Fill Out Your Bridges Access Application Form
The Bridges Access Application form is a crucial tool for individuals seeking assistance with GlaxoSmithKline medications through the Bridges to Access patient assistance program. This program aims to help those who find it challenging to afford necessary medications. Eligibility hinges on specific criteria, including household income and insurance status, making it essential for applicants to gather accurate information before applying. The form requires detailed applicant information, including demographics, income verification, and health conditions. It also asks questions related to existing prescription coverage, including any involvement in state or federal drug programs, which can influence the need for assistance. Once completed, the application must be accompanied by proof of income and prescription details and sent to the designated address. If approved, applicants can access medication for up to a year, initiating with a 90-day supply sent by mail. Reapplication is necessary annually to maintain continued access to support. For further guidance, applicants can visit the dedicated website or contact the program directly. Ensuring all necessary documents are included is vital for a smooth application process.
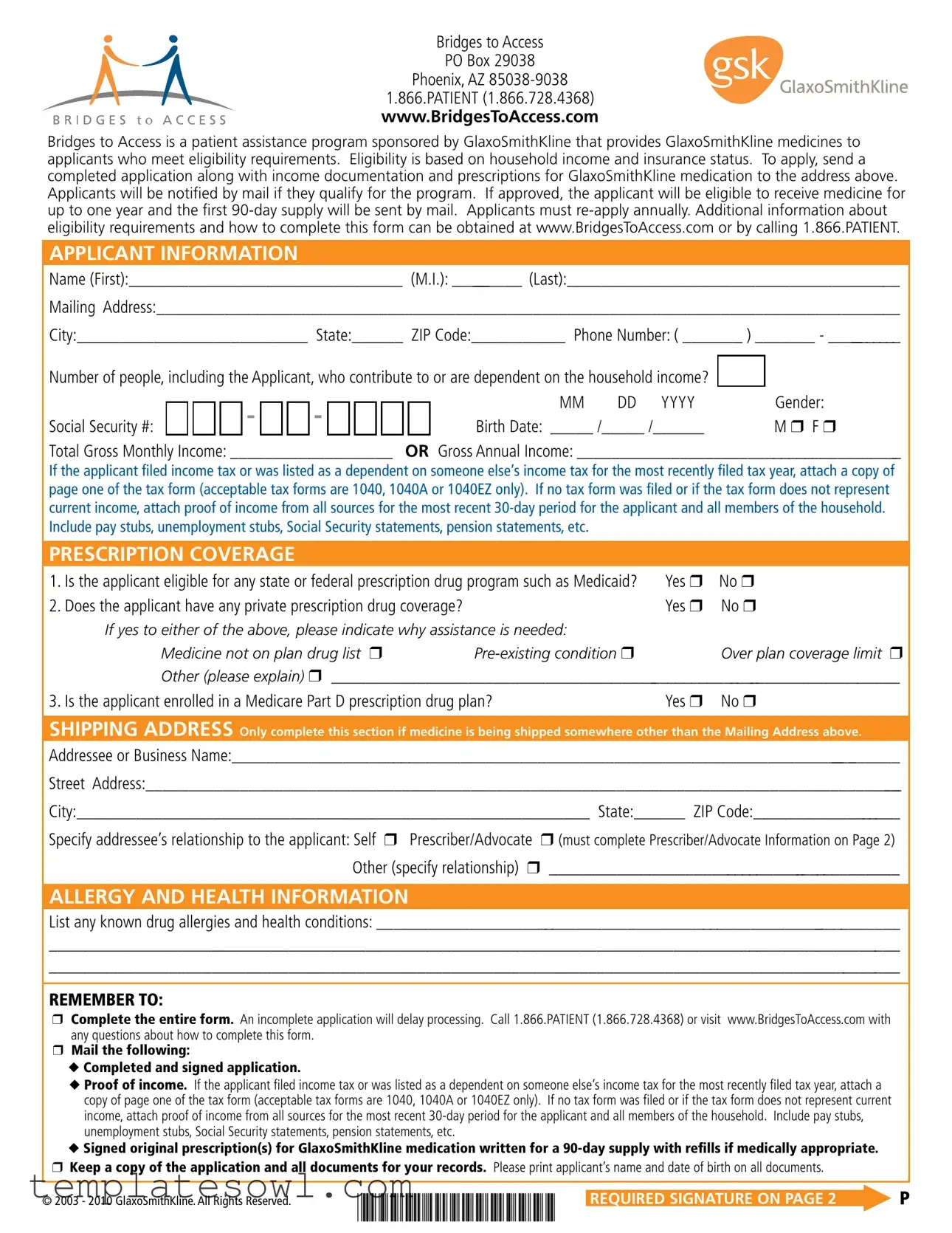
Bridges Access Application Example

Bridges to Access
PO Box 29038
Phoenix, AZ
1.866.PATIENT (1.866.728.4368) www.BridgesToAccess.com
Bridges to Access is a patient assistance program sponsored by GlaxoSmithKline that provides GlaxoSmithKline medicines to applicants who meet eligibility requirements. Eligibility is based on household income and insurance status. To apply, send a completed application along with income documentation and prescriptions for GlaxoSmithKline medication to the address above. Applicants will be notified by mail if they qualify for the program. If approved, the applicant will be eligible to receive medicine for up to one year and the first
APPLICANT INFORMATION
Name (First):________________________________ (M.I.): _________ (Last):_______________________________________
Mailing Address:_______________________________________________________________________________________
City:___________________________ State:______ ZIP Code:___________ Phone Number: ( _______ ) _______ - __________
Number of people, including the Applicant, who contribute to or are dependent on the household income? |
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MM |
DD YYYY |
|
Gender: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Social Security #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Birth Date: _____ /_____ /______ |
|
