Fill Out Your Carefirst Cancellation Form
The CareFirst Cancellation Form is an essential document for individuals looking to terminate their insurance coverage, specifically addressing medical and dental plans obtained through CareFirst in Maryland, Washington D.C., and Northern Virginia. This form is necessary for policy cancellations and does not apply to changes in dependent coverage. The first section of the form collects subscriber information, including names, addresses, and contact details. The second section requires details about the specific plans to be terminated, with an emphasis on the termination date, which usually must be the last day of the month. Reasons for cancellation can vary, including changes in financial circumstances, eligibility for Medicare, relocation, or changes in employment. Subscribers must provide their signatures to validate the request and confirm understanding of the termination process. Additionally, the form includes contact information for member services, emphasizing the importance of careful completion to avoid any complications with the cancellation of coverage.
Carefirst Cancellation Example
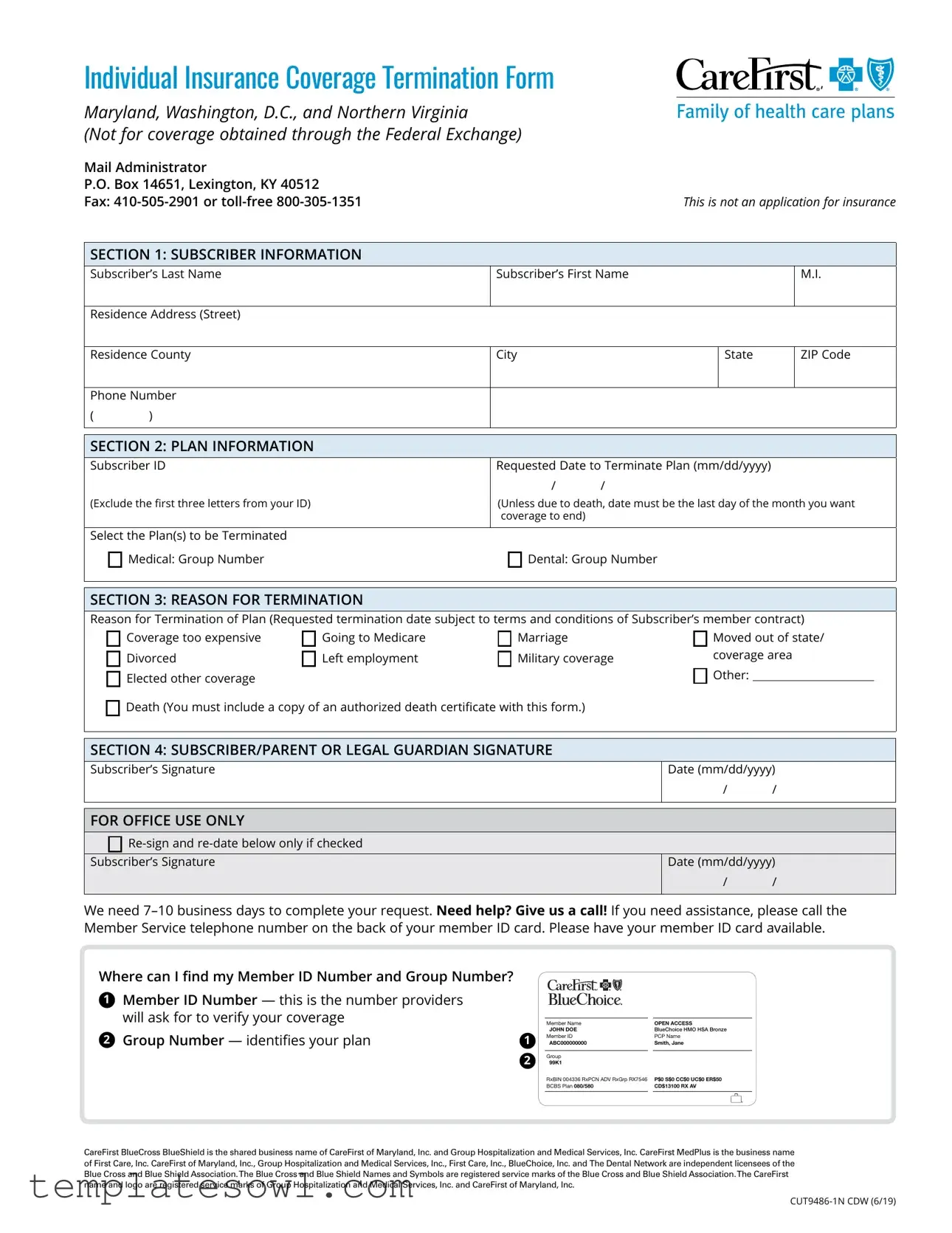
Individual Insurance Coverage Termination Form
Maryland, Washington, D.C., and Northern Virginia
(Not for coverage obtained through the Federal Exchange)
Mail Administrator |
|
P.O. Box 14651, Lexington, KY 40512 |
|
Fax: |
This is not an application for insurance |
SECTION 1: SUBSCRIBER INFORMATION
Subscriber’s Last Name |
Subscriber’s First Name |
M.I. |
|||
|
|
|
|
|
|
Residence Address (Street) |
|
|
|
|
|
|
|
|
|
|
|
Residence County |
City |
|
State |
ZIP Code |
|
|
|
|
|
|
|
Phone Number |
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION 2: PLAN INFORMATION |
|
|
|
|
|
Subscriber ID |
Requested Date to Terminate Plan (mm/dd/yyyy) |
|
|||
|
|
/ |
/ |
|
|
(Exclude the first three letters from your ID) |
(Unless due to death, date must be the last day of the month you want |
||||
|
|
coverage to end) |
|
|
|
|
|
|
|
|
|
Select the Plan(s) to be Terminated |
|
|
|
|
|
|
Medical: Group Number |
Dental: Group Number |
|
||
|
|
|
|
|
|
SECTION 3: REASON FOR TERMINATION
Reason for Termination of Plan (Requested termination date subject to terms and conditions of Subscriber’s member contract)
Coverage too expensive |
Going to Medicare |
Marriage |
Moved out of state/ |
|
Divorced |
Left employment |
Military coverage |
coverage area |
|
Elected other coverage |
|
|
Other: |
|
|
|
|
|
|
Death (You must include a copy of an authorized death certificate with this form.) |
|
|
||
SECTION 4: SUBSCRIBER/PARENT OR LEGAL GUARDIAN SIGNATURE
