Fill Out Your Authorized Representative Form
The Authorized Representative Form plays a crucial role in how individuals can delegate the authority to share their personal health information with someone they trust. For members of UnitedHealthcare, this form enables a designated person, known as the Authorized Representative, to interact with United HealthCare Services and access necessary health-related details. It's essential to note that this form does not grant the Authorized Representative the power to make treatment or care decisions on behalf of the member; additional legal documentation is required for those circumstances. The form includes sections to provide personal information about the enrollee, such as their name and contact details, and it also outlines the responsibilities accepted by the Authorized Representative. Importantly, there are provisions within the form that address the waiver of fees for representation, as well as stipulations concerning the authorization's expiration and the ability to revoke it at any time. Understanding this form and its implications is vital for both enrollees and their chosen representatives, ensuring that personal health information is handled securely and appropriately.
Authorized Representative Example
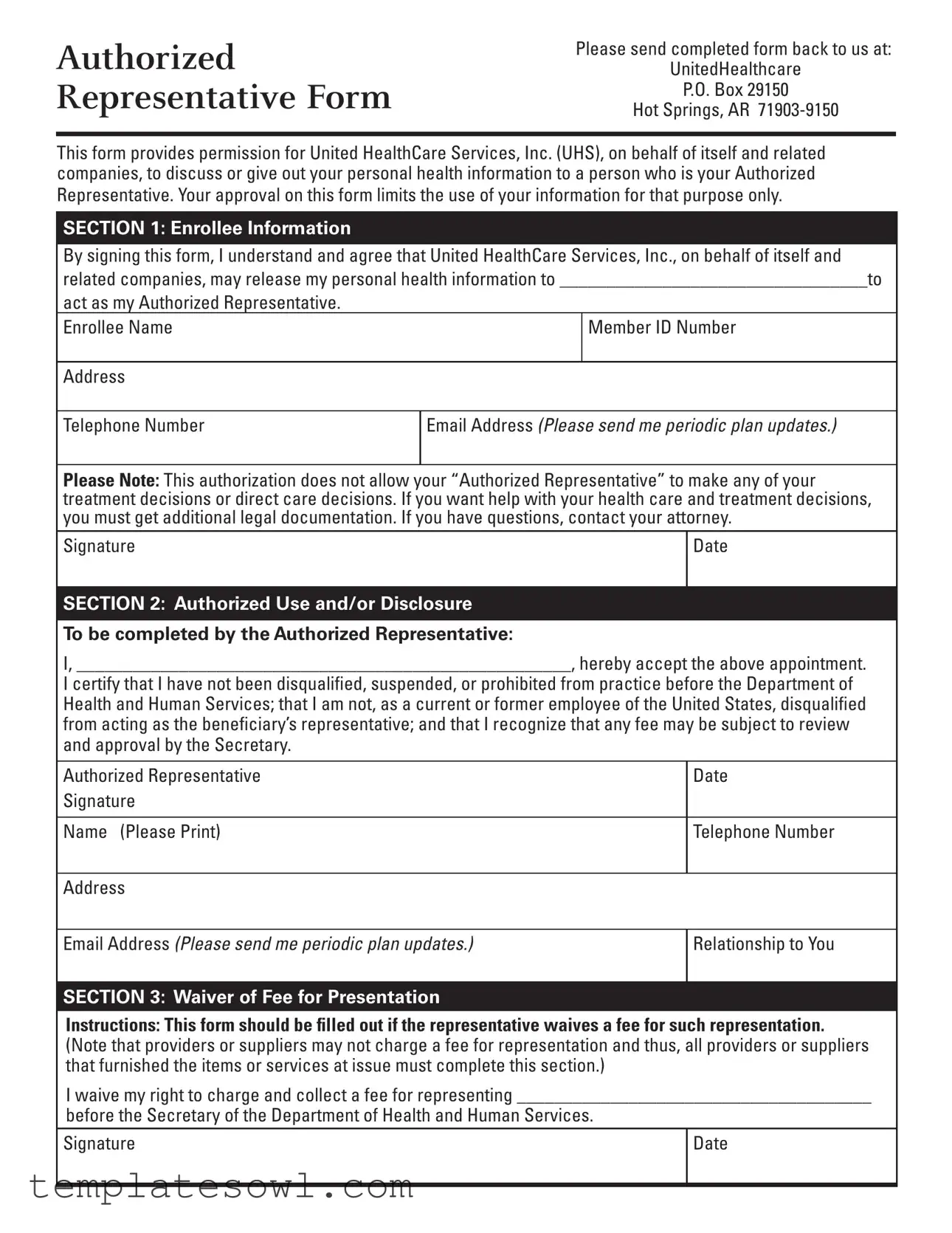
Authorized Representative Form
Please send completed form back to us at:
UnitedHealthcare
P.O. Box 29150
Hot Springs, AR
This form provides permission for United HealthCare Services, Inc. (UHS), on behalf of itself and related companies, to discuss or give out your personal health information to a person who is your Authorized Representative. Your approval on this form limits the use of your information for that purpose only.
