Fill Out Your Child Adolescent Health Form
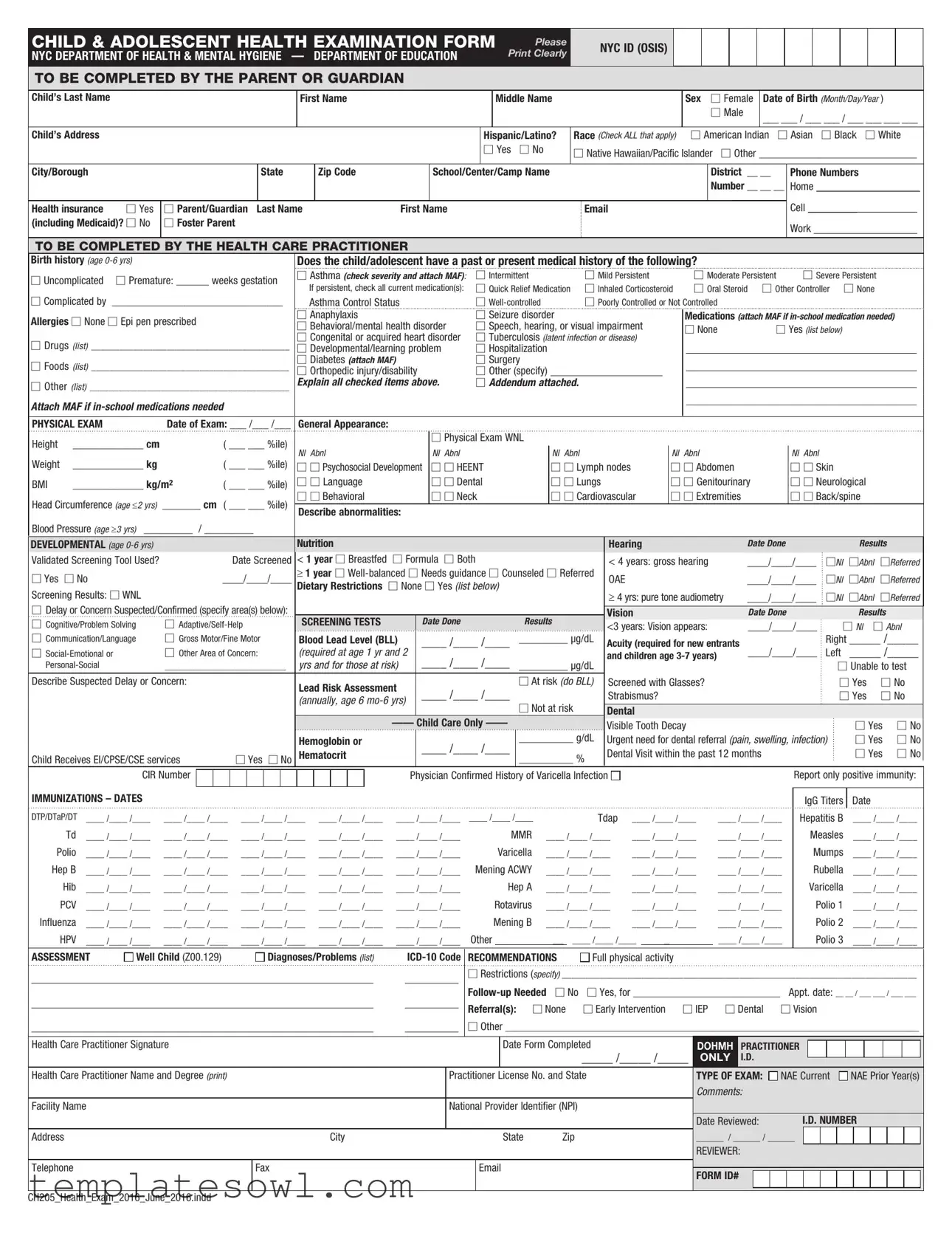
The Child and Adolescent Health Examination Form, developed by the New York City Department of Health and Mental Hygiene in partnership with the Department of Education, is a vital resource that helps parents and guardians provide comprehensive health information about their children. This form collects a variety of details including the child's demographic information such as name, sex, date of birth, and address. It also inquires about the child's health history, focusing on significant areas like birth history, medical conditions, medications, and any allergies. Health care practitioners fill out sections regarding physical examinations, developmental screenings, and immunization records. The form addresses both physical and mental health aspects, assessing everything from growth metrics to potential developmental delays. Additionally, it includes fields for identifying any behavioral, learning, or medical concerns, ensuring a holistic view of the child's health status. By compiling this information, the form aids practitioners in making informed decisions regarding the child’s health and educational needs.