Subscriber’s Signature
Date (mm/dd/yyyy)
/ /
FOR OFFICE USE ONLY


Subscriber’s Signature
Date (mm/dd/yyyy)
/ /
We need
Member Service telephone number on the back of your member ID card. Please have your member ID card available.
Where can I find my Member ID Number and Group Number?
1Member ID Number — this is the number providers will ask for to verify your coverage
2Group Number — identifies your plan
1
2
Member Name |
|
OPEN ACCESS |
JOHN DOE |
|
BLUECHOICE HMO HSA BRONZE |
Member ID |
|
PCP Name |
ABC000000000 |
|
SMITH, JANE |
|
|
|
Group |
|
|
99K1 |
|
|
RxBIN 004336 RxPCN ADV RxGrp RX7546 |
|
P$0 S$0 CC$0 UC$0 ER$50 |
BCBS Plan 080/580 |
|
CD$13100 RX AV |
|
|
|
CareFirst BlueCross BlueShield is the shared business name of CareFirst of Maryland, Inc. and Group Hospitalization and Medical Services, Inc. CareFirst MedPlus is the business name of First Care, Inc. CareFirst of Maryland, Inc., Group Hospitalization and Medical Services, Inc., First Care, Inc., BlueChoice, Inc. and The Dental Network are independent licensees of the Blue Cross and Blue Shield Association.The Blue Cross and Blue Shield Names and Symbols are registered service marks of the Blue Cross and Blue Shield Association.The CareFirst name and logo are registered service marks of Group Hospitalization and Medical Services, Inc. and CareFirst of Maryland, Inc.
Individual Insurance Coverage Termination Form Guidelines
Before you start, please note: This form is used to cancel a POLICY. Do not use this form to make changes to your dependents on an existing policy you wish to keep. Use this form to cancel the following health insurance coverage:
■■Medical, dental, vision coverage if you enrolled directly through CareFirst.
■■Medical, dental coverage if you enrolled via the Maryland or DC Health Exchanges.
This form cannot be used to cancel the following health insurance coverage:
■■If you currently have coverage through your employer; you must work with your Human Resources department and/or plan administrator to terminate your coverage.
■■If you enrolled via the Virginia Federal Facilitated Exchange (FFE); please contact the FFE to terminate your coverage.
■■If a subscriber is deceased and he/she enrolled via the Exchange, please contact the appropriate Exchange to cancel subscriber’s policy.
Below is the most recent contact information.
|
NAME |
WEBSITE |
CUSTOMER SUPPORT |
MD |
Maryland Health Connection |
marylandhealthconnection.gov |
|
D.C. |
DC Health Link |
dchealthlink.com |
|
|
|
|
|
VA |
FFE |
HealthCare.gov |
|
|
|
|
|
Termination effective dates
Request cancellation by the last day of the month you want your coverage to end.
