|
|
|
|
NPI # |
|
|
|
|
|
|
|
|
|
||||
Medicaid Provider # |
|
|
|
|
|
Medicaid Provider # |
|
|
|
|
|
|
|
|
|
|||||||
Signature |
|
|
|
|
|
|
|
Signature |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE OF REFERRAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient 1st |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
EPSDT |
Screening Date ______________________ |
|
|
|
|
Other |
|
|
|
|
|
|
|
|
||||||||
Case Management/Care Coordination |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
LENGTH OF REFERRAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Referral Valid for __________ month(s) or __________ visit(s) from date referral begins. |
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REFERRAL VALID FOR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Evaluation Only |
|
|
|
|
Treatment Only |
|
|
|
|
|
|
|
|
|||||||||
Evaluation and Treatment |
|
|
|
|
Hospital Care (Outpatient) |
|||||||||||||||||
Referral by consultant to other provider for identified |
|
|
|
|
Performance of Interperiodic Screening (if necessary) |
|||||||||||||||||
condition (cascading referral)
Referral by consultant to other provider for additional conditions diagnosed by consultant (EPSDT Only)
Reason for referral by PMP |
Other conditions/diagnoses identified by PMP |
CONSULTANT INFORMATION
Consultant Name
Address
Consultant Telephone # with Area Code
Note: Please submit written report of findings including the date of examination/service, diagnosis, and consultant signature to Primary Physician (PMP).
Findings should be submitted to Primary Physician (PMP) by
|
Fax |
In addition, please telephone |
Form 362 |
Alabama Medicaid Agency |
Rev. |
www.medicaid.alabama.gov |
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Title | The form is officially known as the Alabama Medicaid Agency Referral Form (Form 362). |
| Recipient Information | This form requires detailed patient information such as name, Medicaid number, date of birth, and contact details. |
| Primary Physician Requirement | For hard copy submissions, the primary physician must provide a printed, typed, or stamped name along with an original signature; electronic submissions have their own signature protocols. |
| Governing Laws | The Alabama Medicaid Referral Form is governed by regulations outlined in the Alabama Medicaid Provider Manual, which is available on the Alabama Medicaid website. |
Guidelines on Utilizing Alabama Medicaid Referral
If you need to complete the Alabama Medicaid Referral form, it's a straightforward process. This guide walks you through the necessary steps. Make sure to collect all required information beforehand to make the process smooth.
- Write Today's Date: Fill in the date when you are completing the form.
- Enter Referral Date: Indicate the date when the referral will take effect.
- Provide Recipient Information: Include the patient's name, Medicaid number, date of birth, address, telephone number, and the name of the parent or guardian.
- Primary Physician Information: Complete the section with the primary physician's name, address, telephone number, and NPI information. Ensure to include an original signature; stamped signatures are not allowed.
- Screening Provider Information: If the screening provider is different from the primary physician, fill out their name, address, telephone number, and email.
- Choose Type of Referral: Mark the appropriate box for the type of referral: Patient 1st, EPSDT, Case Management/Care Coordination, Lock-In, or Other.
- Length of Referral: Specify the number of months or visits the referral is valid for.
- Referral Valid For: Indicate if the referral is for evaluation only, treatment only, evaluation and treatment, outpatient hospital care, or another relevant option.
- Reason for Referral: Write down the reason or condition necessitating the referral.
- Other Conditions/Diagnoses: List any additional conditions noted by the primary physician during the initial exam.
- Consultant Information: Fill out the consultant's name, address, and telephone number.
- Submission of Findings: Specify how the primary physician wants to receive findings from the consultant: by mail, email, fax, or phone.
What You Should Know About This Form
What is the Alabama Medicaid Referral Form?
The Alabama Medicaid Referral Form, also known as Form 362, is a document used by healthcare providers to refer Medicaid recipients to specialists or consultants for further evaluation and treatment. This form is essential for ensuring that recipients receive appropriate care under Alabama Medicaid guidelines.
How do I complete the form?
To complete the form, you need to fill in basic recipient information like the patient's name, Medicaid number, date of birth, and contact details. Include the primary physician's information and any other healthcare provider involved, if applicable. You must specify the type of referral and provide details on the reason for referral and expected outcomes.
What types of referrals can I indicate on the form?
You can indicate several types of referrals, including Patient 1st, EPSDT screenings, case management, lock-in status, and others. Each type relates to specific circumstances regarding the patient's health and Medicaid status. Be sure to select the one that fits the patient's situation best.
Is a signature required on the form?
A signature from the primary physician (PMP) is required, whether you are submitting a hard copy or an electronic form. For hard copies, the physician must provide an original signature. Stamped signatures are not acceptable. For electronic forms, a standardized electronic signature protocol is used to confirm the referral.
How long is the referral valid?
The referral is valid for a specific length of time, which you will indicate on the form. You can specify the duration in months or the number of visits the referral covers. This must be completed for the referral to be considered valid.