SECTION 1: Enrollee Information
By signing this form, I understand and agree that United HealthCare Services, Inc., on behalf of itself and related companies, may release my personal health information to _________________________________to
act as my Authorized Representative.
Enrollee Name |
Member ID Number |
|
|
Address |
|
Telephone Number
Email Address (Please send me periodic plan updates.)
Please Note: This authorization does not allow your “Authorized Representative” to make any of your treatment decisions or direct care decisions. If you want help with your health care and treatment decisions, you must get additional legal documentation. If you have questions, contact your attorney.
Signature |
Date |
|
|
SECTION 2: Authorized Use and/or Disclosure
To be completed by the Authorized Representative:
I, _____________________________________________________, hereby accept the above appointment.
I certify that I have not been disqualified, suspended, or prohibited from practice before the Department of Health and Human Services; that I am not, as a current or former employee of the United States, disqualified from acting as the beneficiary’s representative; and that I recognize that any fee may be subject to review and approval by the Secretary.
Authorized Representative |
Date |
Signature |
|
|
|
Name (Please Print) |
Telephone Number |
|
|
Address |
|
Email Address (Please send me periodic plan updates.)
Relationship to You
SECTION 3: Waiver of Fee for Presentation
Instructions: This form should be filled out if the representative waives a fee for such representation. (Note that providers or suppliers may not charge a fee for representation and thus, all providers or suppliers that furnished the items or services at issue must complete this section.)
I waive my right to charge and collect a fee for representing ______________________________________
before the Secretary of the Department of Health and Human Services.
Signature
Date
SECTION 4: Waiver of Payment for Items or Services at Issue
Instructions: Providers or suppliers that furnished the items or services at issue must complete this section if the appeal involves a question of liability under section 1879(a)(2) of the Act. (Section 1879(a)(2) generally addresses whether a provider/supplier or beneficiary did not know, and could not reasonably be expected to know, that the items or services at issue would not be covered by Medicare.)
I waive my right to collect payment from the beneficiary for furnished items or services at issue involving Section 1879(a)(2) of the Act.
Signature
Date
SECTION 5: Expiration and Revocation
I understand that I have the right to end this authorization at any time. I understand that, if I do not wish the person(s) named in Section 2 to remain my Authorized Representative, I must cancel this authorization. I understand that I must put this in writing and send this written notice of my decision to the health plans.
I understand that if UHS has already released any of my personal health information before UHS receives my written request to end this authorization, my notice cannot cancel out any action UHS has already taken.
CHARGING OF FEES FOR REPRESENTING BENEFICIARIES BEFORE THE
SECRETARY OF THE DEPARTMENT OF HEALTH AND HUMAN SERVICES
An attorney, or other representative for a beneficiary, who wishes to charge a fee for services rendered in connection with an appeal before the Department of Health and Human Services (DHHS) at the Administrative Law Judge (ALJ) or Medicare Appeals Council (MAC) level is required by law to obtain approval of the fee in accordance with 42 CFR §405.910(f). A claim that has been remanded by a court to the Secretary for further administrative proceedings is considered to be before the secretary after the remand by the court.
The form, “Petition to Obtain Representative Fee” elicits the information required for a fee petition. It should be completed by the representative and filed with DHHS. Where a representative has rendered services in a claim before DHHS, the regulations require that the amount of the fee to be charged, if any, for services performed before the Secretary of DHHS be specified. If any fee is to be charged for such services, a petition for approval of that amount must be submitted.
An approval of a fee is not required where the appellant is a provider or supplier or where the fee is for services
(1)rendered in an official capacity such as that of legal guardian, committee, or similar court appointed office and the court has approved the fee in question; (2) in representing the beneficiary before the federal district court of above, or (3) in representing the beneficiary in appeals below the ALJ level. If the representative wishes to waive a fee, he or she may do so. Section III on the front of this form can be used for that purpose. In some instances, as indicated on the form, the fee must be waived for representation.
