Fill Out Your Ash Mnr Form
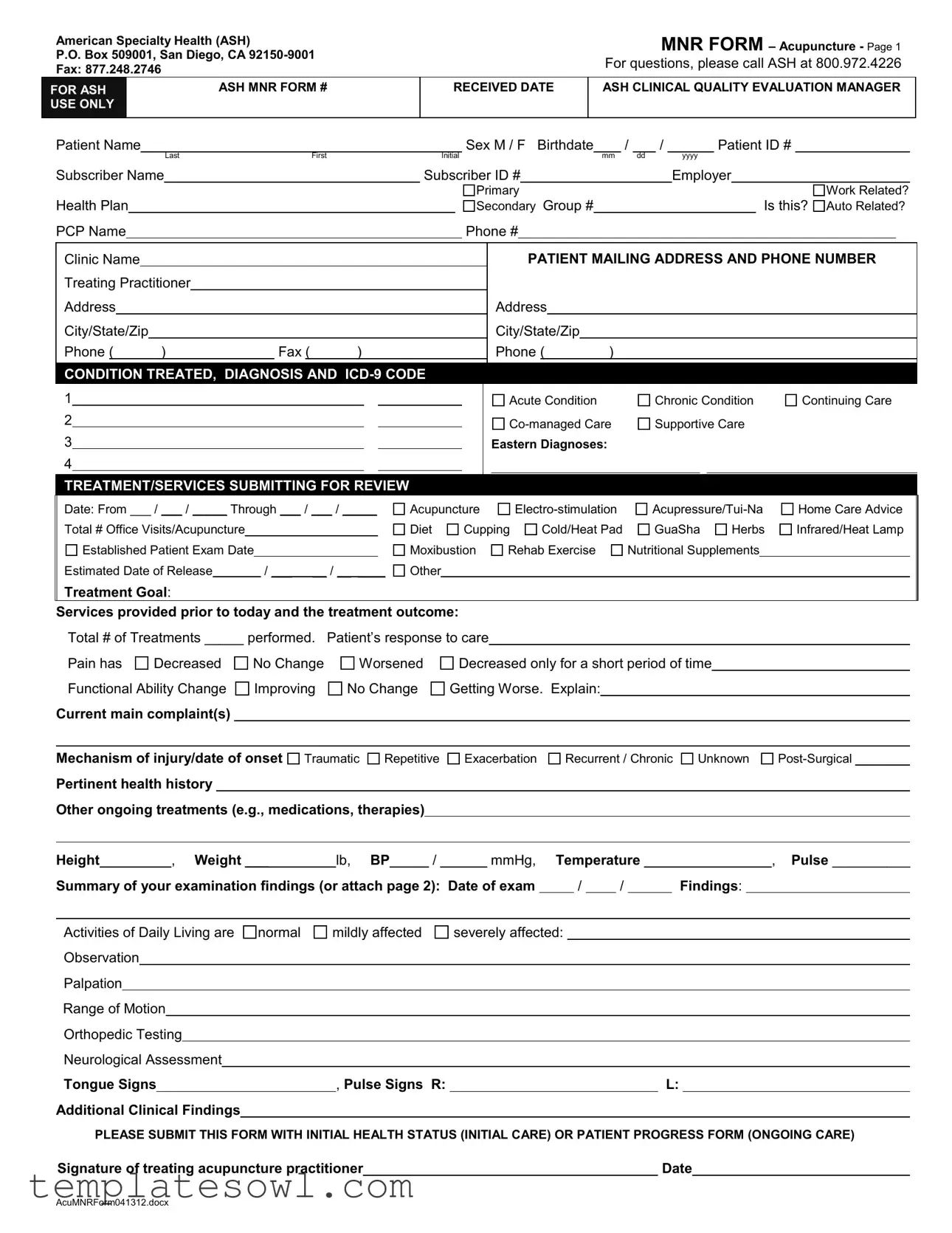
When managing a patient's acupuncture treatment, the Ash Mnr form plays an essential role, serving as a comprehensive tool for documenting relevant clinical information. This form collects a variety of patient details, including personal identification, medical history, and specifics about the treatment provided. Practitioners are required to note the diagnosis, treatment dates, and various modalities used, such as electro-stimulation, cupping, and nutritional supplements. To ensure an accurate representation of progress, the form also includes sections for detailing changes in the patient's condition and overall response to care. Furthermore, practitioners are prompted to describe the patient's ongoing health issues, explain their examination findings, and indicate any pertinent clinical observations. The Ash Mnr form not only facilitates communication between healthcare providers and insurance companies but also promotes continuity of care, ensuring that every patient's unique journey is meticulously documented. By emphasizing the patient’s perspective through comprehensive pain descriptions and treatment outcomes, this form underscores the collaborative nature of healthcare.