M r F r |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Total Gross Monthly Income: ___________________ |
OR Gross Annual Income: _______________________________________ |
||||||||||||||||||||||||
If the applicant filed income tax or was listed as a dependent on someone else’s income tax for the most recently filed tax year, attach a copy of page one of the tax form (acceptable tax forms are 1040, 1040A or 1040EZ only). If no tax form was filed or if the tax form does not represent current income, attach proof of income from all sources for the most recent
PRESCRIPTION COVERAGE
1. |
Is the applicant eligible for any state or federal prescription drug program such as Medicaid? |
Yes r |
No r |
2. |
Does the applicant have any private prescription drug coverage? |
Yes r |
No r |
If yes to either of the above, please indicate why assistance is needed:
Medicine not on plan drug list r |
Over plan coverage limit r |
|
Other (please explain) r _____________________________________________________________________ |
||
3. Is the applicant enrolled in a Medicare Part D prescription drug plan? |
Yes r No r |
|
SHIPPING ADDRESS Only complete this section if medicine is being shipped somewhere other than the Mailing Address above.
Addressee or Business Name:_________________________________________________________________________________
Street Address:_________________________________________________________________________________________
City:____________________________________________________________ State:______ ZIP Code:__________________
Specify addressee’s relationship to the applicant: Self r Prescriber/Advocate r (must complete Prescriber/Advocate Information on Page 2) Other (specify relationship) r ___________________________________________
ALLERGY AND HEALTH INFORMATION
List any known drug allergies and health conditions: ________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
REMEMBER TO:
rComplete the entire form. An incomplete application will delay processing. Call 1.866.PATIENT (1.866.728.4368) or visit www.BridgesToAccess.com with any questions about how to complete this form.
rMail the following:
u Completed and signed application.
u Proof of income. If the applicant filed income tax or was listed as a dependent on someone else’s income tax for the most recently filed tax year, attach a copy of page one of the tax form (acceptable tax forms are 1040, 1040A or 1040EZ only). If no tax form was filed or if the tax form does not represent current income, attach proof of income from all sources for the most recent
u Signed original prescription(s) for GlaxoSmithKline medication written for a
rKeep a copy of the application and all documents for your records. Please print applicant’s name and date of birth on all documents.
