Fill Out Your Anesthesia Record Form
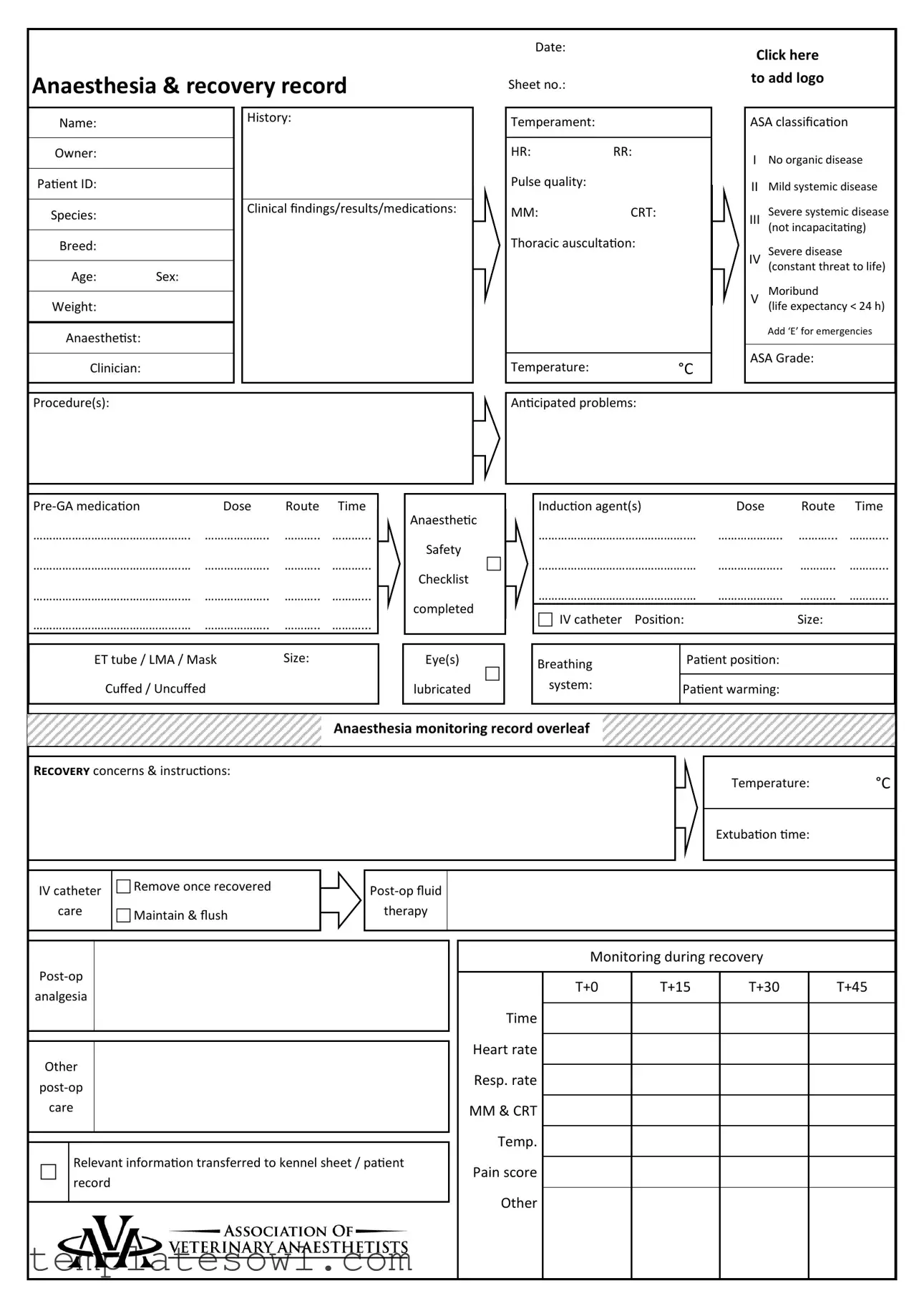
The Anesthesia Record form is a crucial document used in veterinary and medical settings to ensure the safe administration of anesthesia during various procedures. It captures essential patient information such as name, ID, age, breed, and weight, which helps in assessing the patient’s suitability for anesthesia. The form also includes classifications like the ASA classification system, which identifies the patient's overall health status and any potential complications that could arise during the process. A comprehensive pre-anesthetic evaluation details the patient’s medical history, temperament, and results from clinical examinations. Additionally, it outlines the specific anesthesia protocols employed, including the types and doses of medications administered, and records vital signs throughout the procedure. The document provides space for notes regarding monitoring during recovery, including heart rate, respiratory rate, and temperature, helping clinicians identify any issues that may arise post-anesthesia. By documenting all these details meticulously, the Anesthesia Record form not only enhances patient safety but also serves as an essential communication tool for the healthcare team throughout the patient’s care journey.