Note: If you fail to pay premiums for the coverage period prior to your termination date, your coverage may be terminated
due to
Retroactive termination requests
Retroactive terminations, i.e., termination dates in the past, are only permitted in the event of the subscriber’s death. A copy of the subscriber’s death certificate must be submitted with this Termination Form.
Cancelling a termination request
If you submit a termination form but then decide to keep your coverage, it may be possible to withdraw your termination
request. Please note:
■■You cannot withdraw a termination request if you have coverage through the Maryland or DC Health Exchanges.
■■For coverage obtained directly from CareFirst
The withdraw request must be received by CareFirst in writing.
If you are enrolled in a grandfathered plan (you enrolled in a plan before March 23, 2010), you may not be able to
Coverage change due to open enrollment
Switching plans during Open Enrollment does NOT automatically cancel your current coverage. Termination requests must be submitted for the following:
■■Changing and switching from an
■■Switching to an employer plan.
■■Changing health insurers.
■■Moving out of state.
If you do not terminate your old plan by December 31, your premium payment for that plan will be due on January 1.
2 |
Notice of Nondiscrimination and Availability of Language Assistance Services
(UPDATED 8/5/19)
CareFirst BlueCross BlueShield, CareFirst BlueChoice, Inc., CareFirst Diversified Benefits and all of their corporate affiliates (CareFirst) comply with applicable federal civil rights laws and do not discriminate on the basis of race, color, national origin, age, disability or sex. CareFirst does not exclude people or treat them differently because of race, color, national origin, age, disability or sex.
CareFirst:
■Provides free aid and services to people with disabilities to communicate effectively with us, such as:
 Qualified sign language interpreters
Qualified sign language interpreters
 Written information in other formats (large print, audio, accessible electronic formats, other formats)
Written information in other formats (large print, audio, accessible electronic formats, other formats)
■Provides free language services to people whose primary language is not English, such as:
 Qualified interpreters
Qualified interpreters
 Information written in other languages
Information written in other languages
If you need these services, please call
If you believe CareFirst has failed to provide these services, or discriminated in another way, on the basis of race, color, national origin, age, disability or sex, you can file a grievance with our CareFirst Civil Rights Coordinator by mail, fax or email. If you need help filing a grievance, our CareFirst Civil Rights Coordinator is available to help you.
To file a grievance regarding a violation of federal civil rights, please contact the Civil Rights Coordinator as indicated below. Please do not send payments, claims issues, or other documentation to this office.
Civil Rights Coordinator, Corporate Office of Civil Rights
Mailing Address |
P.O. Box 8894 |
|
Baltimore, Maryland 21224 |
Email Address |
civilrightscoordinator@carefirst.com |
Telephone Number |
|
Fax Number |
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights electronically through the Office for Civil Rights Complaint portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf or by mail or phone at:
U.S. Department of Health and Human Services 200 Independence Avenue, SW
Room 509F, HHH Building
Washington, D.C. 20201
Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html.
CareFirst BlueCross BlueShield is the shared business name of CareFirst of Maryland, Inc. and Group Hospitalization and Medical Services, Inc. CareFirst of Maryland, Inc., Group Hospitalization and Medical Services, Inc., CareFirst BlueChoice, Inc., The Dental Network and First Care, Inc. are independent licensees of the Blue Cross and Blue Shield Association. In the District of Columbia and Maryland, CareFirst MedPlus is the business name of First Care, Inc. In Virginia, CareFirst MedPlus is the business name of First Care, Inc. of Maryland (used in VA by: First Care, Inc.). The Blue Cross® and Blue Shield® and the Cross and Shield Symbols are registered service marks of the Blue Cross and Blue Shield Association, an association of independent Blue Cross and Blue Shield Plans.