© 2003 - 2010 GlaxoSmithKline. All Rights Reserved. |
PAGE 1 |
REQUIRED SIGNATURE ON PAGE 2 |
P |
APPLICANT AUTHORIZATION TO RELEASE AND DISCLOSE MEDICAL INFORMATION
By my signature I authorize GlaxoSmithKline, as well as McKesson Specialty Arizona Inc. (MSAZ) and any other companies that GlaxoSmithKline uses to administer Bridges to Access (the “Program”), to do the following:
1)Use any information that I provide in my application for the Program for the purpose of helping me receive GlaxoSmithKline products under the Program or to administer the program;
2)Receive and keep records of all prescriptions for the medications I receive under the Program, which will be used to administer the program;
3)Contact my doctor, healthcare provider, or pharmacist about my application for the Program, and disclose to them information contained in my application, in order to help me receive GlaxoSmithKline products under the Program and ensure that Program guidelines are being met;
4)Request information from my insurer, doctor, healthcare provider, or pharmacist about the prescribed medications I receive or will receive under the Program and about my medical condition. This information will be used only to determine my eligibility for the Program and to administer the Program. By signing below, I also authorize my insurer, doctor, healthcare provider, or pharmacist to release information about my prescribed medications and medical condition that is requested by GlaxoSmithKline, MSAZ or any company that GlaxoSmithKline uses to run the Program;
5)Contact my insurer, other potential funding sources, including the Centers for Medicare and Medicaid Services, social workers or patient advocacy organizations on my behalf in order to determine if I am eligible for health insurance coverage or other funds, and disclose to them information contained in my Program application or information about my prescribed medications and medical condition that has been provided by my physician, healthcare provider, or pharmacist;
6)Disclose any information obtained from the sources listed above to third parties if required by law.
I understand that this Authorization to Release and Disclose Medical Information will remain in effect for as long as I participate in the Program and for a period of 3 years after my participation in the Program ends.
I understand that my healthcare providers will not condition my medical treatment on my agreement to sign this Authorization to Release and Disclose Medical Information. I also understand that I have the right to revoke this authorization at any time by calling 1.866.PATIENT (1.866.728.4368) and
mailing a signed written statement of my revocation to the Program. Such a revocation would end my eligibility to participate in the Program. Revoking this authorization will prohibit disclosures after the date written revocation is received, except to the extent that action has been taken in reliance on my authorization.
I understand that once medical information about me has been disclosed in reliance upon this Authorization, the information may no longer be protected by federal privacy laws and may be further disclosed.
I understand that GlaxoSmithKline does not charge a fee for participation in this Program. There is a copayment for each prescription filled at a retail pharmacy. If my advocate charges a fee for enrollment or refills of my medicine, this money is not paid to GlaxoSmithKline.
I certify that I am not enrolled in any Medicare plan that includes Part D drug coverage. Furthermore, I certify that the information provided in this application is complete and accurate to the best of my knowledge and agree to notify GlaxoSmithKline of any change in my insurance eligibility or financial status.
______________________________________________________ |
____________ |
________________________________________ |
Applicant Signature |
Date |
Relationship (if other than Applicant) |
OPTIONAL: ADVOCATE INFORMATION
This section should be completed only if the advocate enrolls the applicant and wants to be the contact person and receive program correspondence for this applicant.