Anesthesia Record Example

Anaesthesia & recovery record
Date:
Sheet no.:
Click here
to add logo
Name:
History:
Temperament:
ASA classification
Owner:
Patient ID:
HR:RR:
Pulse quality:
INo organic disease
IIMild systemic disease
Species:
Clinical findings/results/medications:
MM: |
CRT: |
Severe systemic disease
III
(not incapacitating)
Breed:
Age: Sex:
Weight:
Anaesthetist:
Clinician:
Thoracic auscultation: |
Temperature:°C
Severe disease
IV
(constant threat to life)
Moribund
V
(life expectancy < 24 h)
Add ‘E’ for emergencies
ASA Grade:
Procedure(s):
Anticipated problems:
|
|
|
Dose |
Route Time |
|
…………………………………………. |
……………….. |
……….. ………... |
……………………………………….… |
……………….. |
……….. ………... |
……………………………………….… |
……………….. |
……….. ………... |
……………………………………….… |
……………….. |
……….. ………... |
|
|
|
ET tube / LMA / Mask |
Size: |
|
Cuffed / Uncuffed |
|
|
|
|
|
Anaesthetic
Safety
Checklist
completed
Eye(s)
lubricated
|
|
|
|
|
|
|
Induction agent(s) |
|
Dose |
Route |
Time |
|
……………………………………….… |
……………….. |
………... |
………... |
|
|
……………………………………….… |
……………….. |
……….. |
………... |
|
|
……………………………………….… |
……………….. |
……….. |
………... |
|
|
IV catheter Position: |
|
Size: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Breathing |
Patient position: |
|
|
|
|
|
|
|
|
|
|
system: |
Patient warming: |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Anaesthesia monitoring record overleaf
Recovery concerns & instructions:
Temperature: °C
Extubation time:
IV catheter
care
Remove once recovered
Maintain & flush
therapy
analgesia
Other
care
Relevant information transferred to kennel sheet / patient record
Monitoring during recovery
|
T+0 |
T+15 |
T+30 |
T+45 |
Time |
|
|
|
|
|
|
|
|
|
Heart rate |
|
|
|
|
|
|
|
|
|
Resp. rate |
|
|
|
|
|
|
|
|
|
MM & CRT |
|
|
|
|
|
|
|
|
|
Temp. |
|
|
|
|
|
|
|
|
|
Pain score |
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Start procedure: |
Finish procedure: |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Throat pack |
Placed |
|
|
Removed |
||||||
|
|
Notes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
volume |
|
Total |
……………..………ml |
|
Dog |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10% |
……………..………ml |
85ml/kg |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Blood |
|
20% |
……………..………ml |
Cat / Rabbit |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
30% |
……………..………ml |
55ml/kg |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Notes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Key |
|
240 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
230 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HR |
● |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
220 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
o |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RR |
210 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
IPPV |
ø |
200 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
190 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
SAP |
˅ |
180 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
MAP |
– |
170 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
160 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
DAP |
˄ |
150 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
140 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Doppler |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
130 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
120 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Palpebral reflex |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
110 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Jaw tone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
100 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
90 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
80 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
70 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Eye position |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
60 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
↓ / → |
|
50 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
40 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
30 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Iso / Sevo |
|
% |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O2 / N2O / Air |
L/min |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Palpebral reflex |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Swabs |
|
|
|
|
|
Sharps |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Eye position |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
In |
|
Out |
|
|
|
In |
|
Out |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Jaw tone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pulse quality |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ETCO2 |
|
kPa/mmHg |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SpO2 |
|
% |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Temperature |
°C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose | The Anesthesia Record form is designed to document patient information, history, and details of anesthesia care during veterinary procedures. |
| Required Information | Essential data includes patient ID, ASA classification, vital signs, and medications used. This ensures comprehensive monitoring and care records. |
| State-Specific Laws | In California, the Veterinary Medicine Practice Act governs the necessity and requirements of anesthesia record-keeping to ensure patient safety and compliance. |
| Patient Safety | The form includes an Anaesthetic Safety Checklist which must be completed prior to any anaesthesia administration to mitigate risks. |
| Legal Importance | Accurate documentation through the Anesthesia Record form can serve as vital evidence in case of disputes or malpractice claims, reinforcing the standard of care provided. |
Guidelines on Utilizing Anesthesia Record
Filling out the Anesthesia Record form requires precise attention to detail. Each section captures critical information about the patient, the anesthesia administered, and the monitoring that occurs throughout the procedure. Though straightforward, it is vital to follow each step properly to ensure safety and comprehensive documentation.