Foreign Language Assistance
Attention (English): This notice contains information about your insurance coverage. It may contain key dates and you may need to take action by certain deadlines. You have the right to get this information and assistance in your language at no cost. Members should call the phone number on the back of their member identification card. All others may call
አማርኛ (Amharic) ማሳሰቢያ፦ ይህ ማስታወቂያ ስለ መድን ሽፋንዎ መረጃ ይዟል። ከተወሰኑ
Èdè Yorùbá (Yoruba) Ìtẹ́tíléko: Àkíyèsí yìí ní ìwífún nípa iṣẹ́adójútòfò rẹ. Ó le ní àwọn déètì pàtó o sì le ní láti gbé ìgbésẹ̀ní àwọn ọjọ́gbèdéke kan. O ni ẹ̀tọ́láti gba ìwífún yìí àti ìrànlọ́wọ́ní èdè rẹ lọ́fẹ̀ẹ́. Àwọn
Tiếng Việt (Vietnamese) Chú ý: Thông báo này chứa thông tin về phạm vi bảo hiểm của quý vị. Thông báo có thể chứa những ngày quan trọng và quý vị cần hành động trước một số thời hạn nhất định. Quý vị có quyền nhận được thông tin này và hỗ trợ bằng ngôn ngữ của quý vị hoàn toàn miễn phí. Các thành viên nên gọi số điện thoại
ởmặt sau của thẻ nhận dạng. Tất cả những người khác có thể gọi số
Tagalog (Tagalog) Atensyon: Ang abisong ito ay naglalaman ng impormasyon tungkol sa nasasaklawan ng iyong insurance. Maaari itong maglaman ng mga pinakamahalagang petsa at maaaring kailangan mong gumawa ng aksyon ayon sa ilang deadline. May karapatan ka na makuha ang impormasyong ito at tulong sa iyong sariling wika nang walang gastos. Dapat tawagan ng mga Miyembro ang numero ng telepono na nasa likuran ng kanilang identification card. Ang lahat ng iba ay maaaring tumawag sa
Español (Spanish) Atención: Este aviso contiene información sobre su cobertura de seguro. Es posible que incluya fechas clave y que usted tenga que realizar alguna acción antes de ciertas fechas límite. Usted tiene derecho a obtener esta información y asistencia en su idioma sin ningún costo. Los asegurados deben llamar al número de teléfono que se encuentra al reverso de su tarjeta de identificación. Todos los demás pueden llamar al
Русский (Russian) Внимание! Настоящее уведомление содержит информацию о вашем страховом обеспечении. В нем могут указываться важные даты, и от вас может потребоваться выполнить некоторые действия до определенного срока. Вы имеете право бесплатно получить настоящие сведения и сопутствующую помощь на удобном вам языке. Участникам следует обращаться по номеру телефона, указанному на тыльной стороне идентификационной карты. Все прочие абоненты могут звонить по номеру
हिन्दी (Hindi) ध्यान दें: इस सचनाू मेंआपकी बीमा कवरेजकेबारेमेंजानकारी दी गई िै।िो सकता िैकक इसमेंख्यु ततथियों का उल्लेखिो और आपकेललए ककसी तनयत
कर हदया जाएगा। |
|
|
|
|
|
|
wa mo! B ̃̌nyu nyu hw |
|
|
|
|
|
|
|
|
|
|
|
fuà ṹá tìǐ |
|
|
|
|
|
|
|
|
|
̃̌gbo- |
||||||||||||||||||||||||
s |
ù |
|
|
|
|
|
|
|
|
|
|
|
|
a |
|
zi |
|
m |
|
|
b |
|
|
|
k |
||||||||||||||||||||||||||||
Ɓǎ ɔ́ɔ̀ ɖ |
|
|
|
Tò Ɖùǔ Cá |
|
ɔ nìà |
|
ɛ ɓá |
|
ɔ ɓě ké m̀ |
|
p |
|
|
kpá ɓó nì |
|
ɛɛ jè dyí |
|
ɔ nìà ɛ |
||||||||||||||||||||||||||||||||||
- |
m |
|
|
|
|
|
|
|
- |
ɔ́m̀ké |
|
|
|
|
ɛɛ |
|
se |
|
|
|
|
|
. Kpoo |
ny |
|
|
|
m |
|
|
f |
̃̌ |
|
|
ɛ kè |
|
|||||||||||||||||
ɓéɖé wé ɛ́ɛ́ɓě ɓɛ́m̀ké ɖɛ |
|
|
|
|
k |
|
ny |
|
|
ɛ̀ɓɛ́wé ɓě |
|
ké |
|
. Ɔ |
|
ɔ̀nì kpé ɓɛ́m̀ké |
|
|
ɔ nìà |
|
k |
||||||||||||||||||||||||||||||||
|
|
|
(Bassa) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
gbo |
|
|
|
ɔ̀ |
|
|
|
|
|
|
- n ny |
|
|
|
|