What if the consultant needs to refer the patient to another provider?
If the consultant finds additional conditions needing attention, they can refer the recipient to another provider. This can happen without securing an additional referral from the primary physician if the conditions were diagnosed during the initial evaluation.
How should findings from the consultant be submitted to the primary physician?
The consultant must submit a written report of their findings to the primary physician, which includes details of the services provided, diagnosis, and the consultant's signature. The primary physician can indicate their preferred method for receiving this information, such as through mail, email, fax, or a phone call.
What is the role of the screening provider?
If the referral arises from an EPSDT screening and differs from the primary physician, the screening provider must also complete and sign the form. Their information will be crucial for processing the referral correctly.
Where can I find the Alabama Medicaid Provider Manual?
The Alabama Medicaid Provider Manual is accessible online at the Alabama Medicaid website. This resource provides comprehensive guidelines and instructions related to the Medicaid program and its various forms, including the referral form.
Common mistakes
Filling out the Alabama Medicaid Referral form accurately is essential for ensuring timely and appropriate medical care. Many individuals make mistakes that can lead to delays or denial of services. One common error is not providing TODAY'S DATE or the REFERRAL DATE. These dates are important as they indicate when the form was completed and when the referral becomes effective. Omitting these dates can create confusion and may lead to miscommunication between providers.
Another frequent mistake involves incomplete or inaccurate RECIPIENT INFORMATION. It is vital to include the patient's full name, Medicaid number, date of birth, address, telephone number, and the name of the parent or guardian. Missing or incorrectly formatted information can result in difficulty in processing the referral.
Individuals may also overlook the requirement to provide the full name and signature of the PRIMARY PHYSICIAN. For hard copy referrals, the printed, typed, or stamped name must be accompanied by the physician's original signature. The use of stamped or copied signatures does not meet the requirements, which can cause the referral to be rejected.
Failing to specify the TYPE OF REFERRAL is another common mistake. The referral must clearly indicate if it is for Patient 1st, EPSDT, case management, or other categories. Each type has specific instructions for processing; not identifying the type correctly may lead to further inquiries or delays.
Additionally, the LENGTH OF REFERRAL section is sometimes neglected. This portion requires the individual to indicate the number of visits or duration that the referral is valid. Leaving this blank invalidates the referral, rendering it ineffective for the intended purpose.
Finally, individuals may fail to provide detailed information regarding the REASON FOR REFERRAL and any other conditions or diagnoses identified by the PRIMARY PHYSICIAN. This information is critical in helping consultants understand the context of the referral and proceed accordingly. Without this detail, appropriate care and follow-up may be compromised.
Documents used along the form
The Alabama Medicaid Referral Form is an essential document that helps coordinate healthcare services for recipients. However, it is often used alongside several other important forms and documents to facilitate smooth communication and management of patient care. Below is a brief overview of these related forms.
- Alabama Medicaid Provider Enrollment Form: This form is necessary for healthcare providers wishing to offer services to Medicaid recipients. It collects basic information about the provider and their practice, facilitating their enrollment in the Medicaid program.
- Prior Authorization Request Form: This document must be submitted when a provider wishes to obtain approval from Medicaid before delivering certain healthcare services. It details the medical necessity for the requested services.
- Patient Health Information Release Form: Also known as a HIPAA release form, this document allows healthcare providers to share a patient’s confidential information with other parties involved in their care, ensuring compliance with federal privacy laws.
- EPSDT Screening Form: This form is used for Early and Periodic Screening, Diagnosis, and Treatment for children and adolescents. It is essential for documenting the screenings performed and identifying the need for further care based on those screenings.
- Care Coordination Referral Form: This document aids in arranging additional support for patients needing specialized services. It facilitates communication among providers involved in the patient’s care management.
- Consultation Summary Report: After a consultation, this report summarizes the findings and any recommended treatment. The consultant sends this to the primary physician to keep them updated on the patient’s care plan.
- Medicaid Claim Form: This form is used by providers to bill Medicaid for services rendered to a recipient. It includes all necessary details to ensure timely and accurate processing of claims for reimbursement.
These forms act as vital tools in the effective management of Medicaid services. By understanding the purpose and function of each document, healthcare providers can ensure that they meet the needs of their patients efficiently.
Similar forms
- Patient Referral Form: Like the Alabama Medicaid Referral form, this document facilitates communication between healthcare providers. It typically includes patient details, referral reasons, and necessary signatures, ensuring that the primary physician and the specialist have all pertinent information for effective patient management.
- Consultation Request Form: Similar in purpose, this form is used to request a specialist consultation. It captures patient demographics, the rationale for the consultation, and any relevant medical history, mirroring the Alabama Medicaid form's emphasis on detailed recipient information.
- Pre-authorization Request Form: This document requires healthcare providers to seek approval before certain treatments or tests. Like the Medicaid form, it mandates specific patient information, diagnosis codes, and detailed treatment plans to ensure clarity and compliance with insurance guidelines.