Child Adolescent Health Example
CHILD & ADOLESCENT HEALTH EXAMINATION FORM
NYC DEPARTMENT OF HEALTH & MENTAL HYGIENE — DEPARTMENT OF EDUCATION
Please Print Clearly
NYC ID (OSIS) 
TO BE COMPLETED BY THE PARENT OR GUARDIAN
Child’s Last Name
First Name
Middle Name
Sex ☐ Female
☐Male
Date of Birth (Month/Day/Year )
___ ___ / ___ ___ / ___ ___ ___ ___
Child’s Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hispanic/Latino? |
Race (Check ALL that apply) |
|
☐ American Indian ☐ Asian |
☐ Black |
☐ White |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
☐ Yes |
|
☐ No |
☐ Native Hawaiian/Pacific Islander |
☐ Other _____________________________ |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
City/Borough |
|
|
|
|
|
|
State |
|
|
Zip Code |
|
|
|
School/Center/Camp Name |
|
|
|
|
|
|
|
|
|
District |
__ __ |
Phone Numbers |
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number __ __ __ |
Home ___________________ |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cell |
_________ |
|
|
|
|
|||||||||
Health insurance |
☐ Yes |
☐ Parent/Guardian Last Name |
|
|
|
|
|
First Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
(including Medicaid)? ☐ No |
☐ Foster Parent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Work |
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TO BE COMPLETED BY THE HEALTH CARE PRACTITIONER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
Birth history (age |
|
|
|
|
|
|
|
|
Does the child/adolescent have a past or present medical history of the following? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
☐ Uncomplicated ☐ Premature: ______ weeks gestation |
☐ Asthma (check severity and attach MAF): |
☐ Intermittent |
|
|
|
☐ Mild Persistent |
|
|
|
☐ Moderate Persistent |
|
☐ Severe Persistent |
|
|
|
||||||||||||||||||||||||||||||||||||||
|
If persistent, check all current medication(s): |
☐ Quick Relief Medication |
☐ Inhaled Corticosteroid |
|
☐ Oral Steroid ☐ Other Controller |
☐ None |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
☐ Complicated by |
_________________________________ |
|
Asthma Control Status |
|
|
|
☐ |
|
|
|
☐ Poorly Controlled or Not Controlled |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
Allergies ☐ None ☐ Epi pen prescribed |
|
|
|
|
|
|
|
☐ Anaphylaxis |
|
|
|
|
☐ Seizure disorder |
|
|
|
|
|
|
|
Medications (attach MAF if |
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
☐ Behavioral/mental health disorder |
☐ Speech, hearing, or visual impairment |
|
|
☐ None |
|
☐ Yes (list below) |
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
☐ Congenital or acquired heart disorder |
☐ Tuberculosis |
(latent infection or disease) |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
☐ Drugs (list) __________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
☐ Developmental/learning problem |
☐ Hospitalization |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
☐ Foods (list) __________________________________________ |
☐ Diabetes (attach MAF) |
|
|
|
☐ Surgery |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
☐ Orthopedic injury/disability |
☐ Other (specify) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
☐ Other (list) __________________________________________ |
Explain all checked items above. |
☐ Addendum attached. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
Attach MAF if |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
PHYSICAL EXAM |
|
Date of Exam: ___ /___ /___ |
General Appearance: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Height |
_____________ cm |
|
|
( ___ ___ %ile) |
|
|
|
|
|
|
|
|
|
☐ Physical Exam WNL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
Nl |
Abnl |
|
|
|
Nl Abnl |
|
|
|
|
|
|
Nl Abnl |
|
|
|
|
|
Nl |
Abnl |
|
|
Nl Abnl |
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
Weight |
_____________ kg |
|
|
( ___ ___ %ile) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
☐ ☐ Psychosocial Development |
☐ ☐ HEENT |
|
|
|
☐ ☐ Lymph nodes |
|
|
|
☐ ☐ Abdomen |
|
☐ ☐ Skin |
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
BMI |
_____________ kg/m2 |
|
( ___ ___ %ile) |
☐ ☐ Language |
|
|
|