|
|
. B |
|
||||||||||||
kpá kpá m̀ ɔ́ɛɛdyé ɖé nì ɓíɖí wùɖù mú ɓɛ́m̀ké |
|
|
wíɖí ɖò |
|
ɛ́ɛ̀ |
|
|
|
|
ɔ ɓě |
|
|
ɛ ɖá |
ṹ |
|
|
|
ɔ̀ɓànìà ɖé waà |
|||||||||||||||||||||||||||||||||||
n |
káàɔ̀ɖeí |
|
ɛ |
|
|
ɔ |
ɔ̀ɔ̀séí |
|
|
ɛ ɖá |
|
ɔ̀ɓànìà |
ɛ |
|
|
|
̃̌ |
|
|
|
|
|
ké m̀ |
ɛ fò |
|
|
ɓɛ́ |
|
kéɛ m̀ |
|
|
|
ɛ ɓɛ́m̀ké |
||||||||||||||||||||
ɔ̀ɓà ɔ̀à |
wu u |
|
|
|
. |
|
|
|
ɛ̀. Ɔ jǔ ké |
|
|
ɔ ɖò |
|
|
m̀ |
|
|
|
|
|
|
ɖ |
m̀ |
|
|
ɔ́ |
|
ɛ |
|
|
ɛ |
ké |
|
|
ɔ ɖò |
|
|
|
ɓó nìì |
||||||||||||||
|
ɛɛ |
|
pàɖàì |
|
|
|
|
|
|
ɔ jǔǐ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
I.D. |
|
n ny . Ny |
t |
|
|
n m |
|
n |
|
|
|
|
|
k : |
|
|
|
|
|
|
|
tee |
|
|
wa |
|
|
|
|
|
gbo c |
|
|
|
|||||||||||||||||||
ɓɛ́ɔ ké nì |
|
ɖ |
ɔ̀mú zà |
|
n hw |
|
|
|
|
|
ny |
|
dyi |
|
g |
|
n, po wu u |
|
m po |
dyi , |
|
ny |
|
|
|
mu |
|
n |
|||||||||||||||||||||||||
|
m |
0 k |
dyi |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
বাাংলা (Bengali) লক্ষ্য করুন: এই ননাটিশে আপনার ববমা কভাশরজ সম্পশকেতথ্য রশেশে। এর মশযয গুরুত্বপূর্েতাবরখ থ্াকশত পাশর এবাং বনবদেষ্টতাবরশখর মশযয আপনাশক পদশক্ষ্প বনশত হশত পাশর। ববনা খরশে বনশজর ভাষাে এই তথ্য পাওোর এবাং সহােতা পাওোর অবযকার আপনার আশে। সদসযশদরশক তাশদর পবরেেপশের বপেশন থ্াকা নম্বশর কল করশত হশব। অশনযরা
نکمم روا ںیہ یتکس وہ ںیخیرات یدیلک ںیم سا ۔ےہ لمتشم رپ تامولعم قلعتم ےس جیروک سنیروشنا ےک پآ سٹون ہی: ہجوت )Urdu( ودرا ہچرخ ریغب روا ےنرک لصاح تامولعم ہی ساپ ےک پآ ۔ےڑپ ترورض یک ےنرک یئاورراک کت ںوخیرات یرخآ صوصخم وک پآ ہک ےہ رگید یھبس ۔ےیہاچ ینرک لاک رپ ربمن نوف دوجوم رپ تشپ یک ڈراک یتخانش ےنپا وک ناربمم ۔ےہ قح اک ےنرک لصاح ددم ںیم نابز ینپا ےیک نابز ہبولطم ینپا رپ ےنید باوج ےک ٹنجیا ۔ںیرک راظتنا کت ےناج ےہک وک ےنابد 0 روا ںیہ ےتکس رک لاک
خیرات ات تسا مزلا و دشاب یمھم یاه خیرات یواح تسا نکمم .تسا امش همیب ششوپ هرابرد یتاعلاطا یواح هیملاعا نیا :هجوت )Farsi( یسراف
.دینک تفایرد ناتدوخ نابز هب ناگیار تروص هب ار ییامنهار و تاعلاطا نیا ات دیتسه رادروخرب قح نیا زا امش .دینک مادقا یصاخ هدش ررقم هرامش اب دنناوت یم دارفا ریاس .دنریگب سامت ناشییاسانش تراک تشپ رد هدش جرد هرامش اب دیاب اضعا نابز ،اهروتارپا زا یکی طسوت ییوگخساپ زا دعب .دنهد راشف ار 0 ددع دوش هتساوخ اھنآ زا ات دننامب رظتنم و دنریگب
.دیوش لصو هطوبرم مجرتم هب ات دینک میظنت ار زاین دروم
ذاختا ىلإ جاتحت دقو ،ةمھم خیراوت ىلع يوتحی دقو ،ةینیمأتلا كتیطغت نأشب تامولعم ىلع راطخلإا اذه يوتحی: هیبنت (Arabic) ةیبرعلا ةغللا لاصتلاا ءاضعلأا ىلع يغبنی. ةفلكت يأ لمحت نودب كتغلب تامولعملاو ةدعاسملا هذه ىلع لوصحلا كل قحی. ةددحم ةیئاھن دیعاوم لولحب تاءارجإ مقرلا ىلع لاصتلاا نیرخلآل نكمی. مھب ةصاخلا ةیوھلا فیرعت ةقاطب رھظ يف روكذملا فتاھلا مقر ىلع اھب لصاوتلا ىلإ جاتحت يتلا ةغللا ركذا ،ءلاكولا دحأ ةباجإ دنع 0. مقر ىلع طغضلا مھنم بلطی ىتح ةثداحملا للاخ راظتنلااو
.نییروفلا نیمجرتملا دحأب كلیصوت متیسو
中文繁体 (Traditional Chinese) 注意:本聲明包含關於您的保險給付相關資訊。本聲明可能包含重要日期 及您在特定期限之前需要採取的行動。您有權利免費獲得這份資訊,以及透過您的母語提供的協助服 務。會員請撥打印在身分識別卡背面的電話號碼。其他所有人士可撥打電話
Igbo (Igbo) Nrụbama: Ọkwa a nwere ozi gbasara mkpuchi nchekwa onwe gị. Ọ nwere ike ịnwe ụbọchị ndị dị mkpa, ị nwere ike ịme ihe tupu ụfọdụ ụbọchị njedebe. Ị nwere ikike ịnweta ozi na enyemaka a n’asụsụ gị na akwụghị ụgwọ ọ bụla. Ndị otu kwesịrị ịkpọ akara ekwentị dị n’azụ nke kaadị njirimara ha. Ndị ọzọ niile nwere ike ịkpọ
