Fill Out Your Capf 160 Form
The CAPF 160 form, known as the CAP Member Health History Form, plays a critical role in ensuring the health and safety of participants within the Civil Air Patrol (CAP). This form is designed to gather essential medical information that aids staff in identifying and addressing any pre-existing medical conditions during activities or encampments. Confidentiality is paramount; the information collected is for official use only and safeguarded from unauthorized access. Applicants must provide personal details, such as their name, age, and CAP identification number, alongside a comprehensive health history that includes allergies, medications, and various medical conditions that may affect performance. Detailed sections address current health issues, past surgical history, and dietary restrictions, offering a clear view of each member's unique health profile. Parents or guardians of minor cadets must also give consent for participation and the administration of necessary medical treatments if needed. With this structured approach, the CAPF 160 form ensures that each member's health needs are appropriately recognized and met while participating in CAP programs.
Capf 160 Example
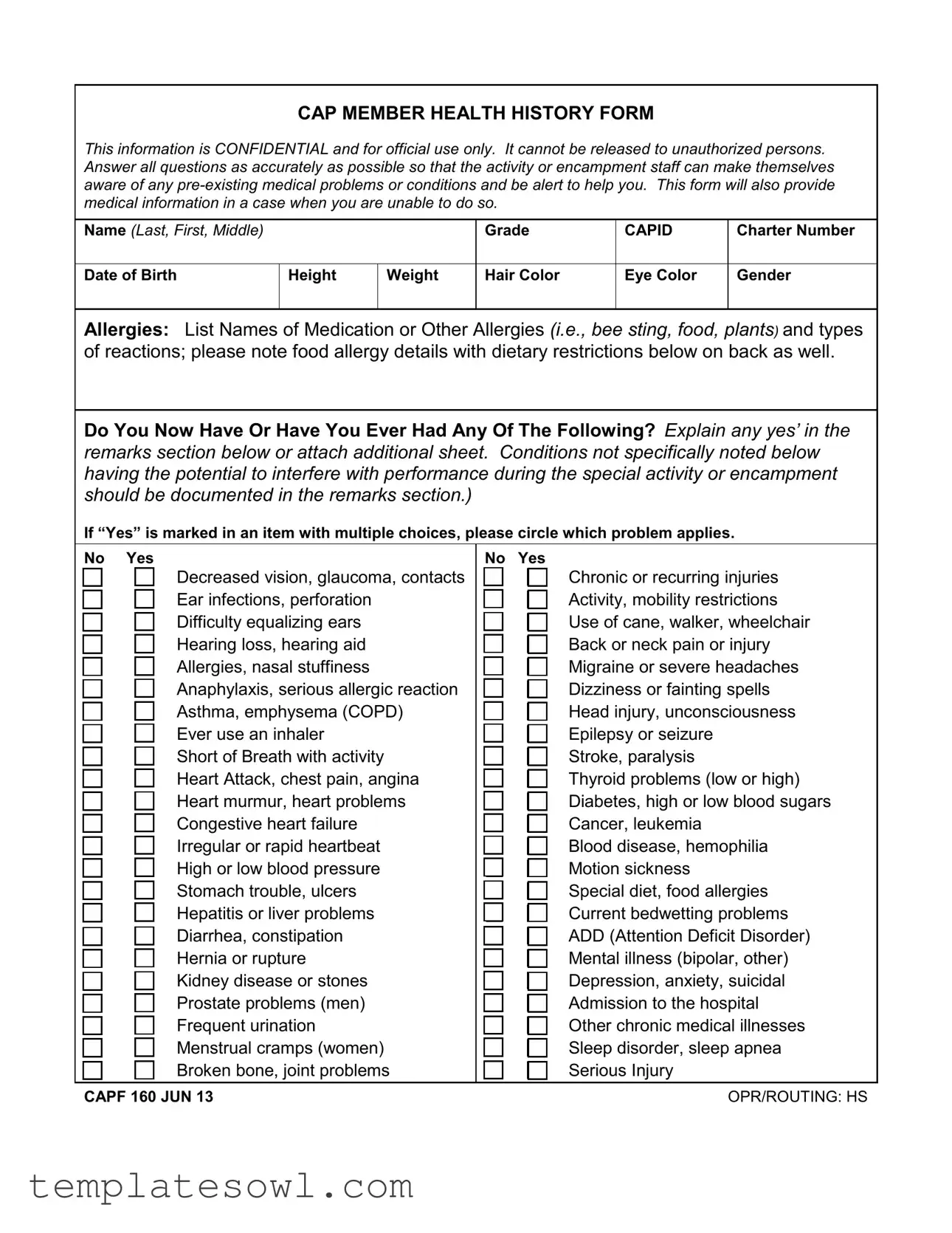
CAP MEMBER HEALTH HISTORY FORM
This information is CONFIDENTIAL and for official use only. It cannot be released to unauthorized persons. Answer all questions as accurately as possible so that the activity or encampment staff can make themselves aware of any
Name (Last, First, Middle)
Grade
CAPID
Charter Number
Date of Birth
Height
Weight
Hair Color
Eye Color
Gender
Allergies: List Names of Medication or Other Allergies (i.e., bee sting, food, plants) and types of reactions; please note food allergy details with dietary restrictions below on back as well.