☐ ☐ Dental |
|
|
|
☐ ☐ Lungs |
|
|
|
☐ ☐ Genitourinary |
☐ ☐ Neurological |
|
|
|
|||||||||||||||||||||||||||||||||
Head Circumference (age ≤2 yrs) |
_______ cm ( ___ ___ %ile) |
☐ ☐ Behavioral |
|
|
|
☐ ☐ Neck |
|
|
|
☐ ☐ Cardiovascular |
|
☐ ☐ Extremities |
|
☐ ☐ Back/spine |
|
|
|
|
|||||||||||||||||||||||||||||||||||
Describe abnormalities: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Blood Pressure (age ≥3 yrs) _________ |
/ _________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
DEVELOPMENTAL (age |
|
|
|
|
|
|
|
|
Nutrition |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hearing |
|
|
|
|
|
|
|
Date Done |
|
|
|
|
|
|
Results |
|
|
||||||||||||
Validated Screening Tool Used? |
|
|
|
Date Screened |
< 1 year ☐ Breastfed |
☐ Formula ☐ Both |
|
|
|
|
|
|
|
< 4 years: gross hearing |
|
____/____/____ |
☐Nl |
|
☐Abnl |
☐Referred |
|||||||||||||||||||||||||||||||||
☐ Yes |
☐ No |
|
|
____/____/____ |
≥ 1 year ☐ |
|
OAE |
|
|
|
|
|
|
|
|
|
____/____/____ |
☐Nl |
|
☐Abnl |
☐Referred |
||||||||||||||||||||||||||||||||
Screening Results: ☐ WNL |
|
|
|
|
|
|
|
|
Dietary Restrictions |
☐ None ☐ Yes (list below) |
|
|
|
|
|
|
|
≥ 4 yrs: pure tone audiometry |
____/____/____ |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
☐Nl |
|
☐Abnl |
☐Referred |
||||||||||||||||||||||
☐ Delay or Concern Suspected/Confirmed (specify area(s) below): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vision |
|
|
|
|
|
|
|
Date Done |
|
|
|
|
|
|
Results |
|
|
||||||||||||||||
☐ Cognitive/Problem Solving |
☐ |
SCREENING TESTS |
|
|
Date Done |
|
|
|
|
Results |
|
|
<3 years: Vision appears: |
|
____/____/____ |
☐ Nl |
☐ Abnl |
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
☐ Communication/Language |
☐ Gross Motor/Fine Motor |
Blood Lead Level (BLL) |
|
____ /____ /____ |
|
_________ µg/dL |
|
Acuity (required for new entrants |
|
|
|
|
|
Right _____ /_____ |
|||||||||||||||||||||||||||||||||||||||
☐ |
☐ Other Area of Concern: |
(required at age 1 yr and 2 |
|
____ /____ /____ |
|
|
|
|
|
|
|
and children age |
|
____/____/____ |
Left |
_____ /_____ |
|||||||||||||||||||||||||||||||||||||
|
__________________________ |
yrs and for those at risk) |
|
|
_________ µg/dL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
☐ Unable to test |
|||||||||||||||||||||||||||||||
Describe Suspected Delay or Concern: |
|
|
|
|
|
|
|
Lead Risk Assessment |
|
____ /____ /____ |
|
☐ At risk (do BLL) |
Screened with Glasses? |
|
|
|
|
|
|
☐ Yes |
☐ No |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Strabismus? |
|
|
|
|
|
|
|
|
|
|
|
|
☐ Yes |
☐ No |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
(annually, age 6 |
|
|
☐ Not at risk |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dental |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
__________ g/dL |
|
Visible Tooth Decay |
|
|
|
|
|
|
|
|
☐ Yes |
☐ No |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Hemoglobin or |
|
|
____ /____ /____ |
|
|
Urgent need for dental referral (pain, swelling, infection) |
|
☐ Yes |
☐ No |
||||||||||||||||||||||||||||||||
Child Receives EI/CPSE/CSE services |
|
|
☐ Yes ☐ No |
Hematocrit |
|
|
|
__________ % |
|
Dental Visit within the past 12 months |
|
|
|
|
|
|
☐ Yes |
☐ No |
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
CIR Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician Confirmed History of Varicella Infection |
|
|
|
|
|
|
|
|
|
|
|
Report only positive immunity: |
|||||||||||||||||||||||
IMMUNIZATIONS – DATES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IgG Titers |
|
Date |
|
|
|
||||||||
DTP/DTaP/DT |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
|
|
|
|
Tdap |
____ /____ /____ |
|
|
____ /____ /____ |
|
Hepatitis B |
____ /____ /____ |
|
||||||||||||||||||||||||||||||||||
|
Td |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
|
|
|
MMR |
____ /____ /____ |
____ /____ /____ |
|
|
____ /____ /____ |
|
|
Measles |
____ /____ /____ |
|
|||||||||||||||||||||||||||||||||
Polio |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
|
|
Varicella |
____ /____ /____ |
____ /____ /____ |
|
|
____ /____ /____ |
|
|
Mumps |