- Continuity of Care Document (CCD): This form provides a comprehensive view of a patient's health history and ongoing treatment plans. Similarities include a focus on patient data and care coordination, helping to maintain consistent care across different providers, much like the Alabama Medicaid Referral form.
- Emergency Medical Referral Form: Used in urgent situations, this form allows for quick patient transfer between healthcare facilities. It includes essential patient information and the reason for the transfer, paralleling the requirement for detailed medical history in the Medicaid referral process.
- Home Health Care Referral Form: This document facilitates the initiation of home health services for eligible patients. It shares similarities in requesting patient details, provider information, and reasons for referral, ensuring appropriate care is delivered at home.
- Specialist Appointment Confirmation Form: This confirms the details of a scheduled appointment with a specialist. Like the Alabama Medicaid Referral form, it requires patient and provider information and communicates important details such as appointment time and purposes of the visit.
Dos and Don'ts
When filling out the Alabama Medicaid Referral form, consider these important guidelines. Following them can ease the process and ensure accuracy.
- Use the correct dates. Clearly specify both the date you complete the form and the date the referral becomes effective.
- Provide complete recipient information. Include the patient’s name, Medicaid number, date of birth, address, telephone number, and the name of the parent or guardian.
- Ensure correct primary physician information. Fill in all relevant details of the primary physician, ensuring the original signature is included.
- Clearly indicate the type of referral. Specify whether the referral is for Patient 1st, EPSDT, or other types clearly.
- Document the length of the referral. State the number of visits or the duration the referral is valid for to avoid confusion.
- Submit findings promptly. Ensure that the consultant submits findings to the primary physician by the desired communication method.
Also, avoid the following common mistakes:
- Don't use copied signatures. Only original signatures will be accepted; stamped or copied ones may lead to rejection.
- Don't leave sections blank. Ensure every required field is filled, as incomplete forms can lead to delays or denials.
- Don't forget to specify additional conditions. If there are other diagnoses, explicitly mention them to ensure comprehensive care.
- Don’t neglect the consultant’s information. Provide the full contact details of the consultant for effective communication.
- Don't overlook privacy concerns. Treat all patient information as confidential and secure.
- Don’t forget to keep a copy. Retain a copy of the completed referral form for your records.
Misconceptions
When dealing with the Alabama Medicaid Referral form, misunderstandings can create unnecessary confusion. Let's clear up some prevalent misconceptions:
- All signatures can be stamped or copied. Only original handwritten signatures are accepted for hard copy referrals. Stamped signatures will not qualify.
- Filling out the form is optional. It's crucial to complete the form accurately; without it, referrals may not be valid.
- The referral is valid for an indefinite time. You must specify the length of the referral, whether it's for a set number of visits or a duration.
- Only primary physicians can make referrals. Secondary screening providers can also complete and sign the referral if they performed an EPSDT screening.
- The referral is the same as a prescription. A referral outlines the need for specialized treatment but does not serve as a prescription for medication.
- All referrals are for treatment only. Some referrals are simply for evaluation; it's essential to indicate the purpose clearly on the form.
- Once a referral is made, no further documentation is needed. Consultants must provide findings back to the primary physician, including the details of the visit and diagnosis.
- Electronic referrals don't need any signatures. Even for these, appropriate electronic signature protocols must be followed to ensure validity.
- All types of referrals have the same process. There are different categories, and each has specific requirements and instructions that need to be adhered to.
- Using the wrong form has no consequences. Submitting an incorrect or incomplete form can lead to denials of services, so accuracy is vital.
By understanding these misconceptions, patients and providers can navigate the Alabama Medicaid Referral process more seamlessly, ensuring timely and effective healthcare services.
Key takeaways
When dealing with the Alabama Medicaid Referral Form, understanding its components is crucial. Here are some key takeaways that can streamline the process:
- Correct Completion Is Essential: The form requires detailed recipient information, including the patient's name, Medicaid number, and contact details. Incomplete or inaccurate information can delay referrals, so careful attention is vital.
- Signature Requirements: The primary physician's signature must be original. Stamped or copied signatures will not be accepted, whether the referral is submitted on paper or through electronic means. Compliance with this requirement is non-negotiable.
- Type and Length of Referral Matter: Clearly indicate the type of referral (e.g., Patient 1st, EPSDT) and specify the length of time for which the referral is valid. This ensures that the consultant understands the scope and timeline of the needed services.
- Communication of Findings: The form allows the primary physician to specify how they want to receive findings from the consultant. Options include mail, email, or fax. Clearly indicating a preferred communication method helps facilitate timely coordination of care.
Browse Other Templates
Fbi Background Check for Visa - You can submit the I-783 form by mail along with a fingerprint card.
Standard Form 25a - Information about the issuance or denial of a license can be shared with other licensing authorities.