Do You Now Have Or Have You Ever Had Any Of The Following? Explain any yes’ in the remarks section below or attach additional sheet. Conditions not specifically noted below having the potential to interfere with performance during the special activity or encampment should be documented in the remarks section.)
If “Yes” is marked in an item with multiple choices, please circle which problem applies.
|
No Yes |
|
No Yes |
||||||
|
|
|
|
Decreased vision, glaucoma, contacts |
|
|
|
|
Chronic or recurring injuries |
|
|
|
|
Ear infections, perforation |
|
|
|
|
Activity, mobility restrictions |
|
|
|
|
|
|
|
|
||
|
|
|
|
Difficulty equalizing ears |
|
|
|
|
Use of cane, walker, wheelchair |
|
|
|
|
|
|
|
|
||
|
|
|
|
Hearing loss, hearing aid |
|
|
|
|
Back or neck pain or injury |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
|
|
|
|
Allergies, nasal stuffiness |
|
|
|
|
Migraine or severe headaches |
|
|
|
|
|
|
|
|
||
|
|
|
|
Anaphylaxis, serious allergic reaction |
|
|
|
|
Dizziness or fainting spells |
|
|
|
|
|
|
|
|
||
|
|
|
|
Asthma, emphysema (COPD) |
|
|
|
|
Head injury, unconsciousness |
|
|
|
|
|
|
|
|
||
|
|
|
|
Ever use an inhaler |
|
|
|
|
Epilepsy or seizure |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
|
|
|
|
Short of Breath with activity |
|
|
|
|
Stroke, paralysis |
|
|
|
|
|
|
|
|
||
|
|
|
|
Heart Attack, chest pain, angina |
|
|
|
|
Thyroid problems (low or high) |
|
|
|
|
|
|
|
|
||
|
|
|
|
Heart murmur, heart problems |
|
|
|
|
Diabetes, high or low blood sugars |
|
|
|
|
|
|
|
|
||
|
|
|
|
Congestive heart failure |
|
|
|
|
Cancer, leukemia |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
|
|
|
|
Irregular or rapid heartbeat |
|
|
|
|
Blood disease, hemophilia |
|
|
|
|
|
|
|
|
||
|
|
|
|
High or low blood pressure |
|
|
|
|
Motion sickness |
|
|
|
|
|
|
|
|
||
|
|
|
|
Stomach trouble, ulcers |
|
|
|
|
Special diet, food allergies |
|
|
|
|
|
|
|
|
||
|
|
|
|
Hepatitis or liver problems |
|
|
|
|
Current bedwetting problems |
|
|
|
|
|
|
|
|
||
|
|
|
|
Diarrhea, constipation |
|
|
|
|
ADD (Attention Deficit Disorder) |
|
|
|
|
|
|
|
|
||
|
|
|
|
Hernia or rupture |
|
|
|
|
Mental illness (bipolar, other) |
|
|
|
|
|
|
|
|
||
|
|
|
|
Kidney disease or stones |
|
|
|
|
Depression, anxiety, suicidal |
|
|
|
|
|
|
|
|
||
|
|
|
|
Prostate problems (men) |
|
|
|
|
Admission to the hospital |
|
|
|
|
|
|
|
|
||
|
|
|
|
Frequent urination |
|
|
|
|
Other chronic medical illnesses |
|
|
|
|
|
|
|
|
||
|
|
|
|
Menstrual cramps (women) |
|
|
|
|
Sleep disorder, sleep apnea |
|
|
|
|
|
|
|
|
||
|
|
|
|
Broken bone, joint problems |
|
|
|
|
Serious Injury |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
CAPF 160 JUN 13 |
OPR/ROUTING: HS |
Dietary Restrictions or Limitations (List any dietary restrictions like food allergies, diabetes,
Past Surgical History (List all surgeries including tonsils, ear tubes, appendix, gall bladder, hernia, hysterectomy, heart, heart catheterization, bone and joint and all other surgeries.)