____ /____ /____ |
|
|||||||||||||||||||||||||||||||||||
Hep B |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
Mening ACWY |
____ /____ /____ |
____ /____ /____ |
|
|
____ /____ /____ |
|
|
Rubella |
____ /____ /____ |
|
|||||||||||||||||||||||||||||||||||||
|
Hib |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
|
|
Hep A |
____ /____ /____ |
____ /____ /____ |
|
|
____ /____ /____ |
|
|
Varicella |
____ /____ /____ |
|
||||||||||||||||||||||||||||||||||
|
PCV |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
|
Rotavirus |
____ /____ /____ |
____ /____ /____ |
|
|
____ /____ /____ |
|
|
|
Polio 1 |
____ /____ /____ |
|
||||||||||||||||||||||||||||||||||
Influenza |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
|
Mening B |
____ /____ /____ |
____ /____ /____ |
|
|
____ /____ /____ |
|
|
|
Polio 2 |
____ /____ /____ |
|
|||||||||||||||||||||||||||||||||||
|
HPV |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
Other |
|
|
|
__ |
|
____ /____ /____ |
|
_ |
|
|
|
|
____ /____ /____ |
|
|
|
Polio 3 |
____ /____ /____ |
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
ASSESSMENT |
Well Child (Z00.129) |
|
|
|
Diagnoses/Problems (list) |
RECOMMENDATIONS |
Full physical activity |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
☐Restrictions (specify) ____________________________________________________________________________
☐ Yes, for ___________________________ |
Appt. date: __ __ / ___ ___ / ___ ___ |
|||
Referral(s): ☐ None |
☐ Early Intervention |
☐ IEP |
☐ Dental |
☐ Vision |
☐Other ____________________________________________________________________________
Health Care Practitioner Signature |
|
|
|
Date Form Completed |
DOHMH |
|
PRACTITIONER |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
_____ /_____ /_____ |
ONLY |
|
I.D. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Health Care Practitioner Name and Degree (print) |
|
Practitioner License No. and State |
TYPE OF EXAM: |
|
NAE Current |
|
NAE Prior Year(s) |
||||||||||||||||||
|
|
|
|
|
|
Comments: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Facility Name |
|
National Provider Identifier (NPI) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
Date Reviewed: |
|
|
i.D. NUMBER |
||||||||||||||||
Address |
City |
|
|
State |
Zip |
______ / ______ / ______ |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
reviewer: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone |
Fax |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
FORM ID# |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CH205_Health_Exam_2016_June_2016.indd |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Form Characteristics
| Fact Name | Details |
|---|---|
| Purpose | The Child & Adolescent Health Examination Form is used to assess the health of children and adolescents in New York City. |
| Completion Requirement | This form must be completed by a parent or guardian prior to the child's examination. |
| Data Collected | It collects personal information, medical history, and details about the child's development and vaccinations. |
| Health Insurance Inquiry | The form asks whether the child has health insurance, including Medicaid. |
| Medical History Details | Parents provide information on the child's past or current medical conditions, such as asthma or diabetes. |
| Physical Examination | Healthcare practitioners assess physical health, measuring parameters like height, weight, and blood pressure. |
| Developmental Assessments | Screenings for developmental concerns and various health issues like hearing and vision are included. |
| Immunization Records | The form requests detailed immunization history with specific dates for each vaccine received. |
| Legal Compliance | This form is governed by New York City Department of Health and Mental Hygiene regulations. |
Guidelines on Utilizing Child Adolescent Health
Completing the Child Adolescent Health form is an important step in ensuring that your child's health needs are effectively communicated to healthcare providers. Gathering the necessary information before starting will help make the process smoother and more efficient.