Advocate ID Number: ______________ (You must be a registered advocate. Register at www.BridgesToAccess.com or by calling 1.866.PATIENT)
Name (First):________________________________ (M.I.): ____________ (Last):_______________________________________
Facility Name:__________________________________________________________________________________________
Street Address: ____________________________________________________________________________________________
City:_________________________________________________________________ State:_______ ZIP Code:____________
Phone Number: (_______)
By my signature, I certify to the best of my knowledge, the information on this application is correct and complete. I have no knowledge of any intent to sell, barter or give this product to any person other than the Applicant for whom it has been prescribed. To the best of my knowledge, the Applicant has no medical/prescription insurance benefits for the indicated pharmaceutical(s), including Medicaid or other public programs other than as indicated, and the Applicant has insufficient financial resources to pay for the prescribed therapy.
___________________________________________________________________ |
________________________________________ |
Advocate Signature (Original signature required. Stamped signature not accepted.) |
Date |
PAGE 2 |
BtA Mail Rev. 04/10 |
Form Characteristics
| Fact Name | Description |
|---|---|
| Program Sponsor | Bridges to Access is a patient assistance program sponsored by GlaxoSmithKline. |
| Eligibility Criteria | Eligibility depends on household income and insurance status. |
| Application Submission | Completed applications must include income documentation and prescriptions. |
| Notification | Applicants receive mail notifications regarding their program qualification. |
| Initial Supply Duration | If approved, applicants can receive medicine for up to one year, starting with a 90-day supply. |
| Re-application Requirement | Applicants must re-apply annually to maintain eligibility for the program. |
| Contact Information | For questions or assistance, call 1.866.PATIENT or visit www.BridgesToAccess.com. |
| Medical Authorization | Applicants authorize GlaxoSmithKline and partners to access necessary medical information. |
| Compliance with Medicare | Applicants must certify they are not enrolled in any Medicare plan that includes Part D drug coverage. |
Guidelines on Utilizing Bridges Access Application
Filling out the Bridges Access Application form involves several key steps. Completing this application accurately is essential for those seeking assistance from the program. Once the form is filled out and submitted with the required documentation, applicants will await notification regarding their eligibility. If eligible, they can expect to receive 90 days of medication by mail.
- Begin by providing the Applicant Information. Fill in first name, middle initial, last name, mailing address, city, state, ZIP code, and phone number.
- Indicate the number of people who contribute to or are dependent on the household income.
- Complete the personal details such as gender, Social Security number, and birth date.
- Enter the total gross monthly or annual income. Include necessary documentation as instructed.
- Answer questions regarding Prescription Coverage, indicating any eligibility for state or federal programs.
- If applicable, fill out the Shipping Address section for where the medicine should be sent.
- List any known drug allergies and health conditions under the Allergy and Health Information section.
- Ensure that all parts of the form are completed. Incomplete applications may delay processing.
- Gather and include the necessary documentation: the completed application, proof of income, and signed original prescriptions for GlaxoSmithKline medications.
- Keep a copy of the entire application and documents for personal records.
- Sign the application, authorizing the release and disclosure of medical information where indicated.
What You Should Know About This Form
What is the Bridges Access Application form?
The Bridges Access Application form allows individuals to apply for assistance with GlaxoSmithKline medicines through the Bridges to Access program. This program helps eligible applicants based on household income and insurance status. To get started, you need to complete the application, provide necessary income documentation, and submit the prescription for the relevant medication.
Who is eligible to apply for the Bridges Access program?
Eligibility is determined by your household income and insurance coverage. To qualify, you must provide income documentation, which can include tax forms or recent pay stubs. Additionally, applicants must not have adequate insurance coverage for the prescribed GlaxoSmithKline medications. If there are any questions about specifics, you can reach out by calling 1.866.PATIENT or visiting the website.
How do I submit my application?
You can submit your completed application by mailing it to Bridges to Access at PO Box 29038, Phoenix, AZ 85038-9038. Ensure that you include all required documents, such as proof of income and your signed original prescription for a 90-day supply of the medication, along with any necessary re-fills.
How will I be notified if I qualify for the program?
If you qualify for the Bridges to Access program, you will receive a notification by mail. It's important to ensure that all your information is accurate and complete to help expedite the review process.
What happens if my application is approved?