Date Tetanus
Booster
No Td or Tdap
Date:
|
Pneumonia |
Hepatitis Vaccine |
Vaccine |
No |
No |
Date: |
Date: |
|
|
Varicella Immuni- zation/chickenpox
No
Date:
Influenza Vaccine No
Date:
Medication Information - Include supplements,
|
|
Times |
|
Any Special Dosing or Storage |
|
Tablet |
taken |
Reason for |
Instructions (i.e., as needed, with |
Name of Medication/Inhaler |
Strength |
per day |
Medication |
meals, must be refrigerated, etc.) |
1. |
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
Social History
Tobacco Use (packs per day, years smoked, smokeless tobacco use)
Occupation (student or other)
Religious Preference
Remarks (Attach additional sheet if needed)
CONSENT FOR MINOR CADET PARTICIPATION, MEDICATIONS, TREATMENT
I give permission for full participation in CAP programs, subject to any limitations noted herein.
My signature below evidences my consent for my child/ward to possess and
In case of emergency, I understand every effort will be made to contact me. In the event I cannot be reached, I hereby give my permission to the licensed
___________________________ |
________________________________________________________________________________________________________ |
DATE |
SIGNATURE OF PARENT/GUARDIAN |
CAP Form 160 Reverse
Form Characteristics
| Fact Name | Details |
|---|---|
| Form Purpose | The CAPF 160 form serves to collect health history information from participants in Civil Air Patrol activities. This helps staff be aware of any medical conditions that may require attention. |
| Confidentiality | The information provided on this form is confidential. It is used solely for official purposes and cannot be shared with unauthorized individuals. |
| Required Details | Participants must provide personal information such as name, date of birth, height, weight, and a comprehensive list of medical conditions, allergies, and medication. |
| Parental Consent | For minors, a signature is required from a parent or guardian. This consent allows for participation and outlines medical treatment permissions in emergencies. |
| Usage Frequency | The CAPF 160 form must be completed and updated annually, ensuring all health information remains current and accurate for each participant. |
Guidelines on Utilizing Capf 160
Completing the CAPF 160 form is an important step in ensuring that all pertinent medical information is accurately recorded before participation in CAP programs. This form needs to be filled out carefully, as it will help staff provide the necessary support during activities. Follow the steps below to fill out the form correctly.
- Begin by entering your personal information. Write your name in the format of Last, First, Middle. Include your Grade, CAP ID, and Charter Number.
- Provide your Date of Birth, Height, Weight, Hair Color, Eye Color, and Gender.
- List any Allergies you have, including medication and other allergies, along with the type of reactions.
- Answer the questions about your current and past medical history. Mark 'Yes' or 'No' for any conditions you have or have had. Circle applicable issues if you answer 'Yes.'
- Make sure to explain any 'Yes' answers in the Remarks section or attach an additional sheet if necessary.
- Indicate any Dietary Restrictions or Limitations you may have, highlighting important food allergies or dietary needs.
- Detail your Past Surgical History, listing all surgeries you have undergone.
- Fill in the Vaccination History, noting dates for Tetanus Booster, Pneumonia, Hepatitis Vaccine, Varicella Immunization, and Influenza Vaccine.
- Provide Medication Information, including any supplements, over-the-counter medicines, or herbal products. Include specific instructions if applicable.
- Complete your Social History by indicating Tobacco Use and your Occupation.
- Note your Religious Preference if applicable.
- In the Remarks section, include any additional relevant information you feel is necessary.
- Finally, review the consent for minor cadet participation, medications, and treatment. Make sure to provide your signature and the date as the parent or guardian.
What You Should Know About This Form
What is the CAPF 160 form?
The CAPF 160, also known as the CAP Member Health History Form, is a document used by the Civil Air Patrol (CAP) to collect important health and medical information about participants. This form ensures that activity or encampment staff are aware of any pre-existing medical conditions so they can provide appropriate support and care.
Who needs to fill out the CAPF 160 form?
All participants in Civil Air Patrol activities, including cadets and adult members, must complete the CAPF 160 form. This includes any volunteer who plans to attend encampments or other CAP events where medical assistance may be required.
Why is the information on the CAPF 160 form confidential?