- Locate the form: Obtain the Child Adolescent Health Examination form from your local health department or school district.
- Begin with identification: Fill in your child’s last name, first name, and middle name at the top of the form. Include their date of birth in the format Month/Day/Year.
- Provide personal details: Input your child's address, city, state, zip code, and the name of their school or camp. Note their NYC ID (OSIS) number and the district they belong to.
- Complete contact information: Write down your phone numbers, including home, cell, and work numbers. Enter the parent or guardian's last name, first name, and email address.
- Health background: For children aged 0 to 6 years, go through the birth and medical history section. Indicate any past or present health issues, including asthma, allergies, or any medications currently being taken.
- Physical exam section: Enter the date of the exam and provide details about your child's general appearance, height, weight, and other physical assessment results. This includes checking various body systems indicated on the form.
- Developmental assessments: Fill in results for nutrition and hearing tests, alongside any suspected delays in development. Provide vision screening results if applicable.
- Immunization record: Complete the immunization section by listing dates for vaccinations your child has received, ensuring that all required vaccines are noted.
- Final evaluations: In the assessment section, note any diagnoses or problems related to your child’s health and provide appropriate ICD-10 codes if known.
- Sign and date: Finally, the healthcare practitioner will need to sign and date the form. Ensure that their name, license number, and contact information are accurately filled out.
Once completed, it is essential to submit the form to the appropriate school, camp, or healthcare provider as required. This will ensure that they have all necessary health information to support your child's well-being.
What You Should Know About This Form
What is the purpose of the Child Adolescent Health form?
The Child Adolescent Health form is designed to gather essential health information about children and adolescents. It assists health care practitioners in assessing a child's physical, emotional, and developmental well-being. This form is particularly important in schools, daycares, and other community settings, ensuring that children receive appropriate medical care and support when necessary.
Who is required to complete the form?
The form must be completed by a parent or guardian of the child. In circumstances where the child is in foster care, a foster parent may also fill out the form. It is crucial to provide accurate information to allow for comprehensive health assessments by healthcare professionals.
What information is collected in the form?
Information collected in the form includes the child's personal details, medical history, physical examination findings, developmental screenings, immunization records, and any specific recommendations from healthcare practitioners. This comprehensive data helps identify potential health issues early on and enhances the child's access to appropriate resources.
What is the significance of developmental screenings included in this form?
Developmental screenings are vital for identifying any delays or concerns in a child's growth and development. This part of the form assesses various areas, such as cognitive skills, language development, and social-emotional health. Early identification of developmental issues allows for timely interventions that can significantly improve outcomes for the child.
How does the form address allergies, medications, and health conditions?
The form includes specific sections that inquire about allergies, current medications, and past or present health conditions. This information is crucial for healthcare providers as it helps them to understand the overall health status of the child. Knowing about allergies and medications is particularly important for avoiding any adverse reactions during treatment.
What should be done if there are significant health concerns noted in the form?
If significant health concerns are identified, the healthcare practitioner may recommend follow-up appointments or referrals to specialists. This ensures that the child receives the necessary evaluations and interventions. Parents or guardians are urged to take these recommendations seriously to safeguard the child’s health and well-being.
How frequently should the Child Adolescent Health form be updated?
The Child Adolescent Health form should be updated annually or whenever there is a significant change in the child’s health status. Regular updates help maintain accurate health records, which are vital for ongoing care and support as the child grows.
