Fill Out Your Asam Level Of Care Cheat Sheet Form
The ASAM Level of Care Cheat Sheet form is an essential tool designed to aid professionals in evaluating and determining the appropriate level of care for individuals seeking treatment for substance use and mental health disorders. Utilizing the ASAM Adult Patient Placement Criteria, this form helps in assessing six critical dimensions of a client’s needs, starting with immediate emergency requirements and then progressing to the least intensive level of care that can still effectively support the client’s goals. The form outlines various levels of care, ranging from outpatient services to inpatient hospitalization, each with specific admission criteria and service levels. By systematically rating clients based on their withdrawal potential, biomedical conditions, emotional stability, motivation for treatment, relapse potential, and recovery environment, it ensures a comprehensive understanding of the patient’s situation. This structured approach facilitates the decision-making process, ensuring that individuals receive the appropriate interventions tailored to their unique needs, ultimately promoting a higher chance of successful outcomes in their recovery journey.
Asam Level Of Care Cheat Sheet Example

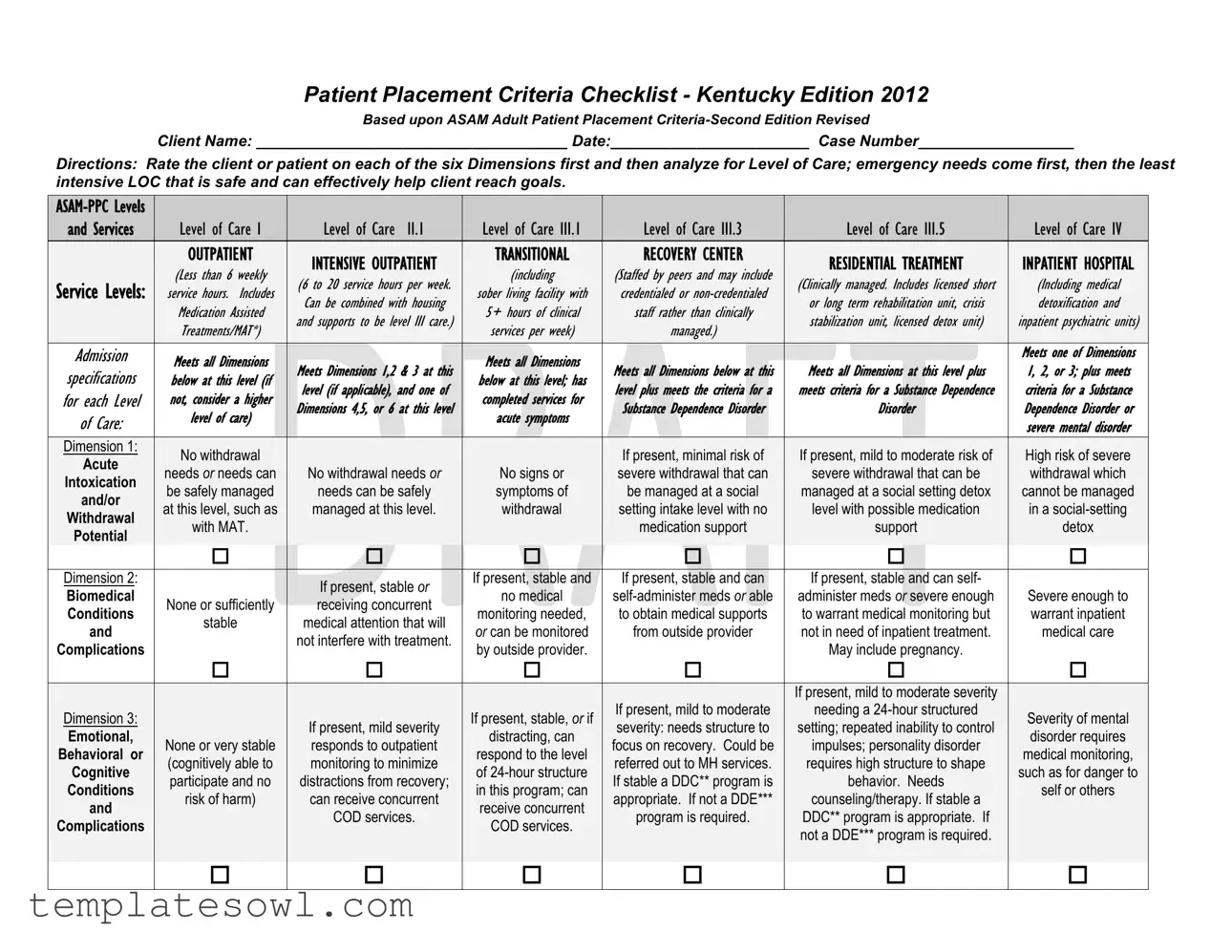
Patient Placement Criteria Checklist - Kentucky Edition 2012
Based upon ASAM Adult Patient Placement
Client Name: ____________________________________ Date:_______________________ Case Number__________________
Directions: Rate the client or patient on each of the six Dimensions first and then analyze for Level of Care; emergency needs come first, then the least intensive LOC that is safe and can effectively help client reach goals.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
and Services |
|
|
Level of Care I |
|
|
Level of Care |
II.1 |
|
|
Level of |
Care III.1 |
|
|
Level of |
Care III.3 |
|
|
Level of Care III.5 |
|
|
Level of |
Care IV |
|
|||||||
|
|
|
|
OUTPATIENT |
|
|
|
|
|
|
|
|
TRANSITIONAL |
|
|
RECOVERY CENTER |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
INTENSIVE OUTPATIENT |
|
|
|
|
RESIDENTIAL TREATMENT |
|
|
INPATIENT HOSPITAL |
|
||||||||||||||||
|
|
|
|
(Less |
than 6 |
weekly |
|
|
|
|
|
(including |
|
|
(Staffed by peers and may include |
|
|
|
|
|
|||||||||||
|
Service Levels: |
|
|
|
|
(6 to 20 service hours per week. |
|
|
|
|
|
|
|
(Clinically managed. Includes licensed short |
|
|
(Including medical |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
service |
hours. |
Includes |
|
|
|
|
sober |
living |
facility with |
|
|
credentialed or |
|
|
|
|
|
|||||||||||
|
|
|
|
|
Can be combined |
with |
housing |
|
|
|
|
or long term |
rehabilitation |
unit, crisis |
|
|
detoxification and |
|
|||||||||||||
|
|
|
|
Medication Assisted |
|
|
|
|
5+ |
hours |
of clinical |
|
|
staff rather |
than clinically |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
and supports to be |
level |
III care.) |
|
|
|
|
|
|
stabilization |
unit, licensed |
detox unit) |
|
|
inpatient psychiatric units) |
|
||||||||||
|
|
|
|
Treatments/MAT*) |
|
|
|
|
services per week) |
|
|
managed.) |
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Admission |
|
|
Meets |
all Dimensions |
|
|
|
|
|
|
|
Meets all |
Dimensions |
|
|
|
|
|
|
|
|
|
|
Meets one of Dimensions |
||||||
|
|
|
|
|
Meets Dimensions 1,2 & 3 at this |
|
|
Meets all Dimensions below at this |
|
Meets all Dimensions at this level plus |