The information provided in the CAPF 160 form is confidential and for official use only. It is designed to protect the privacy of the individuals filling it out. Sharing this information with unauthorized persons is strictly prohibited to ensure that personal health details remain secure.
What types of medical information are required on the CAPF 160 form?
The form requests various types of medical information, including allergies (such as food or medication), current health conditions (like asthma or diabetes), past surgical history, and dietary restrictions. Providing accurate details helps staff to manage health-related issues during activities.
How should I handle allergies on the form?
If you have allergies, you must list them on the form, detailing the type of allergy and the reaction experienced. You can also indicate any dietary restrictions related to your allergies to help staff accommodate any special meal needs.
What if I have chronic health issues?
If you have any chronic health issues or medical conditions, you should specify them on the form. There is space for additional remarks, where you can explain any conditions not specifically listed. This ensures that staff are prepared to assist you as needed.
Is parental consent needed for minors?
Yes, if a participant is a minor, parental consent is required. The parent or guardian must sign the form, granting permission for their child to participate and receive medical treatment if necessary. This secures proper medical care in emergencies.
How should I indicate medication I am taking?
You should list any medications, including prescription, over-the-counter, and supplements, on the form. Note the dosage and specific instructions for use, such as whether the medication needs to be taken with food or stored in a certain way. This information is vital for the care staff to understand your needs.
What happens if I don’t fill out the form completely?
Incomplete forms can hinder the ability of the staff to provide necessary care and support. It is essential to answer all questions as accurately as possible and provide any extra information that might be relevant to your health during CAP activities.
Common mistakes
When filling out the CAPF 160 form, many individuals overlook critical details, leading to potential misunderstandings or complications. One common mistake is failing to provide accurate medical history. This section is crucial for ensuring that activity staff are aware of any pre-existing conditions that could affect participation. A misleading or incomplete medical history can result in insufficient care during emergencies.
Another frequent error involves neglecting to list all allergies. Participants often list only a few without elaborating on the severity of their reactions. It is essential to note not just medication allergies but also food allergies and any dietary restrictions. This information helps staff to accommodate participants during meals and activities safely.
People frequently misinterpret the health questions regarding previous medical conditions. A simple "yes" or "no" doesn’t suffice; it is important to provide explanations where necessary. If a participant has experienced any health issues listed, they should elaborate in the remarks section. Omitting this information can lead to misunderstandings about a participant’s health status.
Finally, a common oversight is inadequate documentation of medication details. Participants might forget to include over-the-counter medications, supplements, or any special dosing instructions. This omission can hinder staff from providing appropriate care. Accurate medication information ensures that everyone involved understands what a participant may need during an encampment, allowing for proper management of health needs.
Documents used along the form
The CAPF 160 form is essential for members participating in the Civil Air Patrol (CAP) programs, particularly to ensure their safety and well-being during activities or encampments. Several other forms and documents work in conjunction with it to provide important information and permissions. Below is a list of those documents.
- CAPF 161 - Youth Protection Policy: This form outlines the policies and procedures to protect youth participants in CAP activities. It emphasizes the importance of ensuring a safe environment and details the background checks required for adult leaders interacting with minors.
- CAPF 162 - Medical Release Form: This document authorizes medical treatment for participants in the event of an emergency. It allows caregivers to designate who can make medical decisions and provides critical health information to medical professionals if needed.
- CAPF 165 - Application for Membership: Essential for enrolling new members in the CAP. This form collects basic personal information, along with eligibility details necessary for processing membership applications and ensuring compliance with CAP guidelines.
- CAPF 18 - Report of Cadet Activity: Used to document the participation and activities of cadet members. This report helps staff track achievements and progress, ensuring cadets get recognized for their efforts and experiences during CAP events.
- CAPF 388 - Cadet Protection Policy Acknowledgment: This form confirms that cadets and their guardians understand the CAP’s policies regarding youth protection. It’s crucial for establishing an awareness of responsibilities and safety measures in place during activities.
These accompanying documents not only streamline the processing of information but also ensure that the needs of each cadet are addressed appropriately. Proper completion aids in creating a safe and effective program for all participants.
Similar forms
- Medical History Form: Similar to the CAPF 160 form, a medical history form collects a patient’s health background, including chronic conditions and allergies, to inform medical providers about necessary precautions during treatment.
- Emergency Contact Form: The CAPF 160 requires an emergency contact in case of medical situations, similar to emergency contact forms used in schools and organizations to ensure quick access to family or guardians in times of need.