Deutsch (German) Achtung: Diese Mitteilung enthält Informationen über Ihren Versicherungsschutz. Sie kann wichtige Termine beinhalten, und Sie müssen gegebenenfalls innerhalb bestimmter Fristen reagieren. Sie haben das Recht, diese Informationen und weitere Unterstützung kostenlos in Ihrer Sprache zu erhalten. Als Mitglied verwenden Sie bitte die auf der Rückseite Ihrer Karte angegebene Telefonnummer. Alle anderen Personen rufen bitte die Nummer
Français (French) Attention: cet avis contient des informations sur votre couverture d'assurance. Des dates importantes peuvent y figurer et il se peut que vous deviez entreprendre des démarches avant certaines échéances. Vous avez le droit d'obtenir gratuitement ces informations et de l'aide dans votre langue. Les membres doivent appeler le numéro de téléphone figurant à l'arrière de leur carte d'identification. Tous les autres peuvent appeler le
한국어(Korean) 주의: 이 통지서에는 보험 커버리지에 대한 정보가 포함되어 있습니다. 주요 날짜 및 조치를 취해야 하는 특정 기한이 포함될 수 있습니다. 귀하에게는 사용 언어로 해당 정보와 지원을 받을 권리가 있습니다. 회원이신 경우 ID 카드의 뒷면에 있는 전화번호로 연락해 주십시오. 회원이 아니신 경우
(Navajo)
Form Characteristics
| Fact Name | Description |
|---|---|
| Usage | This form is used specifically to terminate individual insurance coverage, including medical and dental plans, for residents of Maryland, Washington D.C., and Northern Virginia. |
| Mailing Address | Completed forms should be mailed to the Administrator at P.O. Box 14651, Lexington, KY 40512. |
| Termination Date | The termination date must be the last day of the month in which the subscriber wants coverage to end unless it is due to the subscriber's death. |
| Eligibility Criteria | Eligibility to use this form excludes coverage obtained through the Federal Exchange or employer-sponsored plans. |
| Assistance Contact | If help is needed, subscribers can contact Member Services using the number on the back of their member ID card. |
| Governing Law | This form operates under the regulations established in Maryland, Washington D.C. and Virginia, dictated by state-specific insurance laws. |
Guidelines on Utilizing Carefirst Cancellation
After completing the CareFirst Cancellation form, it is essential to understand that you will send it to the designated address or fax number provided. Once submitted, the request may take 7 to 10 business days to process. If you have questions or need assistance, you can reach out to member services using the contact number on your ID card.
- Begin by filling in the Subscriber Information. Enter your last name, first name, and middle initial.
- Provide your complete residence address, including street, county, city, state, and ZIP code.
- Enter your phone number in the designated space.
- In the Plan Information section, write your Subscriber ID, excluding the first three letters.
- Specify the Requested Date to Terminate Plan. Keep in mind that this date must be the last day of the month you want the coverage to end.
- Select which options you wish to terminate, such as Medical or Dental, and include any relevant group numbers.
- In the Reason for Termination section, mark the reason for cancellation. If it is due to death, include a death certificate with your form.
- Sign and date the form in the Subscriber/Parent or Legal Guardian Signature section.
- Review the completed form to ensure all information is accurate and complete before submission.
- Mail or fax the completed form to CareFirst at the address or fax number listed on the form.
What You Should Know About This Form
What is the Carefirst Cancellation form used for?