|
1, 2, or 3; plus meets |
|||||||||||||||||||
|
specifications |
|
|
below |
at this |
level (if |
|
|
below |
at this level; has |
|
|
|
||||||||||||||||||
|
for each Level |
|
|
not, consider |
a higher |
|
level (if applicable), |
and one of |
|
completed |
services for |
|
level plus meets |
the criteria for a |
|
meets criteria for a Substance Dependence |
|
criteria for |
a Substance |
||||||||||||
|
|
|
|
Dimensions 4,5, or |
6 at this level |
|
|
Substance Dependence Disorder |
|
|
Disorder |
|
|
|
Dependence |
Disorder or |
|||||||||||||||
|
of Care: |
|
|
level of care) |
|
|
acute symptoms |
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
severe mental disorder |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Dimension 1: |
|
|
No withdrawal |
|
|
|
|
|
|
|
|
|
|
|
|
|
If present, minimal risk of |
|
|
If present, mild to moderate risk of |
|
|
High risk of severe |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Acute |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
needs OR needs can |
|
|
No withdrawal needs OR |
|
|
No signs or |
|
|
severe withdrawal that can |
|
|
severe withdrawal that can be |
|
|
withdrawal which |
|
||||||||||||
|
Intoxication |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
be safely managed |
|
|
needs can be safely |
|
|
symptoms of |
|
|
be managed at a social |
|
|
managed at a social setting detox |
|
|
cannot be managed |
|
||||||||||||
|
and/or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
at this level, such as |
|
|
managed at this level. |
|
|
withdrawal |
|
|
setting intake level with no |
|
|
level with possible medication |
|
|
in a |
|
||||||||||||
|
Withdrawal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
with MAT. |
|
|
|
|
|
|
|
|
|
|
|
|
|
medication support |
|
|
|
support |
|
|
|
detox |
|
|||||
|
Potential |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Dimension 2: |
|
|
|
|
|
|
|
If present, stable OR |
|
If present, stable and |
|
If present, stable and can |
|
If present, stable and can self- |
|
|
|
|
||||||||||||
|
Biomedical |
|
|
|
|
|
|
|
|
no medical |
|
|
administer meds OR severe enough |
|
Severe enough to |
||||||||||||||||
|
|
|
None or sufficiently |
|
receiving concurrent |
|
|
|
|
||||||||||||||||||||||
|
Conditions |
|
|
|
|
monitoring needed, |
|
to obtain medical supports |
|
to warrant medical monitoring but |
|
warrant inpatient |
|||||||||||||||||||
|
|
|
|
stable |
|
medical attention that will |
|
|
|
|
|||||||||||||||||||||
|
and |
|
|
|
|
|
OR can be monitored |
|
from outside provider |
|
not in need of inpatient treatment. |
|
medical care |
||||||||||||||||||
|
|
|
|
|
|
|
|
not interfere with treatment. |
|
|
|
|
|||||||||||||||||||
|
Complications |
|
|
|
|
|
|
|
|
by outside provider. |
|
|
|
|
|
May include pregnancy. |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If present, mild to moderate severity |
|
|
|
|
|
||
|
Dimension 3: |
|
|
|
|
|
|
|
|
|
|
|
|
|
If present, stable, OR if |
|
|
If present, mild to moderate |
|
|
needing a |
|
|
Severity of mental |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
If present, mild severity |
|
|
|
severity: needs structure to |
|
|
setting; repeated inability to control |
|
|
||||||||||||||
|
Emotional, |
|
|
|
|
|
|
|
|
|
distracting, can |
|
|
|
|
|
|
disorder requires |
|
||||||||||||
|
|
|
None or very stable |
|
|
responds to outpatient |
|
|
|
|
focus on recovery. Could be |
|
|
impulses; personality disorder |