Common mistakes
Filling out the Child Adolescent Health form correctly is crucial for ensuring that your child's health needs are fully understood and met. However, there are common mistakes that can impact the effectiveness of the form. One major mistake is neglecting to provide complete information about the child's medical history. When this section is not fully filled out, healthcare professionals may overlook vital health concerns that could affect your child's care.
Another frequent error occurs when parents fail to check all relevant boxes regarding allergies and medications. If a child has an allergy to peanuts but the box is left unchecked, it can lead to severe reactions during school or camp activities. Additionally, listing medications without their specific dosages can create confusion. Always be precise and thorough in these sections.
Some parents also struggle with clarity in their handwriting. If sections of the form are difficult to read, it can lead to misunderstandings. Use block letters and be consistent in how names and addresses are written. This small step can make a significant difference in the legibility of the information.
Moreover, submitting the form without proper contact information is a considerable mistake. Whether it's a home phone number, cell phone, or email, make sure all communication lines are open. In case of emergencies or follow-ups, having correct contact information ensures timely interventions.
Additionally, people often overlook the importance of updating immunization records. Failing to provide the most recent vaccination dates can hinder a child’s school health compliance. Review your child’s immunizations before submitting the form, and include all necessary documentation where indicated.
Another misconception is that simple forms do not require a parent's signature. Many people neglect to sign the form, thinking it is unnecessary. However, a signature verifies that the information provided is accurate and authorized by a responsible adult, which is essential for legal and procedural purposes.
In some cases, parents may not attach additional documents when required. For instance, if your child is on medication during school hours, attaching a Medication Administration Form (MAF) is vital. Without it, the school may not be able to administer necessary medications, causing distress for the child.
Finally, not reviewing the entire completed form before submission can lead to errors being overlooked. A final check can catch mistakes such as incorrect birth dates or missing information that could affect your child's health assessment. Taking the time for a thorough review ensures that everything is in order, minimizing complications later.
Documents used along the form
The Child Adolescent Health Form is an important document used to assess the health and development of children and adolescents. It is often accompanied by various other forms and documents that provide additional important health information. Below is a list of related documents that are frequently utilized alongside the Child Adolescent Health Form.
- Immunization Record: This document lists all vaccinations a child has received. It's crucial for ensuring that children are protected against preventable diseases.
- Medication Administration Form (MAF): This form is used when a child requires medication during school hours. It ensures that medications are given safely and properly.
- Vision Screening Form: This form records the results of vision tests. It detects potential vision issues early on and helps plan further evaluations if needed.
- Hearing Screening Form: Similar to the vision form, this document records hearing test results. It is essential for identifying any hearing impairments early.
- Behavioral Health Assessment Form: This assesses a child's mental health and emotional well-being. Early detection of issues can lead to timely interventions.
- Nutritional Assessment Form: This form evaluates a child's dietary habits and nutritional needs, which is vital for ensuring healthy growth and development.
- Emergency Contact Form: This document provides information on whom to contact in case of an emergency. It is essential for safety at school or daycare.
- Developmental Milestones Checklist: This tool tracks a child’s development across various domains. It ensures that they meet critical growth benchmarks.
- Referral Form: If a child requires further evaluation or services from specialists, this form is used to facilitate a referral to the appropriate healthcare provider.
Each of these forms plays a vital role in developing a comprehensive understanding of a child’s health. Proper completion and communication of this information help ensure children receive the best possible care and support.
Similar forms
-
School Health Form: Like the Child Adolescent Health form, the School Health Form collects essential health information about students. It includes records of immunizations, allergies, and any medical conditions that could affect school performance or require special considerations during school activities.
-
Wellness Check Form: This document is similar as it assesses the overall health of children during routine checkups. Both forms focus on capturing medical history and ensuring that children meet developmental milestones, providing a comprehensive overview of a child's health status.
-
Immunization Record: The Immunization Record details vaccine history, just like the immunization section in the Child Adolescent Health form. Both documents ensure that a child's vaccinations are up-to-date and track any required vaccinations for school entry or participation in activities.
-
Physical Examination Report: This report contains findings from a physical exam, similar to the sections dedicated to general appearance and physical health in the Child Adolescent Health form. It ensures that practitioners record important health indicators like weight, height, and blood pressure.