The Carefirst Cancellation form is designed to officially cancel your individual insurance coverage with CareFirst. Whether you need to terminate your medical, dental, or vision insurance, this form is necessary for your request to be processed. Keep in mind that it can't be used for changes to dependents or for coverage obtained via employer or federal exchanges.
How do I fill out the Carefirst Cancellation form?
To complete the form, provide your personal information such as your name, address, and phone number. You'll also need to indicate your Subscriber ID and the group number for your plan. Then, select the reason for termination from a list, including options like moving out of state or switching to Medicare. Finally, sign and date the form before submitting it.
Where should I send the completed form?
Your completed cancellation form should be mailed to CareFirst at P.O. Box 14651, Lexington, KY 40512. Alternatively, you can fax it to 410-505-2901 or their toll-free number 800-305-1351. Keep a copy of the form for your records before sending it.
When will my coverage officially end after I submit the form?
Your requested cancellation will typically take effect on the last day of the month you specify. Make sure to submit the form at least 7–10 business days in advance to ensure it’s processed in time. If premiums are unpaid before your desired termination date, coverage may end due to non-payment.
Can I cancel my cancellation request?
If you change your mind after submitting the cancellation form, you might be able to withdraw your request. However, this must be done in writing. Be aware that if your coverage was obtained through the Maryland or DC Health Exchanges, you cannot withdraw the cancellation.
What happens if I miss the cancellation deadline?
If you don’t submit your cancellation by the last day of the month, you’ll need to pay the premium for the next month. It's crucial to get your form in on time to avoid unexpected charges.
Can I request a retroactive cancellation?
Retroactive cancellations are only allowed if the request is due to the subscriber's death. In that case, a copy of the death certificate must accompany the cancellation form for processing.
What if I have further questions or need help?
If you have additional questions about the cancellation process or need assistance, contact CareFirst's Member Service number located on the back of your member ID card. Having your member ID card handy will help facilitate the conversation.
Common mistakes
When completing the CareFirst Cancellation Form, individuals often make several common mistakes that can delay the process. One prevalent error is not providing complete subscriber information. The form requires specific details such as the subscriber's last name, first name, middle initial, residence address, and phone number. Leaving out any of this crucial information may lead to complications in processing the cancellation.
Another mistake occurs in the **selected termination date** section. To ensure the cancellation is effective by the desired date, it is essential to specify the last day of the month when you want the coverage to end. Many individuals mistakenly submit a date that does not align with this requirement, resulting in unexpected charges or prolonged insurance coverage.
Additionally, people sometimes choose the wrong reason for termination. The form includes various options, such as moving out of state, marriage, or going to Medicare. Selecting an incorrect reason can create confusion and possibly require additional documentation or clarification.
Failing to include the **Subscriber ID** is another frequent oversight. This identification number is critical for the provider to locate the correct policy. Without it, processing the cancellation may take significantly longer, which can be frustrating for the subscriber looking for a timely resolution.
Many also overlook the need for signatures. In Section 4, the subscriber or their legal guardian must sign and date the form. Failing to do this can lead to immediate rejection of the request, prolonging the cancellation process unnecessarily.
Finally, individuals often forget to check the mailing instructions. Sending the form to the wrong address or not using the correct method of submission can result in delays. CareFirst specifies that submissions should be sent to a specific P.O. Box or can be faxed. Ignoring these details could mean your cancellation does not go through as intended.
Documents used along the form
Along with the Carefirst Cancellation form, there are several other forms and documents that may be useful during the cancellation process. Here’s a brief description of each commonly used document.
- Proof of Coverage Form: This document verifies current coverage details with Carefirst. It may be required when transitioning to another insurance provider or when applying for new coverage.
- Change of Address Form: If the subscriber has moved, this form updates Carefirst with the new address. Accurate information is important for receiving necessary documents and communications.
- Dependent Removal Request: For subscribers who need to remove dependents from their policy, this form specifies which dependents are being removed and the effective date.
- Medicare Enrollment Form: When transitioning to Medicare, this document enrolls the individual in Medicare, ensuring eligible benefits are established properly.
- Withdrawal of Cancellation Request: If the subscriber changes their mind about cancelling, this document formally requests to withdraw the cancellation submitted earlier.
- Death Certificate: This form is required if the cancellation request is due to the subscriber's death. An official copy must accompany the cancellation form.
Understanding these documents can help streamline the cancellation process and ensure all necessary steps are followed correctly. Having the appropriate paperwork ready can prevent delays and complications.
Similar forms
- Insurance Policy Cancellation Request: This document serves a similar purpose as the Carefirst Cancellation form, allowing individuals to formally request the termination of their insurance policies. Both require personal information and reasons for cancellation.
