Fill Out Your Cms 2728 U3 Form
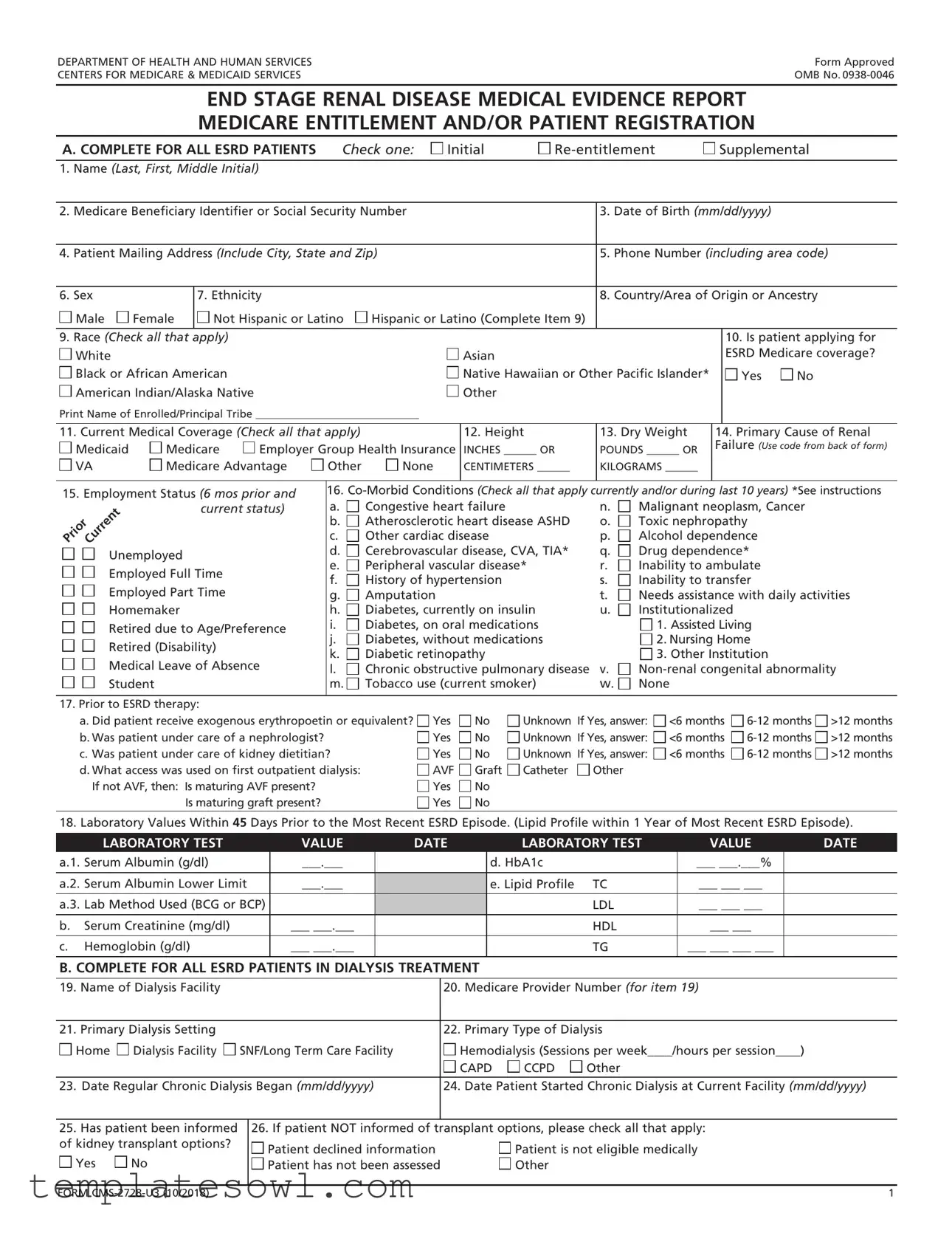
The CMS 2728 U3 Form plays a crucial role in the healthcare system, particularly for individuals diagnosed with End Stage Renal Disease (ESRD) who are seeking Medicare coverage. This form serves multiple purposes, including initial applications for Medicare entitlement, re-entitlement for beneficiaries who have previously lost coverage, and supplemental requests for those who recently underwent a kidney transplant or underwent self-care dialysis training. The form collects essential information about patients, including their demographics, medical history, and current healthcare status. Notably, it requires details such as the patient's name, date of birth, Medicare Beneficiary Identifier, and the primary cause of renal failure, which is determined using ICD-10 codes. The attending physician—or another qualified healthcare professional—must certify the information to confirm that the patient requires regular dialysis or a kidney transplant, emphasizing the form's significance in determining eligibility for Medicare benefits. By thoroughly documenting this information, the CMS 2728 U3 Form ensures that patients receive the necessary financial support and medical care they require to manage their condition effectively.