- Date: Write the date of the procedure.
- Sheet no: Enter the sheet number for tracking purposes.
- Name: Fill in the patient’s name.
- Owner: Record the owner's name.
- Patient ID: Input the unique identification number for the patient.
- Species: Indicate the species of the patient.
- Breed: Specify the breed of the patient.
- Age: Note the age of the patient.
- Sex: Enter the sex of the patient.
- Weight: Document the weight of the patient in appropriate units.
- Temperament: Describe the patient’s temperament.
- ASA classification: Select the appropriate ASA grade indicating the patient's health status.
- HR: Note the heart rate of the patient.
- RR: Write down the respiratory rate.
- Pulse quality: Describe the quality of the pulse.
- Clinical findings/results/medications: List any relevant clinical observations and medications administered.
- Thoracic auscultation: Note findings from the thoracic auscultation.
- Temperature: Record the patient’s temperature.
- Procedure(s): Identify the procedure being performed.
- Pre-GA medication: List pre-operative medications, including dose, route, and time.
- Induction agent(s): Document induction agents used, including their dose, route, and time.
- ET tube / LMA / Mask: Indicate the size and type (cuffed/un-cuffed) used.
- Patient position: Note the position of the patient for the procedure.
- IV catheter: Document the position and size of any IV catheter placed.
- Recovery concerns & instructions: Outline any concerns and instructions for recovery.
- Monitoring during recovery: Record heart rate, respiratory rate, and other vital signs at specified intervals.
- Start and finish procedure: Document the start and end times of the procedure.
- Throat pack: Note the placement and removal of throat packs.
- Notes: Include any additional comments or information relevant to the anesthesia process.
What You Should Know About This Form
What is the purpose of the Anesthesia Record form?
The Anesthesia Record form is crucial for documenting all aspects of a patient's anesthesia during surgical procedures. It serves as a comprehensive record of the patient’s history, classification, medications administered, monitoring during anesthesia, and recovery details. This documentation ensures continuity of care and helps in evaluating the anesthesia process both during and after the procedure.
What information is included in the Anesthesia Record?
The form contains various essential details such as the date, patient identification, and history. It also includes the patient's ASA classification, vital signs (like heart rate, respiratory rate, and temperature), medications given, anesthesia techniques used, and recovery instructions. Additional sections cover anticipated problems, monitoring records, and notes on fluid volume administered, ensuring a complete and thorough documentation of the anesthesia process.
How does the ASA classification impact patient management?
The ASA (American Society of Anesthesiologists) classification assesses the physical status of the patient prior to anesthesia. Ranging from ASA I (healthy) to ASA V (moribund), this classification helps clinicians make informed decisions regarding the anesthesia plan and the potential risks involved. A higher ASA classification often indicates a need for more intensive monitoring and care throughout the procedure and recovery.
Why is patient monitoring important during anesthesia?
Monitoring is vital for ensuring patient safety during anesthesia. The Anesthesia Record provides space for tracking critical parameters such as heart rate, respiratory rate, temperature, and pain levels at various intervals. This ongoing assessment allows the anesthetist to quickly identify any potential complications and respond accordingly, ultimately improving patient outcomes and minimizing risks.
What are the instructions for recovery mentioned in the Anesthesia Record?
Recovery instructions in the Anesthesia Record form guide post-operative care. These may include temperature monitoring, IV catheter management, and post-operative fluid therapy. The form also details analgesia and any other special care that the patient may require after being extubated, ensuring a smooth recovery process tailored to the individual’s needs.
How should I use the Anesthesia Record form in practice?
Proper use of the Anesthesia Record form involves accurately documenting information before, during, and after the surgical procedure. Fill out the patient's details, including history and ASA classification, before anesthesia begins. During the procedure, record all medications and vital signs diligently. After the procedure, complete the recovery instructions and ensure all data is transferred to necessary records. Thorough completion of the form is essential for quality patient care and compliance with best practice standards.
Common mistakes
Filling out the Anesthesia Record form requires careful attention to detail. One common mistake is providing incomplete patient information. Each section of the form must include full details, such as owner, breed, age, and patient ID. Omitting any of this information can lead to confusion and potential medical errors.