|
|
|
||||||||||||||
|
Behavioral or |
|
|
|
|
|
|
respond to the level |
|
|
|
|
|
|
medical monitoring, |
|
|||||||||||||||
|
|
|
(cognitively able to |
|
|
monitoring to minimize |
|
|
|
|
referred out to MH services. |
|
|
requires high structure to shape |
|
|
|
||||||||||||||
|
Cognitive |
|
|
|
|
|
|
of |
|
|
|
|
|
|
such as for danger to |
|
|||||||||||||||
|
|
|
participate and no |
|
|
distractions from recovery; |
|
|
|
|
If stable a DDC** program is |
|
|
behavior. Needs |
|
|
|
||||||||||||||
|
Conditions |
|
|
|
|
|
|
in this program; can |
|
|
|
|
|
|
self or others |
|
|||||||||||||||
|
|
|
risk of harm) |
|
|
can receive concurrent |
|
|
|
|
appropriate. If not a DDE*** |
|
|
counseling/therapy. If stable a |
|
|
|
||||||||||||||
|
and |
|
|
|
|
|
|
receive concurrent |
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
COD services. |
|
|
|
|
program is required. |
|
|
DDC** program is appropriate. If |
|
|
|
|
|
||||||||||
|
Complications |
|
|
|
|
|
|
|
|
|
COD services. |
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
not a DDE*** program is required. |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
CLIENT NAME:________________________________________________ DATE: _____________________ CASE NUMBER:________________________ ____
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Level of Care I |
|
|
Level of |
Care |
II.1 |
|
|
Level of |
Care III.1 |
|
|
Level of Care III.3 |
|
|
|
Level of Care III.5 |
|
Level of Care IV |
|
|||||||
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
OUTPATIENT |
|
|
INTENSIVE OUTPATIENT |
|
|
|
Transitional |
|
|
RECOVERY CENTER |
|
|
RESIDENTIAL TREATMENT |
|
INPATIENT HOSPITAL |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
(Less |
than 6 |
weekly |
|
|
(6 to |
20 service hours per |
|
|
|
(including |
|
|
(Staffed by peers and may include |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
(Clinically |
managed. Includes |
licensed short |
|
(Including medical |
|
||||||||||||
|
Service Levels: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
service |
hours. |
Includes |
|
|
week. Can |
be combined |
|
|
sober |
living |
facility with |
|
|
credentialed or |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
or long |
term |
rehabilitation |
unit, crisis |
|
detoxification and |
|
|||||||||||||
|
|
|
|
Medication Assisted |
|
|
with |
housing |
and |
supports |
|
|
5+ |
hours |
of |
clinical |
|
|
staff rather than clinically |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
stabilization |
unit, licensed |
detox unit) |
|
inpatient psychiatric units) |
|
|||||||||||||
|
|
|
|
Treatments/MAT*) |
|
|
to |
be level III |
care.) |
|
|
services per |
week) |
|
|
managed.) |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
Ready to change and |
|
Has marked difficulty with or |
|
|
Willing to cooperate |
Resistance is high |
Has little awareness & needs |
opposition to treatment, with |
||
|
cooperate at this |
|||||
|
or is ambivalent and |
enough to require |
interventions available only |
dangerous consequences; or there |
||
Dimension 4: |
level, OR externalizes |
|||||
needs motivation, |
structured program, |
at this level to engage & stay |
is high severity in this dimension but |
|||
Readiness to |
problems and needs |
|||||
recovery support, |
but not so high as to |
in recovery. May have |
not others. The client therefore |
|||
Change |
this level of structure, |
|||||
and monitoring |
render outpatient |