Cms 2728 U3 Example
DEPARTMENT OF HEALTH AND HUMAN SERVICES |
Form Approved |
CENTERS FOR MEDICARE & MEDICAID SERVICES |
OMB No. |
END STAGE RENAL DISEASE MEDICAL EVIDENCE REPORT
MEDICARE ENTITLEMENT AND/OR PATIENT REGISTRATION
A. COMPLETE FOR ALL ESRD PATIENTS Check one: |
Initial |
Supplemental |
1.Name (Last, First, Middle Initial)
2. Medicare Beneficiary Identifier or Social Security Number |
|
3. Date of Birth (mm/dd/yyyy) |
|
||||||||
|
|
|
|
|
|
|
|||||
4. Patient Mailing Address (Include City, State and Zip) |
|
5. Phone Number (including area code) |
|||||||||
|
|
|
|
|
|
|
|
|
|||
6. Sex |
|
7. Ethnicity |
|
|
|
8. Country/Area of Origin or Ancestry |
|||||
Male |
Female |
Not Hispanic or Latino |
Hispanic or Latino (Complete Item 9) |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
||
9. Race (Check all that apply) |
|
|
|
|
|
|
|
10. Is patient applying for |
|||
White |
|
|
|
|
|
Asian |
|
|
|
ESRD Medicare coverage? |
|
Black or African American |
|
|
|
Native Hawaiian or Other Pacific Islander* |
|
Yes |
No |
||||
American Indian/Alaska Native |
|
|
|
Other |
|
|
|
|
|
||
Print Name of Enrolled/Principal Tribe ______________________________ |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|||||
11. Current Medical Coverage (Check all that apply) |
|
12. Height |
13. Dry Weight |
14. Primary Cause of Renal |
|||||||
Medicaid |
Medicare |
Employer Group Health Insurance |
INCHES ______ OR |
POUNDS ______ OR |
Failure (Use code from back of form) |
||||||
|
|
|
|||||||||
VA |
Medicare Advantage |
Other |
None |
CENTIMETERS ______ |
KILOGRAMS ______ |
|
|
|
|||
|
|
|
|
|
|
||||||
15. Employment Status (6 mos prior and |
16. |
||||||||||
Prior Current |
|
current status) |
a. |
Congestive heart failure |
n. |
Malignant neoplasm, Cancer |
|||||
|
|
|
b. |
Atherosclerotic heart disease ASHD |
o. |
Toxic nephropathy |
|
||||
|
|
|
|
|
|||||||
|
|
|
|
c. |
Other cardiac disease |
p. |
Alcohol dependence |
|
|||
Unemployed |
|
|
d. |
Cerebrovascular disease, CVA, TIA* |
q. |
Drug dependence* |
|
||||
|
|
e. |
Peripheral vascular disease* |
r. |
Inability to ambulate |
|
|||||
Employed Full Time |
|
|
|||||||||
|
f. |
History of hypertension |
s. |
Inability to transfer |
|
||||||
Employed Part Time |
|
|
|||||||||
|
g. |
Amputation |
|
t. |
Needs assistance with daily activities |
||||||
Homemaker |
|
|
h. |
Diabetes, currently on insulin |
u. |
Institutionalized |
|
||||
Retired due to Age/Preference |
i. |
Diabetes, on oral medications |
|
1. Assisted Living |
|
||||||
j. |
Diabetes, without medications |
|
2. Nursing Home |
|
|||||||
Retired (Disability) |
|
|
|
||||||||
|
k. |
Diabetic retinopathy |
|
3. Other Institution |
|
||||||
Medical Leave of Absence |
|
|
|||||||||
l. |
Chronic obstructive pulmonary disease |
v. |
|||||||||
Student |
|
|
m. |
Tobacco use (current smoker) |
w. |
None |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
17. Prior to ESRD therapy: |
|
|
|
|
|
|
|
a. Did patient receive exogenous erythropoetin or equivalent? |
Yes |
No |
Unknown If Yes, answer: |
<6 months |
>12 months |
||
b. Was patient under care of a nephrologist? |
Yes |
No |
Unknown If Yes, answer: |
<6 months |
>12 months |
||
c. Was patient under care of kidney dietitian? |
Yes |
No |
Unknown If Yes, answer: |
<6 months |
>12 months |
||
d. What access was used on first outpatient dialysis: |
AVF |
Graft |
Catheter |
Other |
|
|
|
If not AVF, then: Is maturing AVF present? |
Yes |
No |
|
|
|
|
|
Is maturing graft present? |
Yes |
No |
|
|
|
|
|
18. Laboratory Values Within 45 Days Prior to the Most Recent ESRD Episode. (Lipid Profile within 1 Year of Most Recent ESRD Episode).
|
LABORATORY TEST |
VALUE |
DATE |
LABORATORY TEST |
VALUE |
DATE |
a.1. Serum Albumin (g/dl) |
___.___ |
|
d. HbA1c |
___ ___.___% |
|
|
|
|
|
|
|
|
|
a.2. Serum Albumin Lower Limit |
___.___ |
|
e. Lipid Profile TC |
___ ___ ___ |
|
|
|
|
|
|
|
|
|
a.3. Lab Method Used (BCG or BCP) |
|
|
LDL |
___ ___ ___ |
|
|
|
|
|
|
|
|
|
b. |
Serum Creatinine (mg/dl) |
___ ___.___ |
|
HDL |
___ ___ |
|
|
|
|
|
|
|
|
c. |
Hemoglobin (g/dl) |
___ ___.___ |
|
TG |
___ ___ ___ ___ |
|
|
|
|
|
|
|
|
B. COMPLETE FOR ALL ESRD PATIENTS IN DIALYSIS TREATMENT
19. |
Name of Dialysis Facility |
|
20. |
Medicare Provider Number (for item 19) |
|||
|
|
|
|
|
|||
21. |
Primary Dialysis Setting |
|
22. |
Primary Type of Dialysis |
|||
Home |
Dialysis Facility |
SNF/Long Term Care Facility |
Hemodialysis (Sessions per week____/hours per session____) |
||||
|
|
|
|
CAPD |
CCPD |
Other |
|
23. |
Date Regular Chronic Dialysis Began (mm/dd/yyyy) |
24. |
Date |
Patient Started Chronic Dialysis at Current Facility (mm/dd/yyyy) |
|||
|
|
|
|
|
|
|
|
25.Has patient been informed of kidney transplant options?