Ash Mnr Example
American Specialty Health (ASH)
P.O. Box 509001, San Diego, CA
Fax: 877.248.2746
FOR ASH |
ASH MNR FORM # |
USE ONLY |
|
MNR FORM – Acupuncture - Page 1
For questions, please call ASH at 800.972.4226
|
RECEIVED DATE |
ASH CLINICAL QUALITY EVALUATION MANAGER |
|
|
|
Patient Name |
|
|
Sex M / F Birthdate |
/ |
/ |
|
Patient ID # |
|||||||
|
|
Last |
First |
Initial |
|
mm |
|
dd |
|
yyyy |
|
|
||
Subscriber Name |
|
|
Subscriber ID # |
|
|
|
|
Employer |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Primary |
|
|
Health Plan |
|
Secondary Group # |
Is this? |
|||
PCP Name |
|
|
|
Phone # |
|
|
Work Related? Auto Related?
|
Clinic Name |
|
|
|
|
|
|
|
|
|
|
|
PATIENT MAILING ADDRESS AND PHONE NUMBER |
||||||||||||
|
Treating Practitioner |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Address |
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City/State/Zip |
|
|
|
|
|
|
|
|
|
|
City/State/Zip |
|
|
|
|
|
||||||||
|
Phone ( |
|
) |
|
Fax ( |
) |
|
|
|
|
|
Phone ( |
|
) |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
CONDITION TREATED, DIAGNOSIS AND |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Acute Condition |
|
Chronic Condition |
Continuing Care |
||||||
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Supportive Care |
|
||||||||
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Eastern Diagnoses: |
|
|
|
|
|
|||||
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
 TREATMENT/SERVICES SUBMITTING FOR REVIEW
TREATMENT/SERVICES SUBMITTING FOR REVIEW
Date: From ___ / ___ / _____ Through ___ / ___ / _____ |
Acupuncture |
|
Home Care Advice |
||||||||||||
Total # Office Visits/Acupuncture |
|
|
|
|
Diet |
Cupping |
Cold/Heat Pad |
GuaSha |
Herbs |
Infrared/Heat Lamp |
|||||
Established Patient Exam Date |
|
|
|
Moxibustion |
Rehab Exercise |
Nutritional Supplements |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Estimated Date of Release |
|
/ ___ __ / __ ____ |
Other |
|
|
|
|
|
|
|
|||||
Treatment Goal: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Services provided prior to today and the treatment outcome:
Total # of Treatments _____ performed. |
Patient’s response to care |
|
||||||
Pain has |
Decreased |
No Change |
Worsened |
Decreased only for a short period of time |
||||
Functional Ability Change |
Improving |
|
No Change |
Getting Worse. Explain: |
|
|
||
Current main complaint(s)
Mechanism of injury/date of onset  Traumatic
Traumatic  Repetitive
Repetitive 
 Exacerbation
Exacerbation 
 Recurrent / Chronic
Recurrent / Chronic 
 Unknown
Unknown 

Pertinent health history
Other ongoing treatments (e.g., medications, therapies)
Height |
|
____, Weight ___ |
|
lb, BP_____ / ______ mmHg, |
Temperature |
|
|
|
|
__, Pulse __________ |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Summary of your examination findings (or attach page 2): Date of exam |
|
/ |
|
/ |
|
|
|
Findings: |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Activities of Daily Living are normal |
mildly affected |
severely affected: |
|
|
|
|
|
|
|
|
|
||||||||||||||