external leverage to support |
needs a motivational enhancement |
|||
|
motivation and |
|||||
|
strategies |
treatment ineffective. |
participation. |
program with 24 hour structure. |
||
|
support. |
|||||
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Has little awareness & needs |
|
|
|
|
|
|
|
|
|
|
|
Intensification of |
|
|
Client is at high risk |
|
intervention available only at |
|
Has little awareness & needs |
|
|
|
|
|
|
Able to maintain |
|
|
|
|
for imminent relapse |
|
this level to prevent |
|
intervention available only at this |
|
|
|
|
|
|
|
|
|
symptoms despite |
|
|
|
|
|
|
||||
|
Dimension 5: |
|
abstinence and |
|
|
|
|
with dangerous |
|
continued use, with |
|
level to prevent continued use, with |
|
|
||
|
|
|
|
active participation in |
|
|
|
|
|
|
||||||
|
Relapse, |
|
recovery goals or |
|
|
|
|
consequences. Client |
|
dangerous consequences to |
|
dangerous consequences to self or |
|
|
||
|
|
|
|
Outpatient, OR high |
|
|
|
|
|
|
||||||
|
Continued Use or |
|
achieve awareness |
|
|
|
|
needs |
|
self or others. |
|
others. |
|
|
||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
likelihood of relapse |
|
|
|
|
|
|
||||||
|
Continued |
|
of a substance use |
|
|
|
|
structure and support |
|
Does not recognize triggers, |
|
Does not recognize triggers, unable |
|
|
||
|
|
|
|
without close |
|
|
|
|
|
|
||||||
|
Problem Potential |
|
problem with minimal |
|
|
|
|
OR needs this support |
|
unable to control use, in |
|
to control use, in danger of relapse |
|
|
||
|
|
|
|
monitoring and |
|
|
|
|
|
|
||||||
|
|
|
|
support |
|
|
|
|
to transition into |
|
danger of relapse without |
|
without close |
|
|
|
|
|
|
|
|
|
support |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
community. |
|
close |
|
and structure. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
and structure. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Has a using, |
|
|
|
|
|
|
|
|
|
|
Supportive recovery |
|
|
Lacks social contacts |
|
|
unsupportive, |
|
Homelessness or lack of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
environment OR |
|
|
or social contacts |
|
|
dangerous, or |
|
|
Environment is dangerous or |
|
|
|
|
Dimension 6: |
|
|
|
|
|
|
|
safe, supportive recovery |
|
|
|
||||
|
|
|
willingness to obtain |
|
|
aren’t conducive to |
|
|
victimizing social |
|
|
unsupportive of recovery and client |
|
|
||
|
Recovery |
|
|
|
|
|
|
|
environment and client |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
such OR supports |
|
|
recovery, but with |
|
|
network, or lacks a |
|
|
lacks skills to cope outside of highly |
|
|
||
|
Environment |
|
|
|
|
|
|
|
needs |
|
|
|
||||
|
|
|
need professional |
|
|
structure or support, |
|
|
social network, |
|
|
structured |
|
|
||
|
|
|
|
|
|
|
|
|
learn to cope. |
|
|
|
||||
|
|
|
|
interventions. |
|
|
the patient can cope |
|
|
requiring this level of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Medication Assisted Treatments (MAT) can occur at any level of care and includes methadone, buprenorphine, and medications to control cravings and withdrawal when other criteria are met for level of care. Methadone and Suboxone clinics are generally outpatient, but clients on MAT may sometimes need a higher level of care.
**DDC: Dual Diagnosis Capable Program - has a primary target population of individuals with substance related disorders but also has an expectation and willingness to treat individuals with
referral to concurrent mental health services.