Another frequent error involves the ASA classification. It is crucial to assign the correct ASA grade based on the patient's current health status. Misclassifying a patient can affect anesthesia management and postoperative care.
Many individuals also forget to document pre-anesthetic medication dosages and routes accurately. This oversight can compromise the effectiveness of the medication and the safety of the patient during the procedure.
Additionally, failing to note the induction agents used is a mistake that can have serious implications. Each agent should be clearly recorded with its dose and route, ensuring every detail is accounted for to maintain patient safety.
Monitoring details are often inadequately recorded, particularly during the recovery phase. Consistent updates on the patient's heart rate, respiratory rate, and pain score are vital to assess their recovery accurately. Missing these important observations may lead to oversight of critical changes in the patient's condition.
Another area of concern is the **Anesthetic Safety Checklist**. This checklist is designed to prevent lapses in safety protocols. Neglecting to complete this section can result in increased risks during anesthesia.
Improper documentation of the extubation process is also common. Recording the extubation time and any subsequent recovery care is essential. This information helps ensure that all necessary post-operative care is provided adequately.
Finally, failing to transfer relevant information to the kennel sheet or patient record is a mistake that disrupts continuity of care. Ensuring that all data is accurately communicated among team members promotes better outcomes for patients.
Documents used along the form
When conducting anesthesia for patients, several forms and documents work in conjunction with the Anesthesia Record form. Each of these documents plays a crucial role in ensuring the safety and effective management of the patient during procedures. Below is a list of these related forms and documents.
- Pre-Anesthetic Evaluation Form: This document provides a comprehensive assessment of the patient’s medical history, including any pre-existing conditions and current medications which may affect anesthesia. It is crucial for determining the appropriate anesthetic protocol.
- Informed Consent Form: This form ensures that the owner is fully informed about the risks and benefits associated with the anesthesia and the procedure being performed. It requires the owner’s signature, indicating their agreement to proceed.
- Emergency Response Plan: This document outlines the steps to take in the event of an anesthesia-related emergency. It includes protocols for resuscitation and communication with the veterinary team, ensuring quick action can be taken when necessary.
- Patient Monitoring Record: This form documents vital signs and other relevant data during anesthesia. This ongoing record tracks heart rate, respiratory rate, and other critical parameters to ensure the patient remains stable throughout the procedure.
- Post-Operative Care Instructions: This document provides essential care guidelines for the patient's recovery period. It includes instructions on monitoring the patient at home, potential complications to watch for, and follow-up appointments.
- Anesthetic Drug Administration Log: This log records all medications given during the procedure, including doses and administration routes. It provides an account of what substances were used, which is vital for patient safety and legal documentation.
- Discharge Summary: After the procedure, this summary provides the owner with a detailed report of the anesthesia and surgical procedure. It includes recovery observations as well as any further treatment or follow-up required.
These forms collectively enhance the safety and efficiency of anesthesia practice. Proper documentation is essential not only for legal compliance but also for fostering clear communication among the veterinary team and with pet owners. Adhering to these procedures contributes to better patient outcomes.
Similar forms
- Surgical Consent Form: Similar to the Anesthesia Record, this document records patient information, surgical procedures, and consent details. Both forms ensure that relevant medical history is noted and that consent for anesthesia and surgery is obtained from the owner.
- Preoperative Assessment Form: This form gathers comprehensive details about the patient’s medical history and current health status, just like the Anesthesia Record. Both documents help in identifying potential risks and planning for anesthesia management.
- Monitoring Record: The Monitoring Record is used to capture vital signs throughout a procedure. Just like the Anesthesia Record, it tracks heart rate, respiratory rate, and other critical parameters for patient safety.
- Medication Administration Record (MAR): This document details the medications given to the patient, including dosages and routes. Similar to the Anesthesia Record, it ensures that medication administration is documented clearly and accurately during the procedure.
- Recovery Record: The Recovery Record focuses on the patient's condition after the procedure. It parallels the Anesthesia Record by noting vital signs and recovery instructions, ensuring continuity of care from anesthesia to recovery.
- Emergency Protocols Document: This document outlines protocols for managing emergencies during a procedure. Like the Anesthesia Record, it emphasizes preparedness and outlines potential problems to be anticipated during anesthesia.
- Veterinary Clinical Notes: Clinical notes provide a narrative of the patient’s overall health and treatment plan. Comparable to the Anesthesia Record, these notes capture significant information about the patient’s history, procedures performed, and outcomes.