Observation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Palpation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Range of Motion |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Orthopedic Testing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Neurological Assessment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Tongue Signs |
|
|
|
, Pulse Signs R: |
|
|
|
|
|
|
|
|
L: |
|
|||||||||||
Additional Clinical Findings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
PLEASE SUBMIT THIS FORM WITH INITIAL HEALTH STATUS (INITIAL CARE) OR PATIENT PROGRESS FORM (ONGOING CARE)
Signature of treating acupuncture practitioner |
|
Date |
|
|
|
|
|
AcuMNRForm041312.docx
American Specialty Health (ASH) |
|
|
MNR FORM |
||
|
|
|
|
Acupuncture Clinical Findings |
|
Patient Name |
|
Occupation |
Practitioner Name |
||
|
|
|
|
|
|
Pain Descriptions:
Pain Condition #1: Location ________________ Intensity
Pain is |
Sharp |
Dull |
Stabbing |
Burning |
Spasmodic |
|
Tingling |
Throbbing |
Stiffness |
Distension or |
|
|
|||||||||
Aggravating factors: |
|
|
|
|
|
|
|
|
Alleviating factors: |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Pain Condition #2: Location |
|
|
Intensity |
|
|
Frequency |
|
|
Duration |
|
hours/days |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Pain is |
Sharp |
Dull |
Stabbing |
Burning |
Spasmodic |
|
Tingling |
Throbbing |
Stiffness |
Distension or |
|
|
|||||||||
Aggravating Factors: |
|
|
|
|
|
|
|
|
Alleviating Factors: |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Other Pain Conditions: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Clinical Findings Related to Pain Location:
Head:
Pain with 
 Nausea/Vomiting
Nausea/Vomiting 
 Fever/Chills
Fever/Chills 
 Dizziness
Dizziness 
 Phono/Photophobia
Phono/Photophobia 
 Neck Rigidity
Neck Rigidity
Neurologic Deficit 
 Sensation
Sensation 
 Strength
Strength 
 Speech
Speech 
 Vision
Vision 
 Hearing
Hearing 
 Cognition
Cognition 
 Memory
Memory 
 Eye Motion/Pupils React
Eye Motion/Pupils React
Neck:
Tenderness at
Postural Abnormalities
Functional Limits
Back:
Mild |
Moderate |
Severe |
Worsened. |
Muscle Spasm |
Mild |
Moderate |
Severe |
|
|
Radiating Pain To |
|
|
|
|
|
Tenderness at ________________ |
Mild |
Moderate |
Severe |
Worsened. |
|
Muscle Spasm |
Mild |
Moderate |
Severe |
||||||
Postural Abnormalities ________________ |
Scoliosis _____________________ |
Radiating Pain To |
|
|
|
|
|||||||||
Functional Limits |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Extremities, Hip(s) and Shoulder(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Tenderness at _______________ |
Mild |
Moderate |
Severe |
Worsened. |
Muscle Spasm |
Mild |
Moderate |
Severe |
|||||||
Swelling _______________ Color change __________ |
Deformity |
|
|
|
Radiating pain to |
|
|
|
|
||||||
Functional Limits |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||||||
Neurologic Deficit Location |
|
|
|
|
Weakness |
Abnormal Sensation |
Reflexes (Increased/Decreased) |
||||||||
ROM of Affected joint(s) Use measurement or indicate if ROM Within Normal Limits (WNL), mildly, moderately or severely limited:
Joints
Flexion / Extension
Lateral Flexion R / L
Rotation R / L
Rotation Int./Ext.