Yes |
No |
26. If patient NOT informed of transplant options, please check all that apply:
Patient declined information |
Patient is not eligible medically |
Patient has not been assessed |
Other |
FORM |
1 |
C.COMPLETE FOR ALL KIDNEY TRANSPLANT PATIENTS
27. Date of Transplant (mm/dd/yyyy)
28. Name of Transplant Hospital
29. Medicare Provider Number for Item 28
Date patient was admitted as an inpatient to a hospital in preparation for, or anticipation of, a kidney transplant prior to the date of actual transplantation.
30.Enter Date (mm/dd/yyyy)
31. Name of Preparation Hospital
32.Medicare Provider number for Item 31
33.Current Status of Transplant (if functioning, skip items 36 and 37)
Functioning |
34. Type of Donor:
Deceased |
Living Related |
Living Unrelated |
35. If
36. Current Dialysis Treatment Site
Home |
Dialysis Facility |
SNF/Long Term Care Facility |
D. COMPLETE FOR ALL ESRD
37. |
Name of Training Provider |
38. |
Medicare Provider Number of Training Provider (for Item 37) |
|||
|
|
|
|
|
||
39. |
Date Training Began (mm/dd/yyyy) |
40. |
Type of Training |
|
||
|
|
|
Hemodialysis |
a. |
Home b. In Center |
|
|
|
|
CAPD |
CCPD |
Other |
|
|
|
|
||||
41. |
This Patient is Expected to Complete (or has completed) Training |
42. Date When Patient Completed, or is Expected to Complete, Training |
||||
and will |
(mm/dd/yyyy) |
|
|
|||
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
I certify that the above
43. Printed Name and Signature of Physician personally familiar with the patient’s training
a.) Printed Name |
b.) Signature |
c.) Date (mm/dd/yyyy) |
|
|
|
44. UPIN or NPI of Physician in Item 43
E. PHYSICIAN IDENTIFICATION
45. Attending Physician (Print)
46. Physician’s Phone No. (include Area Code)
47. UPIN or NPI of Physician in Item 45
PHYSICIAN ATTESTATION
I certify, under penalty of perjury, that the information on this form is correct to the best of my knowledge and belief. Based on diagnostic tests and laboratory findings, I further certify that this patient has reached the stage of renal impairment that appears irreversible and permanent and requires a regular course of dialysis or kidney transplant to maintain life. I understand that this information is intended for use in establishing the patient’s entitlement to Medicare benefits and that any falsification, misrepresentation, or concealment of essential information may subject me to fine, imprisonment, civil penalty, or other civil sanctions under applicable Federal laws.
48. Attending Physician’s Signature of Attestation (Same as Item 45)
49.Date (mm/dd/yyyy)
50. Physician Recertification Signature
51.Date (mm/dd/yyyy)
52. Remarks
F. OBTAIN SIGNATURE FROM PATIENT
I hereby authorize any physician, hospital, agency, or other organization to disclose any medical records or other information about my medical condition to the Department of Health and Human Services for purposes of reviewing my application for Medicare entitlement under the Social Security Act and/or for scientific research.
53.Signature of Patient (Signature by mark must be witnessed.)
54.Date (mm/dd/yyyy)
G. PRIVACY STATEMENT
The collection of this information is authorized by Section 226A of the Social Security Act. The information provided will be used to determine if an individual is entitled to Medicare under the End Stage Renal Disease provisions of the law. The information will be maintained in system No.
or maintenance of health. Additional disclosures may be found in the Federal Register notice cited above. You should be aware that
FORM |
2 |

LIST OF PRIMARY CAUSES OF RENAL DISEASE
Item 14. Primary Cause of Renal Failure should be completed by the attending physician from the list below. Enter the
DESCRIPTION |
DIABETES
E10.22 Type 1 diabetes mellitus with diabetic chronic kidney disease
E10.29 Type 1 diabetes mellitus with other diabetic kidney complication
E11.22 Type 2 diabetes mellitus with diabetic chronic kidney disease
E11.29 Type 2 diabetes mellitus with other diabetic kidney complication
GLOMERULONEPHRITIS
N00.8 Acute nephritic syndrome with other morphologic changes
N01.9 Rapidly progressive nephritic syndrome with unspecified morphologic changes
N02.8 Recurrent and persistent hematuria with other morphologic changes
N03.0 Chronic nephritic syndrome with minor glomerular abnormality
N03.1 Chronic nephritic syndrome with focal and segmental glomerular lesions
N03.2 Chronic nephritic syndrome with diffuse membranous glomerulonephritis
N03.3 Chronic nephritic syndrome with diffuse mesangial proliferative glomerulonephritis
N03.4 Chronic nephritic syndrome with diffuse endocapillary proliferative glomerulonephritis
N03.5 Chronic nephritic syndrome with diffuse mesangiocapillary glomerulonephritis
N03.6 Chronic nephritic syndrome with dense deposit disease
N03.7 Chronic nephritic syndrome with diffuse crescentic glomerulonephritis
N03.8 Chronic nephritic syndrome with other morphologic changes
N03.9 Chronic nephritic syndrome with unspecified morphologic changes
N04.0 Nephrotic syndrome with minor glomerular abnormality
N04.1 Nephrotic syndrome with focal and segmental glomerular lesions