-
Special Education Evaluation Form: This form, used for children needing special education services, parallels the Child Adolescent Health form by capturing developmental assessments and any medical conditions. Both are crucial for determining appropriate support and accommodations in educational settings.
Dos and Don'ts
When completing the Child Adolescent Health form, there are several important practices to follow and avoid to ensure accuracy and clarity.
- Do: Print information clearly, using block letters to enhance legibility.
- Do: Ensure all required fields are completed thoroughly to avoid delays in processing.
- Do: Review the information for accuracy before submitting the form.
- Do: Attach any necessary documents, such as medical history or medication authorization forms.
- Don't: Leave any mandatory sections blank, as this may lead to the rejection of the form.
- Don't: Use abbreviations or shorthand, as it may cause confusion for the healthcare practitioner reviewing the form.
- Don't: Provide incorrect or outdated information regarding the child's health or vaccination history.
- Don't: Forget to sign and date the form, which is essential for validation.
Misconceptions
- Misconception 1: The Child Adolescent Health form is only necessary for children with known health issues.
- Misconception 2: Parents and guardians need to fill out the entire form themselves.
- Misconception 3: The information collected on the form is not confidential.
- Misconception 4: Completing the form takes a long time and is overly complicated.
- Misconception 5: You cannot make changes to the form once it has been submitted.
- Misconception 6: Medical consent is not required from parents or guardians.
- Misconception 7: The Child Adolescent Health form is only relevant for school-related activities.
- Misconception 8: Parents can choose not to disclose certain health information.
- Misconception 9: There is no need for follow-up after submitting the form.
This is incorrect. The form is designed for all children and adolescents, regardless of their health status, to ensure that they receive comprehensive health assessments.
While parents or guardians must provide most of the information, a healthcare practitioner will complete the necessary sections regarding medical history and examinations.
In fact, all personal health information is protected. The form follows strict confidentiality guidelines to safeguard children’s health information.
The form is structured for clarity and is meant to be user-friendly. While some sections require detailed responses, most can be completed quickly.
Changes can be made if new health information arises. Parents or guardians should communicate any updates to the school or healthcare provider.
Consent is indeed necessary. The form includes sections that require parental consent for healthcare providers to proceed with assessments or treatments.
This form serves broader purposes, promoting overall health monitoring and supporting access to necessary healthcare services beyond just school activities.
While parents have the right to decide which details to share, providing complete health history is crucial for proper assessment and care.
Follow-ups are often recommended based on the health assessments and any identified concerns. Parents and guardians should pay attention to any suggested appointments or referrals.
Key takeaways
Filling out the Child Adolescent Health form can be straightforward, but it's essential to approach it with care. Here are some key takeaways to consider:
- Print Clearly: Use clear and legible handwriting when completing the form to avoid any misunderstandings.
- Provide Accurate Information: Double-check all entries, especially names, dates, and contact details.
- Medical History Matters: Be honest about your child's medical history, including any past illnesses, surgeries, and existing conditions.
- Complete All Sections: Ensure every section is filled out. Incomplete forms may delay processing.
- Use Medical Abbreviations Wisely: If you must use abbreviations, make sure they are widely recognized to prevent confusion.
- Attach Required Documents: If medications or special health considerations are indicated, attach any necessary medical authorization forms.
- Review Immunization Records: Make sure that all immunization dates are accurate and up to date.
- Focus on Developmental Milestones: Provide detailed information about your child’s developmental history and any concerns you may have noticed.
- Sign the Form: Don't forget to sign and date the form to confirm that all information is correct.
- Ask for Help if Needed: If you have any questions or uncertainties about filling out the form, feel free to ask for assistance from health professionals.
Utilizing this form effectively will help ensure your child's health needs are addressed. It serves as a critical tool in enhancing their overall well-being.
Browse Other Templates
What Is a Disclosure Statement - The form’s format allows for easy check-box responses to streamline the disclosure process.
Resale Certificate Massachusetts - This certificate must be presented each time tax-exempt items are purchased for resale.
Ozempic Insurance Approval - Member information includes name, identification number, and date of birth.