Abduction / Adduction
Other:
Orthopedic/Neurological Test Findings: E.g., Axial Compression ______ ; Patrick’s (Fabere) _______ ; Straight Leg Raising
Abdominal Pain: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Associate Symptoms: Fever |
|
Nausea/Vomit |
Gas/Distension |
|
|
Heartburn/Reflux |
Constipation |
Diarrhea |
or |
|
|
|
|
|||||||||||||||||||||||||||||||
Palpable Mass at |
|
|
|
|
|
Tenderness at |
|
|
|
Rebound Tenderness |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bowel Movement Sounds (Increase/Decrease) |
|
|
|
|
|
|
|
|
Other Findings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Menstrual Pain: Menstrual Cycle |
|
|
|
|
days. Other Symptoms |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Additional Clinical Findings (including Lab / Radiographic Exams) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Outcome Assessments (List both Initial and Current date(s) with score(s) for applicable tests) |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
Initial |
|
|
|
|
Current |
|
|
|
|
|
|
|
|
|
|
Initial |
|
Current |
|
||||||||||||||||||||
List Date Obtained |
|
/ |
|
/ |
|
|
|
|
/ |
|
/ |
|
|
|
List Date Obtained |
|
|
/ |
|
|
/ |
|
|
|
|
|
/ |
|
/ |
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Neck Disability Index score |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
Oswestry score |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LEFS (Lower Extrem.) score |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Pain scale |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DASH (Upper Extrem.) score |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
Signature of treating acupuncture practitioner |
|
|
|
|
|
|
|
|
|
|
|
Examination Date (required)______________ |
|
|||||||||||||||||||||||||||||||
AcuMNRForm041312.docx
Form Characteristics
| Fact Name | Description |
|---|---|
| Provider Information | The form is issued by American Specialty Health located in San Diego, California. It includes contact details for inquiries. |
| Patient Identification | Sections for patient identification include the patient's name, birthdate, and unique patient ID number. |
| Treatment Types | Allowed treatment types for submission include acupuncture, electro-stimulation, acupressure, and more. |
| Diagnosis Codes | ICD-9 codes must be provided to indicate the patient's diagnosis related to the treatment. |
| Health Status Submission | It is essential to submit the initial health status or the patient progress form along with this document. |
| Clinical Findings | Details on pain conditions must be documented, including location, intensity, and any aggravating or alleviating factors. |
| Date Requirements | The form requires specific dates for treatment, examination, and submission, ensuring proper tracking. |
| Signature Confirmation | A signature from the treating acupuncture practitioner is mandatory to validate the submitted information on the form. |
Guidelines on Utilizing Ash Mnr
Once you have the Ash Mnr form in hand, you can proceed to complete it by following a series of organized steps. Taking your time here will ensure that all necessary information is accurately filled out, which is important for a smooth processing of your submission.
- Start with the Patient Name. Fill in the last name, first name, and initial.
- Indicate the Sex by marking 'M' for male or 'F' for female.
- Add the Birthdate in the format mm/dd/yyyy.
- Enter the Patient ID # assigned to the patient.
- Next, provide the Subscriber Name and Subscriber ID # along with the Employer name and Primary Health Plan.
- If applicable, fill out the Secondary Group #.
- Specify if the claim is Work Related or Auto Related.
- Input the Clinic Name and the Patient Mailing Address, including street address, city, state, and zip code.
- Provide both the Phone and Fax numbers for the clinic and the practitioner treating the patient.
- State the Condition Treated and select the relevant options regarding treatment: Acute Condition, Chronic Condition, etc.
- Indicate the dates for the Treatment/Services being submitted for review.
- Check off the applicable treatment types, such as Acupuncture, Electro-stimulation, etc.
- Detail the Estimated Date of Release. Fill this date as mm/dd/yyyy.
- Describe the Services provided prior to today along with the treatment outcome.
- Document the Patient’s response to care, including any changes in pain and functional ability.
- Explain the Current main complaint(s), including the mechanism of injury or date of onset.
- Fill in the Pertinent health history and any ongoing treatments the patient may be undergoing.
- Complete the clinical assessment by recording Height, Weight, Blood Pressure, Temperature, and Pulse.