N04.2 Nephrotic syndrome with diffuse membranous glomerulonephritis
N04.3 Nephrotic syndrome with diffuse mesangial proliferative glomerulonephritis
N04.4 Nephrotic syndrome with diffuse endocapillary proliferative glomerulonephritis
N04.5 Nephrotic syndrome with diffuse mesangiocapillary glomerulonephritis
N04.6 Nephrotic syndrome with dense deposit disease
N04.7 Nephrotic syndrome with diffuse crescentic glomerulonephritis
N04.8 Nephrotic syndrome with other morphologic changes
N04.9 Nephrotic syndrome with unspecified morphologic changes
N05.9 Unspecified nephritic syndrome with unspecified morphologic changes
N07.0 Hereditary nephropathy, not elsewhere classified with minor glomerular abnormality
SECONDARY GLOMERULONEPHRITIS/VASCULITIS
D59.3
D69.0 Allergic purpura
I77.89 Other specified disorders of arteries and arterioles
M31.0 Hypersensitivity angiitis
M31.1 Thrombotic microangiopathy
M31.31 Wegener’s granulomatosis with renal involvement
M31.7 Microscopic polyangiitis
M32.0
M32.10 Systemic lupus erythematosus, organ or system involvement unspecified
M32.14 Glomerular disease in systemic lupus erythematosus
M32.15
M34.89 Other systemic sclerosis
INTERSTITIAL NEPHRITIS/PYELONEPHRITIS
N10 Acute
N11.9 Chronic
N13.70
N13.8 Other obstructive and reflux uropathy 2
TRANSPLANT COMPLICATIONS
T86.00 Unspecified complication of bone marrow transplant
T86.10 Unspecified complication of kidney transplant
T86.20 Unspecified complication of heart transplant
T86.40 Unspecified complication of liver transplant
T86.819 Unspecified complication of lung transplant
T86.859 Unspecified complication of intestine transplant
T86.899 Unspecified complication of other transplanted tissue
FORM |
3 |

LIST OF PRIMARY CAUSES OF RENAL DISEASE
Item 14. Primary Cause of Renal Failure should be completed by the attending physician from the list below. Enter the
DESCRIPTION |
HYPERTENSION/LARGE VESSEL DISEASE
I12.9 Hypertensive chronic kidney disease with stage 1through stage 4 chronic kidney disease, or unspecified chronic kidney disease
I15.0 Renovascular hypertension
I15.8 Other secondary hypertension
I75.81 Atheroembolism of kidney
CYSTIC/HEREDITARY/CONGENITAL/OTHER DISEASES
E72.04 |
Cystinosis |
E72.53 |
Hyperoxaluria |
E75.21 |
Fabry |
N07.8 |
Hereditary nephropathy, not elsewhere classified |
|
with other morphologic lesions |
N31.9 |
Neuromuscular dysfunction of bladder, |
|
unspecified |
Q56.0 |
Hermaphroditism, not elsewhere classified |
Q60.2 |
Renal agenesis, unspecified |
Q61.19 |
Other polycystic kidney, infantile type |
Q61.2 |
Polycystic kidney, adult type |
Q61.4 |
Renal dysplasia |
Q61.5 |
Medullary cystic kidney |
Q61.8 |
Other cystic kidney diseases |
Q62.11 |
Congenital occlusion of ureteropelvic junction |
Q62.12 |
Congenital occlusion of ureterovesical orifice |
Q63.8 |
Other specified congenital malformations of |
|
kidney |
Q64.2 |
Congenital posterior urethral valves |
Q79.4 |
Prune belly syndrome |
Q85.1 |
Tuberous sclerosis |
Q86.8 |
Other congenital malformation syndromes due |
|
to known exogenous causes |
Q87.1 |
Congenital malformation syndromes |
|
predominantly associated with short stature |
Q87.81 |
Alport syndrome |
NEOPLASMS/TUMORS
C64.9 Malignant neoplasm of unspecified kidney, except renal pelvis
C80.1 Malignant (primary) neoplasm, unspecified
C85.93
C88.2 Heavy chain disease
C90.00 Multiple myeloma not having achieved remission
D30.9 Benign neoplasm of urinary organ, unspecified
D41.00 Neoplasm of uncertain behavior of unspecified kidney
D41.9 Neoplasm of uncertain behavior of unspecified urinary organ
E85.9 Amyloidosis, unspecified
N05.8 Unspecified nephritic syndrome with other morphologic changes
DISORDERS OF MINERAL METABOLISM
E83.52 Hypercalcemia
GENITOURINARY SYSTEM
A18.10 Tuberculosis of genitourinary system, unspecified
N28.9 Disorder of kidney and ureter, unspecified
ACUTE KIDNEY FAILURE
N17.0 Acute kidney failure with tubular necrosis
N17.1 Acute kidney failure with acute cortical necrosis
N17.9 Acute kidney failure, unspecified
MISCELLANEOUS CONDITIONS
B20 Human immunodeficiency virus [HIV] disease
D57.1
D57.3 Sickle cell trait
I50.9 Heart failure, unspecified
K76.7 Hepatorenal syndrome
M10.30 Gout due to renal impairment, unspecified site
N14.0 Analgesic nephropathy
N14.1 Nephropathy induced by other drugs, medicaments and biological substances
N14.3 Nephropathy induced by heavy metals
N20.0 Calculus of kidney
N25.89 Other disorders resulting from impaired renal tubular function
N26.9 Renal sclerosis, unspecified
N28.0 Ischemia and infarction of kidney
N28.89 Other specified disorders of kidney and ureter
O90.4 Postpartum acute kidney failure
S37.009A Unspecified injury of unspecified kidney, initial encounter
Z90.5 Acquired Absence of Kidney
FORM |
4 |
INSTRUCTIONS FOR COMPLETION OF END STAGE RENAL DISEASE MEDICAL EVIDENCE REPORT
MEDICARE ENTITLEMENT AND/OR PATIENT REGISTRATION
For whom should this form be completed:
This form SHOULD NOT be completed for those patients who are in acute renal failure. Acute renal failure is a condition in which kidney function can be expected to recover after a short period of dialysis, i.e., several weeks or months.