Once your application is approved, you will be eligible to receive GlaxoSmithKline medicines for up to one year. The first 90-day supply will be mailed directly to you. Remember, at the end of that year, you must re-apply to continue receiving assistance.
Can I track the status of my application?
The Bridges to Access program does not provide a tracking system for applications. However, if you have questions about your application or need assistance, you can call 1.866.PATIENT for updates and support.
What should I do if my financial situation changes?
If there are any changes to your financial situation or insurance eligibility, you must notify GlaxoSmithKline promptly. Keeping them updated can affect your eligibility for the program and ensure you continue to receive the assistance you need.
Common mistakes
Filling out the Bridges Access Application form can be daunting, but avoiding common mistakes can streamline the process. One significant error is leaving the form incomplete. An incomplete application can lead to delays in processing. Make sure every section is filled out, even if it feels unnecessary. Every detail counts towards determining eligibility.
Another mistake applicants frequently make is neglecting to attach the required proof of income. This includes tax forms or pay stubs. If applicants have not filed taxes, it’s essential to provide proof of all income sources from the last 30 days. Failing to do this may result in disqualification or further delays. Review the income documentation checklist carefully and ensure all necessary documents accompany your application.
Applicants also often overlook the importance of their contact information. Inaccurate details, such as a misspelled name or wrong phone number, can prevent the program from reaching you. Ensure that the mailing address and phone number provided are accurate and up-to-date. Double-check spelling; even minor errors can complicate future communications.
Additionally, some make the mistake of not signing the application. A signature is required to validate the information provided. This includes not only the applicant’s signature but also that of an advocate, if applicable. Unsigned applications may be rejected outright, so always be sure to sign and date the form appropriately.
Providing information about prescription coverage often poses challenges. Some applicants fail to accurately disclose whether they are enrolled in any state or federal prescription programs. If the applicant answers incorrectly, it can lead to not qualifying for the assistance needed. Be thorough when answering these questions and consider calling customer support if uncertain.
Finally, applicants sometimes misunderstand the annual reapplication requirement. The program mandates that recipients must reapply each year. Being unaware of this requirement can lead to a lapse in receiving necessary medications. Mark your calendars and set reminders to ensure you reapply on time.
Documents used along the form
The Bridges Access Application form is an important step for patients seeking support from GlaxoSmithKline's patient assistance program. To ensure a smooth application process, several additional documents may be required. Below is a list of commonly used forms and documents that accompany the Bridges Access Application.
- Proof of Income: This may include recent pay stubs, unemployment statements, or Social Security communications. It must reflect the applicant's current financial status for the last 30 days.
- Previous Tax Return: A copy of the first page of the most recent tax return (1040, 1040A, or 1040EZ) may need to be attached if the applicant filed taxes or was listed as a dependent.
- Prescriptions: A signed original prescription for a 90-day supply of the necessary GlaxoSmithKline medication, including any eligible refills, must be provided.
- Authorization Form: A document signed by the applicant allowing GlaxoSmithKline to access medical information and communicate with healthcare providers on their behalf.
- Medical Records: Relevant health information or records related to the applicant’s eligibility may be required to support the application.
- Advocate Information: If an advocate enrolls the applicant, their details, including contact information, must be included to facilitate communication regarding the application.
- Contact Information: Current address and phone number ensure that important notifications regarding the application are delivered promptly.
Each of these documents plays a crucial role in the application process. An incomplete submission can lead to delays. To enhance your chances of approval, ensure that all necessary documentation is included with the Bridges Access Application form.
Similar forms
- Patient Assistance Program Application: Similar to the Bridges Access Application form, this document also seeks to determine eligibility for assistance in accessing prescription medications. Applicants must provide personal information, income details, and documentation to support their claims.
- Health Insurance Marketplace Application: Like the Bridges form, this application captures personal data, income information, and household composition. It is used to ascertain eligibility for health coverage through federal or state health insurance programs.