- Summarize your examination findings or attach additional pages if necessary.
- Conclude with the Signature of treating acupuncture practitioner and the Date of signing.
After completely filling out the form, make sure to submit it along with any required documentation, such as the Initial Health Status or Patient Progress Form, to ensure a thorough review of the patient’s condition and treatment plan.
What You Should Know About This Form
What is the purpose of the Ash Mnr form?
The Ash Mnr form, utilized primarily by American Specialty Health (ASH), serves as a detailed tool for healthcare practitioners to report and review acupuncture treatments. The goal of the form is to gather comprehensive information about a patient's diagnosis, treatment plan, and progress. This allows ASH to evaluate the necessity and effectiveness of the proposed or ongoing acupuncture care, ensuring that patients receive appropriate support based on their specific health needs.
Who needs to complete the Ash Mnr form?
This form is intended to be completed by licensed acupuncture practitioners who provide treatment to patients covered under an ASH health plan. Practitioners use this form to document patient information, treatment modalities, and responses to care. It is essential for ensuring that all necessary details are submitted for ASH's review process, which assesses the appropriateness of the services provided.
What types of information must be included?
The Ash Mnr form requires various details, including patient demographics (name, date of birth, and contact information), treatment specifics (diagnosis, ICD-9 code), and clinical findings. Practitioners must also describe the nature of the patient’s condition, treatment goals, and the response to care, including any changes in pain levels or functional abilities. This comprehensive approach helps ASH make informed decisions about care continuation and coverage.
How can practitioners submit the Ash Mnr form?
Practitioners can submit the Ash Mnr form via mail or fax. The mailing address for submission is American Specialty Health, P.O. Box 509001, San Diego, CA 92150-9001. For those choosing to fax the completed form, the number is 877.248.2746. It is vital to ensure that the form is filled out completely and accurately to prevent delays in the review process.
What happens after the Ash Mnr form is submitted?
Once the form is submitted, ASH engages in a clinical quality evaluation. They review the information provided to determine if the care is necessary and aligns with established guidelines. Practitioners will receive feedback or requests for additional information if needed. This review process can be essential for approvals related to insurance coverage and authorization for ongoing treatments.
Can patients check the status of their Ash Mnr submission?
Yes, patients can inquire about the status of their Ash Mnr submission through their healthcare providers. Practitioners should be able to communicate updates or information received from ASH regarding the form review and any decisions made about the patient's treatment plan. Effective communication between patients and practitioners ensures everyone remains informed throughout the process.
Is there a deadline for submitting the Ash Mnr form?
While specific deadlines can vary depending on individual health plans and the nature of the treatment, it is crucial to submit the Ash Mnr form as promptly as possible. Timeliness ensures that the review process can commence without unnecessary delays, which ultimately helps facilitate ongoing patient care and support. Practitioners should refer to the guidelines provided by ASH or the patient’s health plan for any specific timelines.
Where can practitioners find resources for completing the Ash Mnr form?
Resources and guidance for completing the Ash Mnr form can typically be found on the American Specialty Health website or by contacting their support line at 800.972.4226. Practitioners may also receive training or educational materials directly from ASH that outlines the form's requirements and best practices for completion. Utilizing these resources can enhance the accuracy of submissions and support effective patient care.
Common mistakes
Filling out the ASH MNR form can be daunting. Many individuals make common mistakes that could delay processing. One frequent error is forgetting to include the patient’s ID number. This crucial identifier helps streamline communication and ensures efficient processing of the claim.
Another mistake is leaving out the subscriber information. If the patient is not the subscriber, failing to provide details about the subscriber can lead to confusion and further requests for information. It's essential to include the subscriber's name and ID number accurately.
Many people also overlook the mechanism of injury section. Clearly indicating whether the injury was traumatic, repetitive, or post-surgical helps practitioners understand the treatment context. Providing detailed descriptions enhances the clarity of the submission.