- Health Insurance Termination Notice: Like the Carefirst form, this notice is typically used to communicate the end of health insurance coverage. It outlines the necessary steps and information needed to process the termination.
- Disenrollment Form: This form allows individuals to disenroll from their health plans, similar to the Carefirst Cancellation form. It also requires identifying details and a reason for disenrollment.
- Medicare Coverage Termination Request: Individuals wishing to stop their Medicare coverage must submit this request, which parallels the Carefirst form in structure and function, asking for subscriber details and reasons for termination.
- Long-term Care Insurance Cancellation Form: This form is used to cancel long-term care insurance policies. Like the Carefirst Cancellation form, it requires subscriber information, selected plans for termination, and reasons for cancellation.
- Dental Insurance Cancellation Request: This document works in a similar manner as the Carefirst Cancellation form, allowing subscribers to request termination of their dental coverage while collecting necessary personal information and reasons for ending coverage.
- Vision Insurance Termination Form: Much like the Carefirst Cancellation form, this document is utilized to terminate vision insurance coverage and requires details about the subscriber and the reason for the request.
Dos and Don'ts
When filling out the Carefirst Cancellation form, there are important guidelines to follow. Here are five key actions to take and avoid:
- Do ensure accuracy: Provide correct information for each section, including names, addresses, and subscriber IDs, to prevent delays.
- Do submit timely requests: Send your cancellation request by the last day of the month you want coverage to end.
- Do include necessary documentation: If cancelling due to a death, include a copy of the death certificate.
- Do contact customer service if needed: If you require assistance, use the Member Service number on your ID card for help.
- Do not use the form for dependents: This form is exclusively for terminating a policy and cannot be used to change coverage for dependents.
- Do not request retroactive termination: Retroactive termination is only allowed in the case of subscriber death if accompanied by proper documentation.
- Do not assume coverage is cancelled: Until you receive confirmation from Carefirst, continue to check your coverage status.
- Do not submit a termination after December 31: Failure to terminate your plan by this date means you will owe the premium for the next year.
Misconceptions
- Form is for Insurance Applications: Many believe that the CareFirst Cancellation Form is an application to obtain insurance. In fact, it is strictly a termination form and cannot be used to apply for new coverage.
- Can Cancel Through Third Parties: Some think they can cancel their insurance coverage through representatives or third parties. However, the cancellation must be initiated by the subscriber themselves using the official form.
- Immediate Cancellation: A common misconception is that submitting the form results in an immediate cancellation. The effective date of termination follows specific guidelines and typically ends on the last day of the month in which the request is submitted.
- Retroactive Cancellations Allowed: Individuals often assume they can cancel their coverage retroactively. Retroactive terminations are only permitted in cases of a subscriber’s death, and relevant documentation is required for such requests.
- Withdrawal of Cancellation is Easy: While some believe that withdrawing a cancellation request is straightforward, the ability to do so depends on how the insurance was obtained. If obtained via Maryland or D.C. Health Exchanges, the withdrawal is not possible.
- Can Use to Change Dependent Coverage: People might think they can use this form to make changes regarding dependents. In reality, this form cannot be used for modifying dependent coverage on an existing policy.
- Cancellation Does Not Require Reason: Many assume they can cancel their coverage without providing a reason. The form requires subscribers to indicate a reason for termination, which is a necessary part of the process.
Key takeaways
Key Takeaways for Filling Out the Carefirst Cancellation Form
- Only use this form if you want to cancel your insurance policy. This form is not for making changes to existing coverage.
- Provide all requested subscriber information accurately, including your name, address, and phone number.
- Specify the date you want your coverage to end. It must be the last day of the month you are canceling, except in the case of death.
- List the specific plan(s) you wish to terminate, such as medical or dental coverage.
- State the reason for cancellation clearly. Make sure to refer to the approved reasons, like moving, divorce, or financial constraints.
- Submit the completed form through mail or fax to the designated addresses provided by Carefirst.
- If you change your mind after submitting the form, you may be able to withdraw the cancellation request, but this process varies depending on how you enrolled.
- Allow 7-10 business days for your cancellation request to be processed and finalized.
Browse Other Templates
Florida Lottery Winner Redemption Form,Prize Claim Request Form,Lottery Prize Collection Form,Winning Ticket Claim Application,Lottery Payout Claim Form,Jackpot Winner Submission Form,Lottery Reward Application,Claimant Prize Submission Form,Florida - Take care to complete each section accurately to prevent processing delays.
New York State Renters Tax Credit - It is also important to keep a copy for personal records after submitting the form.
Florida Association of Realtors Forms - All notices between the parties must be delivered in writing, ensuring clear communication regarding contract matters.