***DDE: Dual Diagnosis Enhanced Program – the program has the combined capacity to treat both mental health and substance related disorders equally.
Rater’s Signature: ____________________________________________________________
Last revision:
Form Characteristics
| Fact | Description |
|---|---|
| Form Title | The form is called the "Patient Placement Criteria Checklist - Kentucky Edition 2012," based on the ASAM Adult Patient Placement Criteria - Second Edition Revised. |
| Purpose | The main purpose of the form is to assess a client's needs across six different dimensions to determine the appropriate level of care for substance use treatment. |
| Levels of Care | It outlines six levels of care, ranging from outpatient services (Level I) to intensive inpatient treatment (Level IV), catering to varying degrees of severity in patient needs. |
| Governing Law | This form complies with Kentucky state regulations regarding the provision of substance use treatment services. |
| Admission Criteria | The form specifies criteria for admission at each level of care, ensuring that patients meet certain requirements before receiving treatment. |
Guidelines on Utilizing Asam Level Of Care Cheat Sheet
Completing the ASAM Level of Care Cheat Sheet involves assessing the patient across several dimensions and determining the appropriate level of care based on their needs and circumstances. Careful consideration of each dimension is crucial for accurate placement.
- Begin by entering the Client Name in the designated space.
- Fill in the Date of completion next to the Client Name.
- Add the Case Number in the indicated area.
- Review each of the six Dimensions, which include withdrawal potential, biomedical conditions, emotional and behavioral issues, readiness to change, relapse potential, and recovery environment.
- For each Dimension, rate the client’s status using the provided options, marking a check where appropriate.
- Analyze the ratings to determine the appropriate Level of Care—refer to the ratings guidelines to identify the minimum level required for effective treatment.
- Confirm the findings by signing and dating the Rater’s Signature section at the bottom of the form.
What You Should Know About This Form
What is the purpose of the ASAM Level of Care Cheat Sheet?
The ASAM Level of Care Cheat Sheet serves as a comprehensive tool to assist healthcare providers in determining the most appropriate level of care for individuals battling substance use disorders. It outlines key criteria across six dimensions to evaluate a client’s needs. By analyzing these dimensions, professionals can identify the least intensive level of care that ensures safety and helps clients progress toward their recovery goals. This method ensures that the placement aligns with the client's specific situations and challenges.
How should I use the dimensions when assessing a patient?
To assess a patient effectively, begin by rating each of the six dimensions on the checklist. Each dimension covers essential aspects of the client’s health and stability, including withdrawal symptoms, biomedical conditions, emotional and behavioral health, and social environment. Carefully consider the client’s situation in each dimension. After evaluating, analyze the ratings to identify the suitable level of care. Remember, prioritize emergency needs first, and then locate the least intensive yet safe option for treatment.