In the section detailing treatment rendered, the dates of service must be filled out correctly. Missing or incorrect dates can result in delays, as ASH needs to see a clear timeline of treatments provided. Additionally, the total number of treatments performed should match the submissions listed elsewhere in the form.
Another common oversight involves not providing sufficient detail about pain descriptions and accompanying symptoms. Vague terms like "pain" without elaboration make it difficult for the evaluators to understand the severity and implications, hindering the assessment process.
Many forms include an optional section for clinical findings. Failing to complete this could mean losing out on providing evidence that supports the treatment provided. Adding relevant clinical findings strengthens your case and demonstrates thoroughness.
The signature of the treating practitioner is a crucial sign-off, and some submitters forget this step altogether. An unsigned form is considered incomplete, leading to unnecessary delays in processing.
Poor organization of submissions is another issue. If supporting documents are not attached, or if they are misfiled, it complicates things for everyone involved. Always double-check to ensure all required information and documentation is included.
Additionally, not indicating whether the condition is work-related or auto-related can impact coverage. Clarifying the nature of the injury is necessary, especially when it pertains to insurance claims.
Lastly, many individuals fail to observe the submission method requirements. Whether sending by fax or mail, following the stated guidelines ensures that the form reaches ASH without issues. Always verify the address and ensure all communications are confirmed received.
Documents used along the form
When submitting an ASH MNR form, additional documents may be required to support your treatment requests. Here are six common forms that are often used alongside the ASH MNR form:
- Initial Health Status Form: This document outlines the patient's health condition at the beginning of treatment. It includes important information about medical history, current symptoms, and initial assessment findings.
- Patient Progress Form: This tracks the patient's progress throughout their treatment plan. It details improvements, setbacks, and changes in health status since the initial evaluation.
- Claim Form: This is used to submit a claim for reimbursement from the insurance provider. It includes information about the patient, services rendered, and costs associated with treatment.
- Referral Document: If outside referrals are involved, this form provides details on the referred practitioner and the reasons for the referral. It ensures continuity of care among different specialists.
- Treatment Plan Document: This outlines the proposed treatment strategy, including specific goals, frequency of visits, and types of therapies to be administered. It helps all parties understand the intended approach.
- Authorization for Release of Information: This document allows healthcare providers to share relevant patient information with other entities, such as insurance companies or specialists, facilitating better communication and care.
Submitting these documents along with the ASH MNR form helps ensure that the patient's case is thoroughly evaluated and processed efficiently. Always check with your clinic or practitioner for any specific requirements unique to your situation.
Similar forms
The Ash Mnr form shares similarities with several healthcare-related documents. Below is a list of ten such documents, outlining how they are comparable.
- Patient Intake Form: Like the Ash Mnr form, a patient intake form collects demographic information and medical history, establishing a baseline for treatment.
- Insurance Claim Form: The Ash Mnr form serves as a tool for providers to document services and submit to insurers, similar to how insurance claim forms function in requesting reimbursement.
- Progress Report: Both forms document the patient's treatment progress and outcomes over time, allowing for adjustments in care plans based on patient response.
- Referral Form: Similar to the Ash Mnr form, referral forms provide concise patient information to specialists for continuity of care, ensuring all relevant details are relayed.
- Medical History Questionnaire: The Ash Mnr form gathers pertinent medical history, much like a medical history questionnaire collects background information to inform treatment.
- Treatment Plan Document: Treatment plans outline specific care strategies, sharing a common purpose with the Ash Mnr form of guiding patient care based on outlined diagnoses and interventions.
- Consent Form: Just as consent forms ensure patients understand treatments they will receive, the Ash Mnr form verifies that practitioners document informed consent in the course of care.
- Outcome Measurement Tool: Both the Ash Mnr form and various outcome measurement tools assess the effectiveness of treatments, capturing patient responses and clinical findings.
- Diagnostic Request Form: The Ash Mnr form documents diagnoses and treatment goals, akin to how a diagnostic request form outlines information needed for testing and evaluation.
- Follow-Up Evaluation Form: Both forms aim to evaluate ongoing patient conditions and treatments, helping healthcare providers determine next steps based on the patient's current status.