This form MUST BE completed within 45 days for ALL patients beginning any of the following:
Check the appropriate block that identifies the reason for submission of this form.
Initial
For all patients who initially receive a kidney transplant instead of a course of dialysis.
For patients for whom a regular course of dialysis has been prescribed by a physician because they have reached that stage of renal impairment that a kidney transplant or regular course of dialysis is necessary to maintain life. The first date of a regular course of dialysis is the date this prescription
is implemented whether as an inpatient of a hospital, an outpatient in a dialysis
center or facility, or a home patient. The form should be completed for all patients in this category even if the patient dies within this time period.
For beneficiaries who have already been entitled to ESRD Medicare benefits and those benefits were terminated because their coverage stopped 3 years post transplant but now are again applying for Medicare ESRD benefits because they returned to dialysis or received another kidney transplant.
For beneficiaries who stopped dialysis for more than 12 months, have had their Medicare ESRD benefits terminated and now returned to dialysis or received a kidney transplant. These patients will be reapplying for Medicare ESRD benefits.
Supplemental
Patient has received a transplant or trained for
All items except as follows: To be completed by the attending physician, head nurse, or social worker involved in this patient’s treatment of renal disease.
Items 14,
Item 43: To be signed by the attending physician or the physician familiar with the patient’s
Items 53 and 54: To be signed and dated by the patient.
1.Enter the patient’s legal name (Last, first, middle initial). Name should appear exactly the same as it appears on patient’s social security or Medicare card.
2.If the patient is covered by Medicare, enter his/her Medicare Beneficiary Identifier as it appears on his/her Medicare card. If the patient has not yet been assigned a Medicare Beneficiary Identifier, enter the Social Security Number as it appears on his/her Social Security Card. Only enter the Social Security
Number if the patient does not have a Medicare Beneficiary Identifier.
3.Enter patient’s date of birth
4.Enter the patient’s mailing address (number and street or post office box number, city, state, and ZIP code.)
5.Enter the patient’s home area code and telephone number.
6.Check the appropriate block to identify sex.
7.Check the appropriate block to identify ethnicity. Definitions of the ethnicity categories for Federal statistics are as follows:
Not Hispanic or
Hispanic or
8.Country/Area of origin or
9.Check the appropriate block(s) to identify race. The 1997 OMB standards permit the reporting of more than one race. An individual’s response to the race question is based upon self- identification.
Definitions of the racial categories for Federal statistics are as follows:
Black or African
American Indian/Alaska
Native Hawaiian or Other Pacific
Other
10.Check the appropriate yes or no block to indicate if patient is applying for ESRD Medicare. Note: Even though a person may already be entitled to general Medicare coverage, he/she should reapply for ESRD Medicare coverage.
DISTRIBUTION OF COPIES:
•To the Applicant: Forward the hard copy of this form with original signatures to the Social Security office servicing the claim.
•To the Dialysis Facility: Complete the form in Crown Web or maintain a copy with signature’s in the patient file.
FORM |
5 |
11.Check all the blocks that apply to this patient’s current medical insurance status.
Employer Group Health
Medicare
Other Medical
12.Enter the patient’s most recent recorded height in inches OR centimeters at time form is being completed. If entering height in centimeters, round to the nearest centimeter. Estimate or use last known height for those unable to be measured. (Example of inches - 62. DO NOT PUT 5’2”) NOTE: For amputee patients, enter height prior to amputation.
13.Enter the patient’s most recent recorded dry weight in pounds OR kilograms at time form is being completed. If entering weight in kilograms, round to the nearest kilogram.
NOTE: For amputee patients, enter actual dry weight.
14.Primary Cause of Renal Failure should be determined by the attending physician using the appropriate
15.Check the first box to indicate employment status 6 months prior to renal failure and the second box to indicate current employment status. Check only one box for each time period. If patient is under 6 years of age, leave blank.
16.To be completed by the attending physician. Check all
*Cerebrovascular Disease includes history of stroke/ cerebrovascular accident (CVA) and transient ischemic attack (TIA).
*Peripheral Vascular Disease includes absent foot pulses, prior typical claudication, amputations for vascular disease, gangrene and aortic aneurysm.
*Drug dependence means dependent on illicit drugs.
17.Prior to ESRD therapy, check the appropriate box to indicate whether the patient received Exogenous erythropoetin (EPO) or equivalent, was under the care of a nephrologist and/or was under the care of a kidney dietitian. Provide vascular access information as to the type of access used
NOTE: For those patients
18a1. Enter the serum albumin value (g/dl) and date test was taken.
This value and date must be within 45 days prior to first dialysis treatment or kidney transplant.
18a2. Enter the lower limit of the normal range for serum albumin from the laboratory which performed the serum albumin test entered in 19a1.
18a3. Enter the serum albumin lab method used (BCG or BCP).
18b. Enter the serum creatinine value (mg/dl) and date test was taken. THIS FIELD MUST BE COMPLETED. Value must be within 45 days prior to first dialysis treatment or kidney transplant.
18c. Enter the hemoglobin value (g/dl) and date test was taken. This value and date must be within 45 days prior to the first dialysis treatment or kidney transplant.