AUTHORIZATION OF FEE
The requirement for the approval of fees ensures that representative will receive fair value for the services performed before DHHS on behalf of a claimant while at the same time giving a measure of security to the beneficiaries. In approving a requested fee, the ALJ or MAC considers the nature and type of services performed, the complexity of the case, the level of skill and competence required in rendition of the services, the amount of time spent on the case, the results achieved, the level of administrative review to which the representative carried the appeal and the amount of the fee requested by the representative.
CONFLICT OF INTEREST
Sections 203, 205 and 207 of Title XVIII of the United States Code make it a criminal offense for certain officers, employees and former officers and employees of the United States to render certain services in matters affecting the Government or to aid or assist in the prosecution of claims against the United States. Individuals with a conflict of interest are excluded from being representatives of beneficiaries before DHHS.
SAPDP3060880_XAUE000
S5820S5805S5921_PDP3060880_001 CMS 07/2008
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose of the Form | The Authorized Representative Form allows United Health Care Services, Inc. to share personal health information with a designated authorized representative. |
| Limit of Authorization | This form permits the release of personal health information solely for the specified purpose and does not allow the representative to make treatment decisions. |
| Authorization Revocation | Enrollees have the right to revoke the authorization at any time by providing written notice to the health plans. |
| Fee Waiver | The form includes sections for waiving fees for representation, with an explicit requirement that fees cannot be charged if certain conditions are met. |
| Cancellation Process | Cancellations of authorization must be submitted in writing and should be sent directly to United Health Care. |
| Governing Law | For Medicare appeals, the governing law includes provisions under Title XVIII of the United States Code and the relevant regulations found in 42 CFR §405.910(f). |
| Signature Requirement | Both the enrollee and the authorized representative must sign the form to validate the authorization. |
| Limitation on Representatives | Individuals with disqualifications, suspensions, or prohibitions from practice before the Department of Health and Human Services cannot act as authorized representatives. |
| Item Payment Waiver | Providers or suppliers must complete a section if they waive the right to collect payment for items or services in question under section 1879(a)(2) of the Act. |
| Periodic Updates | Enrollees can opt to receive periodic plan updates by providing their email address on the form, fostering better engagement. |
Guidelines on Utilizing Authorized Representative
Filling out the Authorized Representative form helps ensure that a person you trust can obtain your health information from UnitedHealthcare on your behalf. Completing this form accurately is important for granting permission while protecting your privacy. Follow these steps to fill it out correctly.
- Start with Section 1: Enrollee Information. Write your full name, Member ID Number, address, telephone number, and email address. If you want to receive updates, check the box next to the email section.
- Next, designate your Authorized Representative. In the space provided, fill in the name of the person you are authorizing to receive your health information. Make sure you trust this individual.
- Sign and date the form. This signature indicates your consent for UnitedHealthcare to share your information with the designated representative.
- Move to Section 2: Authorized Use and/or Disclosure. The Authorized Representative must fill out this section. They should write their name, date, and signature. They also need to provide their contact details and relationship to you.
- Section 3 is for Waiver of Fee for Presentation. If the representative is waiving the right to charge you a fee for this representation, they need to sign and date this section.
- Section 4 deals with Waiver of Payment for Items or Services at Issue. If applicable, the Authorized Representative will need to sign and date here too.
- Lastly, review Section 5: Expiration and Revocation. Familiarize yourself with the rights regarding revocation. If you want to cancel this authorization in the future, you will need to put it in writing and send it to the health plans.
After completing the form, make sure to send it to the correct address provided by UnitedHealthcare: P.O. Box 29150, Hot Springs, AR 71903-9150. Keeping a copy for your records is also a good idea, just in case you need to refer back to it later.
What You Should Know About This Form
What is the purpose of the Authorized Representative form?
This form allows you to designate someone to discuss or receive your personal health information from United HealthCare Services, Inc. (UHS). By completing this form, you provide clear permission for UHS to share that information only with the person you specify, ensuring your privacy is maintained for that specific purpose.
Who can I appoint as my Authorized Representative?
You can appoint a trusted individual, such as a family member, friend, or caregiver, to act on your behalf. It's important to choose someone reliable, as they will have access to your health information. However, keep in mind that this authorization does not allow them to make treatment decisions for you; separate legal documentation would be required for that.
Do I need to fill out any specific sections of the form?