- Informed Consent Form: Just as consent is given for medical treatment in the CAPF 160, informed consent forms in healthcare provide legal protection and ensure patients are aware of the risks involved in their treatment.
- Medication Administration Record (MAR): The medication section in the CAPF 160 is akin to a MAR, which tracks medications administered to individuals while documenting dosages, routes, and times for potential legal accountability.
- Physical Examination Form: Like the CAPF 160, a physical examination form summarizes the results of a medical exam, including any restrictions that may affect participation in physical activities or programs.
- Allergy Action Plan: An allergy action plan outlines specific protocols for individuals with known allergies. The CAPF 160 form asks about allergies to ensure proper management and response during events.
- Fitness Assessment Form: Similar to gathering health history, a fitness assessment form usually captures cardiovascular and strength metrics to ascertain readiness for physical activities, mirroring the physical evaluation aspect of the CAPF 160.
- Patient Registration Form: The CAPF 160 shares similarities with patient registration forms by capturing personal details like name, age, and contact information, essential for maintaining accurate health records.
Dos and Don'ts
When filling out the CAPF 160 form, it’s essential to follow some important guidelines to ensure accuracy and clarity.
- Provide complete and legible information. Use clear handwriting or type the details if possible.
- Answer all questions honestly. If unsure, it’s better to ask for help than to guess.
- Review all entries before submission. A careful review can prevent mistakes.
- Attach any extra information on a separate sheet if additional explanation is needed.
- Keep a copy of the filled form for your records. You might need it for future activities.
- Ensure that a parent or guardian signs the consent section if you are a minor.
- Submit the form ahead of the deadline to avoid last-minute issues.
However, there are also things to avoid when completing this form.
- Don’t leave any required fields blank. This can cause delays in processing.
- Avoid providing inaccurate or misleading information. This could put your health at risk during activities.
- Do not forget to mention any allergies or medical conditions. This is vital for your safety.
- Refrain from using jargon or abbreviations that may not be understood by the staff.
- Don’t neglect to update the form if there are changes to your health status.
- Do not ignore the importance of the consent section. It’s legally significant.
- Don’t rush through the form. Take your time to ensure everything is filled out correctly.
Misconceptions
Misconception 1: The CAPF 160 form is not important for participation.
Some believe that the form is merely a formality. In reality, this form is essential for ensuring the safety and well-being of all participants. It provides vital medical history and information that helps staff respond appropriately in case of a health issue.
Misconception 2: Completing the CAPF 160 form is optional.
This form is a requirement for participation. It must be filled out accurately to allow the encampment staff to be prepared for any medical needs. Skipping it could lead to unsafe situations during activities.
Misconception 3: I can skip the details about allergies or medical conditions.
Every detail matters. Omitting information could jeopardize a participant’s health during emergencies. Providing comprehensive data allows staff to act swiftly and effectively, which can be lifesaving.
Misconception 4: Parents do not need to sign the form for minors.
Parental consent is crucial. The signature confirms that parents or guardians understand their child's medical needs and consent to participation. This is particularly important when it comes to administering treatments in emergencies.
Misconception 5: The information on the CAPF 160 form is not confidential.
The content of this form is strictly confidential. It is meant solely for official use, and unauthorized individuals cannot access it. Participants can trust that their medical information is protected and handled with care.
Key takeaways
Filling out the CAPF 160 form accurately is crucial for the well-being of the participant. Here are key takeaways to ensure proper completion and use of the form:
- Confidentiality is Essential: The information provided on the CAPF 160 form is confidential and is intended for official use only. Unauthorized disclosure is prohibited.
- Be Thorough and Accurate: Answer all questions with care. Inaccuracies may compromise safety and preparedness at activities or encampments.
- Document Medical History: Clearly outline any pre-existing medical conditions, allergies, and past surgeries in the appropriate sections. Provide additional details in the remarks section if necessary.
- Establish Consent: For minors, a parent or guardian must provide signed consent for participation and medication administration. Ensure the consent section is completed to avoid potential issues.
- Update Regularly: Revise the form with any changes to health status or medications, particularly before major events. This helps in ensuring a prompt response to medical needs.
Browse Other Templates
Printable Bill of Sale - Both parties should keep their copies of the Bill of Sale for their records.
Dmv Release of Liability Printable Form - Under 21 driver's licenses have unique features to indicate the holder's age.
Hvac Contractor License Requirements - It emphasizes practical hands-on experience, requiring descriptions related to the tools commonly used in the trade.