18d. Enter the HbA1c value and the date the test was taken. The date must be within 1 year prior to the first dialysis treatment or kidney transplant.
18e. Enter the Lipid Profile values and date test was taken. These values:
19.Enter the name of the dialysis facility where patient is currently receiving care and who is completing this form for patient.
20.Enter the
21.If the person is receiving a regular course of dialysis treatment, check the appropriate anticipated
22.If the patient is, or was, on regular dialysis, check the anticipated
the hours that were prescribed for each session), CAPD (Continuous Ambulatory Peritoneal Dialysis) and CCPD (Continuous Cycling Peritoneal Dialysis), or Other. Check only one block. NOTE: Other has been placed on this form to be used only to report IPD (Intermittent Peritoneal Dialysis) and any new method of dialysis that may be developed prior to the renewal of this form by Office of Management
and Budget.
23.Enter the date (month, day, year) that a “regular course of chronic dialysis” began. The beginning of the course of dialysis is counted from the beginning of regularly scheduled dialysis necessary for the treatment of end stage renal disease (ESRD) regardless of the dialysis setting. The date of the first dialysis treatment after the physician has determined that this patient has ESRD and has written a prescription for a “regular course of dialysis” is the “Date Regular Chronic Dialysis Began” regardless of whether this prescription was implemented in a hospital/ inpatient, outpatient, or home setting and regardless of any acute treatments received prior to the implementation of the prescription.
NOTE: For these purposes, end stage renal disease means irreversible damage to a person’s kidneys so severely affecting his/her ability to remove or adjust blood wastes that in order to maintain life he or she must have either a course of dialysis or a kidney transplant to maintain life.
If
24.Enter date patient started chronic dialysis at current facility of dialysis services. In cases where patient transferred to current dialysis facility, this date will be after the date in Item 24.
25.Enter whether the patient has been informed of their options for receiving a kidney transplant.
26.If the patient has not been informed of their options (answered “no” to Item 25), then enter all reasons why a kidney transplant was not an option for this patient at this time.
FORM |
6 |

27.Enter the date(s) of the patient’s kidney transplant(s). If reentering the Medicare program, enter current transplant date.
28.Enter the name of the hospital where the patient received a kidney transplant on the date in Item 27.
29.Enter the
30.Enter date patient was admitted as an inpatient to a hospital in preparation for, or anticipation of, a kidney transplant prior to the date of the actual transplantation. This includes hospitalization for transplant workup in order to place the patient on a transplant waiting list.
31.Enter the name of the hospital where patient was admitted as an inpatient in preparation for, or anticipation of, a kidney transplant prior to the date of the actual transplantation.
32.Enter the
33.Check the appropriate functioning or
34.Enter the type of kidney transplant organ donor, Deceased, Living Related or Living Unrelated, that was provided to the patient.
35.If transplant is nonfunctioning, enter date patient returned to a regular course of dialysis. If patient did not stop dialysis post transplant, enter transplant date.
36.If applicable, check where patient is receiving dialysis treatment following transplant rejection. A nursing home or skilled nursing facility is considered as home setting.
37.Enter the name of the provider furnishing
38.Enter the
39.Enter the date
40.Check the appropriate block which describes the type of self- care dialysis training the patient began. If the patient trained for hemodialysis, enter whether the training was to perform dialysis in the home setting or in the facility (in center). If the patient trained for IPD (Intermittent Peritoneal Dialysis), report as Other.
41.Check the appropriate block as to whether or not the physician certifies that the patient is expected to complete the training successfully and
42.Enter date patient completed or is expected to complete self- dialysis training.
43.Enter printed name and signature of the attending physician or the physician familiar with the patient’s
44.Enter the National Provider Identifier (NPI) or the Unique Physician Identification Number (UPIN) of physician in Item 43. (See Item 47 for explanation of UPIN.)
45.Enter the name of the physician who is supervising the patient’s renal treatment at the time this form is completed.
46.Enter the area code and telephone number of the physician who is supervising the patient’s renal treatment at the time this form is completed.
47.Enter the National Provider Identifier (NPI) or the Unique Physician Identification Number (UPIN) of physician in Item 45
A system of physician identifiers is mandated by Section 9202 of the Consolidated Omnibus Budget Reconciliation Act of 1985. It requires a unique identifier for each physician who provides services for which Medicare payment is made. An identifier is assigned to each physician regardless of his or her practice configuration. The UPIN is established in a national Registry of Medicare Physician Identification and Eligibility Records (MPIER). Transamerica Occidental Life Insurance Company is the Registry Carrier that establishes and maintains the national registry of physicians receiving Part B Medicare payment. Its address is: UPIN Registry, Transamerica Occidental Life, P.O. Box 2575, Los Angeles, CA
The NPI is established by the NPI Enumerator located in Fargo, North Dakota. The NPI Enumerator may be contacted by:
Phone:
Email: customerservice@npienumerator.com.
Mail: NPI Enumerator, P.O. Box 6059, Fargo, ND
48.To be signed by the physician supervising the patient’s kidney treatment. Signature of physician identified in Item 45. A stamped signature is unacceptable.
49.Enter date physician signed this form.
50.To be signed by the physician who is currently following the patient. If the patient had decided initially not to file an application for Medicare, the physician will be
51.The date physician
52.This remarks section may be used for any necessary comments by either the physician, patient, ESRD Network or social security field office.
53.The patient’s signature authorizing the release of information to the Department of Health and Human Services must
be secured here. If the patient is unable to sign the form, it should be signed by a relative, a person assuming responsibility for the patient or by a survivor.