What do the different levels of care signify?
The different levels of care range from outpatient therapy to inpatient hospital treatment. Level I indicates outpatient services where clients receive fewer than six hours of therapy weekly. Levels II and III suggest higher intensity care, including intensive outpatient programs, residential treatment, and transitional care options. Level IV represents the highest level, commonly requiring hospitalized treatment for severe cases. Each level corresponds to a specific service type and sets unique admission criteria, ensuring that individuals receive care appropriate to their needs.
Can patients transition between different levels of care?
Yes, patients can transition between different levels of care as their treatment needs change. It’s crucial for providers to monitor clients continuously and reassess their condition regularly. If a client's progress is substantial, they may step down to a less intensive level of care. Conversely, if circumstances worsen, a client may require a higher level of care. Transitioning should always aim to match the client’s needs with the right services to optimize their recovery journey.
Common mistakes
Filling out the ASAM Level Of Care Cheat Sheet form can be a complex task. However, even small errors can lead to significant consequences for patient placement. Recognizing common mistakes can help ensure accurate evaluations. One of the most frequent errors is not thoroughly understanding the dimensions before rating the client. Each dimension has a specific set of criteria, and misinterpreting them can lead to inappropriate level-of-care recommendations.
Another mistake occurs when clients do not provide complete or accurate information. Omitting critical data, such as medical history or substance use details, impacts the assessment's reliability. This information is essential for determining the appropriate level of care. A third mistake is failing to prioritize emergency needs. It's crucial to address immediate risks before considering less intensive treatment options, so clinicians should keep this in mind during the evaluation process.
Some individuals may also overlook the significance of conducting a comprehensive analysis of all dimensions. It’s important to assess each dimension in relation to the others. Failing to do so can result in an imbalanced perspective on the client's needs. Lastly, rushing through the completion of the form can lead to careless errors. Taking your time ensures that each section receives adequate attention, ultimately benefiting client outcomes.
Documents used along the form
The ASAM Level Of Care Cheat Sheet is integral to determining appropriate care for individuals struggling with substance use disorders. However, several other forms and documents often accompany this cheat sheet, aiding in the overall treatment and placement process. The following is a list of such documents, along with descriptions of their purpose and function.
- Client Assessment Form: This document collects comprehensive information about the client's substance usage history, mental health status, and social circumstances. It serves as an initial evaluation tool to understand the client's needs and readiness for treatment.
- Treatment Plan Template: This structured outline specifies the therapeutic goals, interventions, and expected outcomes for a client. It is a roadmap guiding treatment and adjustments as necessary throughout the rehabilitation process.
- Progress Notes: These are regular updates documented by healthcare professionals detailing the client's ongoing progress, challenges faced, and any changes made to the treatment plan. They ensure continuity of care and help track the client's journey.
- Intake Form: Completed upon a client's entry into treatment, the intake form gathers essential information such as personal details, medical history, and consent for services. It sets the foundation for the client’s treatment experience.
- Discharge Summary: This document outlines a client's accomplishments during treatment, recommendations for continued support, and any follow-up appointments. It provides a comprehensive overview essential for the client’s ongoing recovery efforts.
- Referral Form: When a client requires additional services, such as mental health care or housing assistance, the referral form facilitates communication between providers. It enables seamless access to necessary support systems.
- Release of Information (ROI) Form: This form grants permission to share a client's personal health information with specified individuals or entities. It ensures confidentiality while promoting coordinated care across various service providers.
- Coordination of Care Plan: This document details the collaboration among various treatment providers involved in a client's care. It helps streamline communication, ensuring that everyone involved is on the same page regarding the client's needs and treatment strategies.
Utilizing these forms alongside the ASAM Level Of Care Cheat Sheet fosters a structured and holistic approach to treatment, facilitating effective care and support for clients on their journey to recovery.
Similar forms
-
Patient Placement Criteria Checklist: Like the ASAM Level Of Care Cheat Sheet, this document assesses patient needs across various dimensions to determine the appropriate level of care. It also prioritizes emergency needs and the least intensive level of care that can effectively help the client.