Dos and Don'ts
When filling out the Ash Mnr form, there are important guidelines to follow. Adhering to these guidelines can help ensure that your submission is processed smoothly. Here are some essential dos and don'ts:
- Do provide accurate and complete patient information, including name, birthdate, and ID numbers.
- Do use clear and concise language when describing the condition treated and treatment outcomes.
- Do include the exact dates of treatment in the specified format to avoid confusion.
- Do ensure all signatures are present, especially from the treating acupuncture practitioner.
- Do double-check all diagnoses and ICD-9 codes for accuracy.
- Don't leave any fields blank; incomplete forms may be returned or delayed.
- Don't use unclear language or abbreviations that could lead to misunderstandings.
- Don't provide information that is not requested on the form, as it can create confusion.
- Don't forget to submit all required supporting documents alongside the MNR form.
- Don't rush through the form; take your time to ensure all information is accurate and thorough.
Misconceptions
- Misconception 1: The Ash Mnr form is only needed for acupuncture treatments.
- Misconception 2: I can submit the Ash Mnr form any time after the treatment.
- Misconception 3: I need to provide a detailed medical history every time I fill out the Ash Mnr form.
- Misconception 4: The provider does not need to sign the Ash Mnr form.
- Misconception 5: The form is only for new patients.
- Misconception 6: The ICD-9 code is optional on the Ash Mnr form.
- Misconception 7: I can send the Ash Mnr form via email.
- Misconception 8: Only certain conditions qualify for submitting the Ash Mnr form.
- Misconception 9: Providing patient's response to care is not important.
- Misconception 10: I can leave certain sections of the Ash Mnr form blank.
This form can actually be used for other modalities as well, including electro-stimulation and cupping.
The form must be submitted alongside the initial health status or patient progress forms. Timeliness is key for appropriate review.
You only need to provide the relevant information that pertains to the current condition being treated.
A signature from the treating acupuncture practitioner is essential; it validates the information provided.
Established patients also need to submit this form when seeking ongoing care or updates regarding their treatment plan.
The code is important; it identifies the diagnosis accurately and facilitates the review process.
This form needs to be faxed or mailed to ensure secure handling of patient information.
The form accommodates a variety of conditions, both acute and chronic. Always check with your provider for specifics.
This information is crucial as it helps assess the effectiveness of the treatment and guides future care.
Completing all relevant sections ensures comprehensive evaluations and prevents delays in processing.
Key takeaways
Here are some key takeaways for filling out and using the ASH MNR form:
- Patient Information: Clearly enter the patient's name, sex, birthdate, and ID number to avoid any identification errors.
- Subscriber Details: Include subscriber name and ID, as well as employer and health plan information, both primary and secondary.
- Condition and Diagnosis: Specify the condition being treated, including the diagnosis and correct ICD-9 code to ensure proper processing.
- Treatment Timeline: Clearly state the treatment dates. Specify the beginning and end dates for the services being reviewed.
- Detailed Treatment Description: List all treatments provided, including acupuncture, moxibustion, and any other relevant services.
- Patient Response: Document the patient’s response to treatment accurately. This includes any changes in pain level or functional ability.
- Important Measurements: Record the patient’s height, weight, blood pressure, temperature, and pulse for comprehensive assessment.
- Signature Requirement: Ensure the treating acupuncture practitioner signs the form and includes the date; without this, the submission may be rejected.
- Attach Relevant Documents: Include initial health status or patient progress forms as indicated. This can support the review process.
- Contact Information: Provide accurate clinic and practitioner contact details to facilitate follow-up or additional information requests.
Filling out the form correctly is crucial for effective communication with American Specialty Health. Attention to detail can significantly enhance the likelihood of approval for necessary services.
Browse Other Templates
Which of the Following Vessels Must Be Registered to Operate Legally on Mississippi Public Waters? - Be mindful of deadlines when applying to ensure timely registration.
California Corporation - Ensure accurate information is provided to avoid delays in processing.