54.The date patient signed form.
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is
FORM |
7 |
Form Characteristics
| Fact Name | Details |
|---|---|
| Purpose | The CMS-2728 U3 form is used to document medical evidence and patient information for those eligible for Medicare entitlement related to end-stage renal disease (ESRD). |
| Eligibility Requirement | This form must be completed for all ESRD patients beginning a regular course of dialysis or receiving a kidney transplant. |
| Submission Timeline | Providers must submit the CMS-2728 U3 within 45 days of starting dialysis or indicating the need for a transplant. |
| Governing Law | The use of this form complies with the Social Security Act, specifically Section 226A. |
| Patient Information | Key details required include the patient's name, Medicare Beneficiary Identifier (or Social Security Number), date of birth, and current medical coverage. |
| Additional Information | Completing the form involves specific sections for dialysis patients, transplant patients, and those undergoing self-dialysis training. |
Guidelines on Utilizing Cms 2728 U3
Once you have gathered the necessary information, it’s time to complete the CMS 2728 U3 form. Adhering to these clear steps will ensure that all sections are filled out correctly, paving the way for a smooth application process. After submission, the form will be reviewed, and you may await further instructions regarding Medicare coverage for the patient.
- Start with the patient’s full legal name. Ensure it matches the name on the Medicare or Social Security card.
- Input the Medicare Beneficiary Identifier or Social Security Number, depending on which is applicable.
- Include the patient’s date of birth, formatted as two-digit month, day, and four-digit year (mm/dd/yyyy).
- Provide the patient’s mailing address, consisting of street number, city, state, and ZIP code.
- Enter the patient’s phone number, including the area code.
- Select the patient’s sex by checking the appropriate box.
- Indicate the patient's ethnicity by checking the corresponding box.
- If the patient is Hispanic or Latino, complete the country/area of origin or ancestry section.
- Check all applicable boxes to identify the patient's race, as self-identified.
- Answer whether the patient is applying for ESRD Medicare coverage by selecting "Yes" or "No."
- List all forms of current medical coverage by checking the relevant boxes.
- Provide the patient’s height and dry weight in appropriate units.
- Specify the primary cause of renal failure by selecting the correct code from the provided list.
- Note the employment status for the past six months and current conditions.
- Detail any co-morbid conditions by checking all that apply.
- Complete the section about prior therapies, including erythropoietin usage and nephrology care.
- Fill out laboratory values collected within 45 days prior to the most recent ESRD episode.
- If applicable, provide details regarding the dialysis facility, type of dialysis, and treatment dates.
- For transplant patients, include transplant data and current status.
- If applicable, complete details for self-dialysis training, including training dates and provider information.
- Ensure the physician involved signs the form where applicable.
- Lastly, have the patient sign and date the authorization section.
What You Should Know About This Form
1. What is the CMS 2728 U3 form?
The CMS 2728 U3 form, also known as the End Stage Renal Disease Medical Evidence Report, is a document used to establish a patient’s entitlement to Medicare benefits due to End Stage Renal Disease (ESRD). It collects essential information about the patient’s medical history, current treatment, and demographic details. Completing this form is a critical step in ensuring that patients can access the care and coverage they need as they face the challenges of renal disease.
2. Who needs to complete the CMS 2728 U3 form?
This form must be completed for all patients who have been diagnosed with end stage renal disease, representing a permanent and irreversible stage of kidney failure. It is necessary for patients starting dialysis treatment or those receiving a kidney transplant. Additionally, patients reapplying for Medicare benefits after a period discontinuation, or those who have received supplemental care, must also complete this form.
3. How is the form submitted?
The completed CMS 2728 U3 form must be submitted to the Social Security Administration office that services the patient’s claim. It’s important to ensure that all required information is filled out correctly, as errors could delay the processing of Medicare entitlement. Additionally, a copy should be maintained by the dialysis facility or healthcare provider involved in the patient’s care.
4. What kind of information is collected on the form?
The CMS 2728 U3 form collects a variety of information, including the patient's personal details like name, address, date of birth, and Medicare Beneficiary Identifier. Medical history, current treatment plans, the cause of renal failure, and details regarding any ongoing dialysis treatments or transplant procedures are also documented. This comprehensive data helps to assess the patient’s needs and eligibility for Medicare benefits.
5. What happens after the form is submitted?
Once the CMS 2728 U3 form is submitted to the Social Security Administration, it is reviewed to determine the patient's eligibility for Medicare benefits due to ESRD. If approved, the patient will begin receiving the benefits that cover necessary expenses associated with their treatment. If there are any issues with the submission or eligibility, the patient may be contacted to provide additional information or clarification.
6. What is the significance of patient demographics on the form?
Patient demographics, including sex, ethnicity, and race, are crucial as they help ensure compliance with federal reporting requirements. This information is collected for statistical and research purposes and is vital for understanding how different populations are affected by ESRD. Accurate demographic information also supports the development of healthcare policies that address the needs of diverse patient groups.
7. Can the form be updated or amended?
Yes, if there are changes in the patient's condition or treatment after the form has been submitted, the CMS 2728 U3 can be updated. It’s important for the healthcare provider to submit any necessary amendments to reflect the current medical status accurately. Keeping this information up-to-date ensures that the patient receives the appropriate benefits without any disruptions.
8. What if a patient is not eligible for Medicare?
If a patient is found ineligible for Medicare benefits after submitting the CMS 2728 U3 form, they may explore other options for coverage. There could be state programs or private insurance plans available that provide financial assistance for medical expenses related to renal disease. It can be beneficial for patients to speak with a social worker or financial counselor familiar with healthcare options for further guidance.