-
ASAM Criteria: This document outlines the criteria for patient placement across different levels of care. Its focus on the same six dimensions ensures consistency in evaluating patient needs, allowing for appropriate treatment planning based on severity and risk factors.
-
Clinical Assessment Tools: These tools serve a similar purpose by identifying the primary challenges faced by patients. They help professionals gauge readiness for treatment and necessary support levels, aligning with the ASAM's focus on personal needs and circumstances.
-
Treatment Planning Worksheets: Much like the ASAM Level Of Care Cheat Sheet, these worksheets guide practitioners in developing individualized treatment plans. They incorporate the classification of care levels and specific client needs, promoting tailored approaches to recovery.
Dos and Don'ts
When filling out the ASAM Level of Care Cheat Sheet form, it is important to follow established guidelines to ensure accuracy and effectiveness. Here is a list of actions you should consider:
- Do: Clearly write the client's name, date, and case number at the top of the form to avoid confusion.
- Do: Carefully assess each dimension of the patient’s condition before selecting a level of care.
- Do: Use objective observations and clinical data when rating the severity of each dimension.
- Do: Check all boxes that apply in each dimension to provide a comprehensive overview of the client's needs.
- Do: Ensure that the selected level of care aligns with the patient's current state and treatment goals.
In addition to these recommendations, some actions should be avoided:
- Don’t: Rush through the assessment; thoroughness is key for accurate placement.
- Don’t: Skip any dimensions; each plays a vital role in determining the appropriate level of care.
- Don’t: Provide subjective opinions instead of factual information; focus on the patient's clinical needs.
- Don’t: Leave any fields blank; incomplete forms can lead to incorrect assessments and treatment delays.
Misconceptions
Understanding the ASAM Level of Care Cheat Sheet is essential for effective patient placement in treatment settings. However, several misconceptions can cloud its use. Here are four common misunderstandings and clarifications about this tool:
- Misconception 1: The form is only for individuals with severe addiction issues.
- Misconception 2: The levels of care are rigid and do not allow for flexibility.
- Misconception 3: The cheat sheet guarantees a specific level of care for every client.
- Misconception 4: Using the cheat sheet is only relevant during initial assessments.
This is not entirely true. While the ASAM Level of Care Cheat Sheet is beneficial for those with significant substance use disorders, it can also be used for individuals at various stages of addiction, including those seeking early intervention or outpatient support. It evaluates needs across different dimensions, making it applicable to a wider range of patients.
Many people believe that the levels of care are fixed categories. In reality, the ASAM framework is designed to be flexible. Treatment providers can adapt their recommendations based on individual patient needs, and clients may move between levels as their circumstances change.
Some assume that completing the cheat sheet will automatically secure a particular level of care for the client. However, while it is a helpful guideline, the final determination for placement also depends on other factors, including available services and the clinical judgment of the treatment team.
It is a common belief that the ASAM Level of Care Cheat Sheet has limited application and is only necessary during the initial evaluation. On the contrary, it can be used throughout the treatment process to reassess patient needs and adjust levels of care as necessary for ongoing effectiveness and support.
Key takeaways
When using the ASAM Level Of Care Cheat Sheet, keep these key points in mind:
- Start by assessing the patient based on the six dimensions outlined in the form.
- Emergency needs should be addressed first, followed by identifying the least intensive level of care that is safe and can effectively support the patient's goals.
- Each level of care corresponds to specific service requirements, including the number of clinical staff hours and types of settings.
- Dimension scores will help to determine the appropriate level of care needed along with any necessary interventions.
- Medication Assisted Treatments (MAT) can occur at any level of care and may require additional support depending on the patient’s needs.
- Consider the patient’s readiness to change, as this will affect their engagement and cooperation in treatment.
- Be aware that different levels may require various types of programs, such as Dual Diagnosis Capable or Dual Diagnosis Enhanced programs.
- Document the patient's name, case number, and date accurately for proper tracking and follow-up.
Browse Other Templates
Smw Nys Go Ke Course Selection Pdf - Upon completion, recruits may engage in voluntary service projects or enroll in technical vocational education training.
Real Estate Client Information Sheet - It emphasizes the importance of communication between agents and buyers.
Motion to Modify Parenting Time Illinois - This form should be filed along with a Notice of Motion to initiate the court process for modifying visitation.