- Medicaid Application: This document functions similarly by collecting information on the applicant’s financial situation, household size, and health status. Medicaid eligibility is determined based on income and family dynamics, paralleling the Bridges Access process.
- Medicare Extra Help Application: This application evaluates an individual’s qualification for extra help with prescription drug costs. It requires detailed income information and personal data, which aligns closely with the Bridges Access Application form's requirements.
- Community Health Center Sliding Fee Scale Application: Applicants use this document to request reduced costs for health services based on income. It similarly requires personal and financial information, thus resembling the Bridges Access form in purpose and structure.
Dos and Don'ts
When filling out the Bridges Access Application form, it is essential to be thorough and precise. Following these guidelines can help ensure a smooth application process. Below is a list of important dos and don’ts for applicants.
- Do complete the entire form. An incomplete application can lead to delays in processing.
- Do provide accurate income documentation. Attach the necessary tax forms or recent proof of income from all sources.
- Do confirm that all prescription medications are written for a 90-day supply with appropriate refills if medically justified.
- Do ensure you keep a copy of the entire application along with all documents for your personal records.
- Do print the applicant’s name and date of birth on every document submitted.
- Don’t skip any required sections, especially regarding income and prescription coverage. This information is crucial for processing.
- Don’t assume your application will be processed without proof of income. All documentation must be provided.
- Don’t forget to sign the application. An unsigned application will not be accepted.
- Don’t submit the application without providing clear and detailed information about any known allergies or health conditions.
- Don’t hesitate to reach out for help. Call 1.866.PATIENT or visit the website for any questions or concerns.
Misconceptions
Misconceptions about the Bridges Access Application form can lead to confusion. Here are six common myths and the realities that clarify them:
- Myth: You don’t need proof of income to apply.
- Myth: Anyone can apply for benefits regardless of income.
- Myth: You only need to apply once; annual re-application is not required.
- Myth: Sending in an incomplete application has no impact.
- Myth: You do not need a prescription from a healthcare provider.
- Myth: There are no fees involved in this program.
Reality: Proof of income is essential. Applicants must provide documentation showing their household income. This can be in the form of recent pay stubs or tax forms.
Reality: Eligibility is based on household income and insurance status. Only those who meet specific criteria can qualify for the program.
Reality: Applicants must re-apply every year to continue receiving assistance. This ensures that eligibility is based on current financial status.
Reality: Incomplete applications will delay processing. It’s important to fill out every section carefully to avoid setbacks.
Reality: A signed prescription for a 90-day supply is required. This prescription should be for medications made by GlaxoSmithKline.
Reality: While there is no fee for participation in the program, there may be a copayment for each prescription filled at a pharmacy. Advocates cannot charge fees for handling applications.
Understanding these realities can help navigate the application process more effectively. For assistance or questions, feel free to reach out to Bridges to Access directly.
Key takeaways
When filling out and using the Bridges Access Application form, here are some important points to keep in mind:
- Complete all sections: Ensure that you fill out the entire form. Missing information can delay the processing of your application.
- Provide proof of income: You need to attach income documentation. This can be either a tax form or proof from the past 30 days like pay stubs or Social Security statements.
- Annual re-application: If approved, you will receive medication for up to one year. However, you must submit a new application annually to continue receiving assistance.
- Contact for help: If you have questions about the application process, feel free to call 1.866.PATIENT or visit the official website for additional information.
Browse Other Templates
Veteran Travel Reimbursement Claim Form,Claim for Travel Costs by Veterans,Travel Reimbursement Application for Veterans,Travel Expense Reimbursement Request,Veteran Beneficiary Travel Reimbursement Form,Request for Veteran Travel Expense Refund,Form - Timely submission of the VA 10-3542 can lead to quicker reimbursement and alleviate some financial stress associated with travel costs.
Snow Plowing Contracts - Payment terms, including billing frequency, are defined within this agreement.