- Owner Communication Log: This form documents conversations with the pet owner regarding care and treatment. Similar to the Anesthesia Record in its emphasis on communication, it ensures the owner is kept informed about the patient's status and care decisions during anesthesia and recovery.
Dos and Don'ts
When filling out the Anesthesia Record form, attention to detail is crucial. Here’s a guide of things you should and should not do:
- Do ensure all patient information is complete and accurate, including name, breed, age, and weight.
- Do classify the ASA correctly based on the patient’s health status.
- Do document all pre-GA medications, including doses and routes of administration.
- Do record vital signs continuously during the procedure.
- Do complete the Anaesthetic Safety Checklist before starting any procedure.
- Don’t skip over any sections, even if they seem unimportant.
- Don’t use abbreviations that aren’t commonly understood.
- Don’t forget to note any anticipated problems related to the procedure.
- Don’t leave the form incomplete, especially in the recovery section.
Misconceptions
Understanding the Anesthesia Record form is essential for anyone involved in veterinary anesthesia. However, misconceptions can often cloud its true purpose and importance. Below are some common misconceptions, clearly explained.
- It’s just a checklist. Many view the Anesthesia Record as merely a checklist, but it's a comprehensive document that captures vital information about the patient's health, procedure details, and anesthesia management throughout the process.
- All patients are evaluated the same way. The record allows for individualized patient assessments. Each animal's history, temperament, and ASA classification are documented to tailor the anesthesia plan according to its specific needs.
- Temperature is unimportant during anesthesia. Temperature monitoring is critical. Anesthesia can affect a patient’s ability to regulate temperature, and maintaining normothermia is essential for recovery.
- Only one anesthetist fills out the record. It is common for multiple team members to contribute to the Anesthesia Record, ensuring comprehensive monitoring and recording of all aspects during the procedure.
- Recovery concerns are not a priority. Recovery instructions and concerns are clearly documented. This helps guide post-operative care and ensures a smooth recovery process for the patient.
- The monitoring data is not necessary. The monitoring data recorded during anesthesia is crucial. It provides a real-time overview of the patient’s physiological status and helps guide decisions during the procedure.
- This form is only for dogs and cats. While many are familiar with canine and feline anesthesia, the Anesthesia Record is applicable to all species, including rabbits and other small mammals, which also require careful monitoring.
- Post-operative care is just a formality. The record emphasizes the importance of detailed post-operative care. This includes pain management and fluid therapy, which can significantly impact recovery.
- Once signed, the record is no longer relevant. The Anesthesia Record serves as a valuable document for future reference. It provides historical data that can inform future anesthesia protocols for the same patient.
By clearing up these misconceptions, veterinary teams can better utilize the Anesthesia Record to enhance patient safety and care quality.
Key takeaways
Filling out and utilizing the Anesthesia Record form is a crucial part of ensuring patient safety and proper documentation during anesthesia procedures. Here are key takeaways to consider:
- Accurate Patient Information: Ensure that all details related to the patient, including name, history, breed, age, sex, and weight, are filled in correctly. This information is essential for tailored care.
- ASA Classification: Assign an ASA classification to assess the patient’s physical status. This system helps in deciding the appropriate anesthesia approach.
- Complete Pre-GA Medication Details: Document the type, dose, route, and time of any pre-anesthesia medication used. This ensures that all necessary treatments are tracked and can be revisited as needed.
- Anesthetic Safety Checklist: Always complete the anesthesia safety checklist. This checklist can help to identify potential risks before starting the procedure.
- Monitoring Records: Keep detailed records of vital signs during the procedure. Monitoring heart rate, respiratory rate, and temperature at different time intervals helps assess the patient’s stability.
- Recovery Instructions: Clearly outline recovery concerns and post-operative care instructions. These are essential for ensuring a smooth recovery for the patient.
- Transfer of Information: Relevant details must be transferred to the kennel sheet or patient record, ensuring continuity of care and communication among the veterinary team.
These takeaways highlight the importance of thoroughness and attention to detail when filling out the Anesthesia Record form. Proper documentation supports better patient outcomes and enhances the safety of anesthesia procedures.
Browse Other Templates
Sgs Certified Meaning - Check the IEC 62321 Ed.1 standards for various contaminant tests provided.
Invisalign Case Transfer Form - Each healthcare provider is expected to handle patient information with care and confidentiality.
Delta Bag Fee - Claimants must indicate if the case was reported to customs officials.