Yes, you must complete Section 1 with your information, including your name and member ID number. In Section 2, your Authorized Representative will need to fill in their information and certify their acceptance of this role. Additionally, if your representative waives any fee for representing you, they can note that in Section 3.
How do I revoke or end this authorization?
If you decide that you no longer want someone to be your Authorized Representative, you have the right to cancel the authorization. This must be done in writing. When you send this written notice to UHS, make sure it's clear that you wish to revoke the authorization. Be aware that any information already released prior to your notice cannot be undone.
Will my Authorized Representative be able to charge me a fee for their help?
Typically, representatives like attorneys must obtain approval to charge fees for assisting with claims before the Department of Health and Human Services. However, your Authorized Representative may choose to waive any fee for their services, which they can indicate on the form. If they do not intend to charge, having this documented provides clarity moving forward.
Can my Authorized Representative help with treatment decisions using this form?
No, this form strictly limits the access to your personal information and does not grant your Authorized Representative the authority to make decisions about your healthcare. If you want someone to assist you in treatment decisions, you would need a different type of legal agreement.
What happens if UHS has already shared my information?
If UHS has shared your health information before they receive your written request to revoke the authorization, there is no way to reverse those actions. Your notice only instructs UHS regarding future disclosures, not prior ones.
Do I need to complete the entire form, or are there sections I can skip?
It is crucial to complete the sections that apply to you. All information on the form serves a purpose, whether it's outlining who your Authorized Representative is, confirming they are accepting the role, or noting any waivers of fees. Skipping sections may lead to confusion or delays in processing your authorization.
Where do I send the completed Authorized Representative form?
Send the completed form to UnitedHealthcare at the following address: UnitedHealthcare, P.O. Box 29150, Hot Springs, AR 71903-9150. It's always a good idea to keep a copy of the form for your records before sending it off.
Common mistakes
Completing the Authorized Representative form can be a straightforward process, but mistakes often occur that could delay or complicate approval. One common error is failing to provide complete information in the Enrollee Information section. Missing details like the Member ID Number or contact information can lead to unnecessary back-and-forth communication. Ensuring that each field is fully filled out helps facilitate the processing of the form and ensures that it reaches the correct team at UnitedHealthcare.
Another frequent mistake involves not signing the form. Though it might seem obvious, many individuals overlook the importance of including their signature and the date. This step is critical because without a signature, the authorization is considered invalid. Subsequently, the form cannot be processed, which can cause delays in obtaining assistance or necessary medical information.
In Section 2, many people forget to have their Authorized Representative sign and provide their information. It's essential that this individual acknowledges their role formally by signing and filling out their details correctly. The absence of their signature may lead to confusion regarding their authorization, undermining the purpose of the form and delaying important health-related discussions.
Lastly, people often misunderstand the scope of authorization outlined in the form. Many mistakenly believe that granting someone the title of Authorized Representative allows them to make health treatment decisions on behalf of the enrollee. However, the form explicitly states that this authorization does not grant any decision-making power regarding treatment. Understanding this limitation ensures that individuals do not overstep boundaries, which could lead to misunderstandings about care and representation.
Documents used along the form
The Authorized Representative form is often accompanied by various documents that facilitate the representation process. Below is a list of forms that are frequently used alongside the Authorized Representative form, each serving a distinctive purpose in health care and legal representation.
- Petition to Obtain Representative Fee - This document is submitted by representatives seeking approval for any fees charged for their services rendered in connection with an appeal before the Department of Health and Human Services.
- Waiver of Fee for Presentation - This form indicates that the Authorized Representative waives their right to charge a fee for representing an individual before the Secretary of the Department of Health and Human Services.
- Waiver of Payment for Items or Services - This section is completed by providers or suppliers to indicate they will not seek payment from the beneficiary for specific items or services at issue.
- Revocation of Authorization - A written document that an individual uses to cancel the authorization granted to their Authorized Representative, thereby ending their ability to access the beneficiary's personal health information.
- Medical Release Form - This form authorizes healthcare providers to disclose specific medical records or information to the Authorized Representative for the purpose of representation.
- HIPAA Authorization Form - It allows healthcare entities to share protected health information with third parties, ensuring compliance with the Health Insurance Portability and Accountability Act (HIPAA).
- Claim Form - A standard form used to request benefits or reimbursement for healthcare costs from an insurance provider or government agency.
- Appeal Form - This document is used when a beneficiary wishes to formally appeal a decision made by a healthcare service provider or insurer regarding the coverage of services or items.
- Statement of Disqualification - A declaration confirming that the Authorized Representative does not have any disqualifications that would prevent them from acting on behalf of the beneficiary.
These documents work together to ensure that individuals can effectively navigate the healthcare system while maintaining control over their personal health information. Understanding each of these forms can aid beneficiaries in making informed decisions about their representation and healthcare needs.
Similar forms
- Power of Attorney (POA): Like the Authorized Representative form, a Power of Attorney grants someone the authority to act on behalf of another person. However, POA can allow for broader decision-making powers, including financial and healthcare decisions.
- Health Care Proxy: This document specifically allows an individual to appoint someone to make healthcare decisions on their behalf if they become unable to do so. Unlike the Authorized Representative form, a Health Care Proxy can empower someone to make treatment decisions.
- Medical Release Form: Similar to the Authorized Representative form, this document permits healthcare providers to release an individual's medical information to a designated person. It serves the same purpose of managing personal health information but does not confer decision-making authority.
- HIPAA Authorization Form: This document is used to authorize the disclosure of health information in accordance with the Health Insurance Portability and Accountability Act (HIPAA). While it also protects personal health information, it is broader in scope compared to the Authorized Representative form.
- Living Will: A living will indicates an individual's wishes regarding medical treatment in case of terminal illness or incapacity. Unlike the Authorized Representative form, it directly lays out treatment preferences rather than assigning someone to speak on their behalf.
- Appointment of Representative (AOR) Form: This identical function empowers a person to assist with Social Security claims. Similar to the Authorized Representative form, it designates a representative but is specific to Social Security-related matters.
- Consent for Treatment Form: This form allows patients to give their consent for medical treatments or procedures. While the Authorized Representative form focuses on information sharing, consent forms are usually about agreeing to specific medical interventions.
Dos and Don'ts
When filling out the Authorized Representative form, there are important guidelines to follow. Here’s a list of things you should and shouldn't do:
- Do ensure all information is accurate and complete to avoid delays.
- Do sign and date the form where required, as this confirms your consent.
- Do provide contact information for yourself and your Authorized Representative.
- Do read through all sections thoroughly before submitting.
- Don't leave any required fields blank, as this may lead to rejection of the form.
- Don't forget to notify the health plan in writing if you decide to revoke the authorization.
- Don't assume your Authorized Representative can make treatment decisions; they only have access to information.
Misconceptions
Misconceptions about the Authorized Representative form can lead to confusion and mismanagement of health information. Here are six common misconceptions explained:
- Authorized Representatives can make treatment decisions: The form only allows a representative to access health information. They cannot make treatment or care decisions on behalf of the enrollee.
- All representatives must be attorneys: While many representatives may be attorneys, anyone can be appointed as a representative as long as they meet certain requirements outlined by UnitedHealthcare.
- The form automatically goes into effect until revoked: The authorization does not automatically remain in effect indefinitely. It can be revoked at any time by the enrollee, but written notice must be provided to the health plan.
- Representatives can charge any fee for their services: Not all representatives are allowed to charge fees, and if a fee is to be charged, it must follow specific approval procedures set by the Department of Health and Human Services.
- Once signed, the information is no longer protected: Signing the form does allow information sharing, but it does not eliminate protections under privacy regulations. The information shared is strictly limited to what the authorization specifies.
- The form can be completed verbally: The form requires a physical signature from both the enrollee and the authorized representative. Verbal agreements are not valid for this purpose.
Key takeaways
When filling out the Authorized Representative form, keep the following key takeaways in mind:
- This form grants United HealthCare Services, Inc. permission to share your personal health information with your chosen Authorized Representative.
- Signing the form does not give your Authorized Representative the ability to make treatment decisions on your behalf. Additional legal documentation is required for that level of authority.
- You have the right to revoke this authorization at any time by providing written notice to United HealthCare Services.
- If you select an Authorized Representative, ensure that they are qualified and have not been disqualified, suspended, or prohibited from practicing before the Department of Health and Human Services.
- Representatives can opt to waive their fees for assisting you. This should be indicated in Section 3 of the form if applicable.
- Be aware that upon completion and submission, your designation of an Authorized Representative is effective only until you revoke it in writing.
Browse Other Templates
Dcnr Login - The P A Forestry Application is required for work on or near trees under NYC Parks jurisdiction.
Ny State Sales Tax - Submitting the DTF-803 form does not guarantee exemption approval; it's subject to review.