9. Why is it important to complete the form within the specified time frame?
Completing the CMS 2728 U3 form within the designated 45-day window is essential to ensure swift access to necessary Medicare benefits. Delays in submission can result in interruptions in treatment coverage, putting the patient at risk of medical complications. Moreover, timely completion helps in avoiding complications with eligibility, which can prolong the approval process for needed healthcare services.
Common mistakes
Filling out the CMS 2728 U3 form for End Stage Renal Disease can be a complex task, and errors can lead to delays in processing applications for Medicare entitlement. One common mistake occurs with identifying the patient's legal name. It is crucial that the name matches exactly as it appears on the patient's Medicare or Social Security card. A minor discrepancy, such as a change in middle initials or order of the last names, can result in significant issues affecting the verification process.
Another frequent error lies in entering the Medicare Beneficiary Identifier or Social Security Number. Individuals may mistakenly use an outdated Social Security Number or fail to populate the identifier accurately. It's important to check that the number provided correlates with the current Medicare card to avoid unnecessary complications. In the absence of a Medicare Beneficiary Identifier, the Social Security Number is acceptable only if entered correctly.
People often overlook co-morbid conditions, which should be checked accurately in the form. This section asks for all relevant medical conditions the patient has experienced over the last ten years. Not reporting existing conditions may lead to an incomplete evaluation of the patient’s eligibility for benefits, potentially hindering the application process. It is advisable to review the patient's medical history carefully and check all applicable boxes.
Finally, errors can occur in indicating whether the patient is applying for ESRD Medicare coverage. Some individuals may forget to mark 'Yes' or 'No' correctly in this section. This detail is vital for processing the application appropriately. A missed checkbox can result in automatic denial or delays. Therefore, reviewing the entire document before submission for any unchecked items is a best practice.
Documents used along the form
The CMS 2728 U3 form is an important document for individuals facing End Stage Renal Disease (ESRD). To support this process, several other documents may be required or beneficial for patients and healthcare providers. Below is a list of common forms that are often used alongside the CMS 2728 U3 form. Each document plays a vital role in ensuring comprehensive care and proper management of ESRD.
- CMS 2728 Fact Sheet: This document provides a summary of the CMS 2728 U3 form's purpose and instructions, outlining what information is needed and why it matters for Medicare eligibility.
- Medicare Application for Health Coverage (Form CMS-40B): This form is used to apply for Medicare coverage, whether for the first time or for re-enrollment. It helps ensure that patients receive necessary healthcare services.
- ESRD Certification Form (Form CMS-2746): This certification is specifically for patients transitioning from dialysis to kidney transplant evaluation or treatment. It verifies that a patient meets the necessary criteria for kidney transplantation.
- Dialysis Facility Information Form (Form CMS-2744): This form collects information about the patient's dialysis facility. It includes the facility's Medicare provider number and services offered, ensuring streamlined communications between providers.
- Patient Assignment of Benefits Form: Through this document, patients allow healthcare providers to bill Medicare directly for ESRD-related services. It simplifies the billing process and ensures that claims are submitted accurately.
- Advanced Beneficiary Notice of Non-coverage (ABN): This form alerts patients when a Medicare service is likely to be denied. It encourages informed decision-making regarding treatment options and potential financial responsibilities.
- Social Security Number (SSN) Card: A copy of the patient's SSN card is often required for verifying identity and for filling out forms that involve Medicare enrollment.
- Medical Records Release Authorization: Patients use this form to authorize their healthcare providers to share their medical records with Medicare or other relevant organizations, facilitating eligibility review.
- Patient Care Plan: This document outlines the patient's treatment and care strategy for managing ESRD, including dialysis schedules and medication management. It helps ensure that all healthcare providers are aligned in their approach.
Collectively, these documents provide essential support and clarity during what can be a challenging time for patients and their families. Each plays a specific role within the broader context of ESRD care and Medicare processes, ensuring that patients receive the appropriate resources and support they need.
Similar forms
The CMS 2728 U3 form is pivotal for documenting the medical evidence required for Medicare entitlement for patients with end-stage renal disease (ESRD). Several other documents serve similar functions in healthcare or entitlement processes. Here are five notable examples:
- Form CMS-1450: This form is used by hospitals to bill Medicare for services provided. It captures information about the patient's medical condition and treatment, similar to how CMS 2728 U3 collects data regarding renal disease and treatment needs.
- CMS 1500 Form: Healthcare providers use this form to bill Medicare for outpatient services. Like the CMS 2728 U3, it requires details about the patient’s diagnosis and treatment, facilitating claims processing.
- Form CMS-940: This is a Medicare Outpatient Therapy Cap Exception Application. It documents medical necessity for therapies, much like the CMS 2728 U3 establishes medical necessity for ESRD services.
- Form 855I: This Medicare enrollment application for individual providers captures essential information to determine eligibility, paralleling how the CMS 2728 U3 assesses ESRD eligibility for Medicare coverage.
- Patient Health Questionnaire (PHQ-9): This form screens for depression among patients and records relevant health information. Similar to the CMS 2728 U3, it aids in managing patient care by documenting vital health data.
Dos and Don'ts
When filling out the CMS 2728 U3 form, follow these guidelines:
- Provide Accurate Information: Ensure all fields are filled out correctly.
- Use Legal Names: Enter the patient’s legal name as it appears on the Medicare card.
- Verify Medicare Identifier: Include the correct Medicare Beneficiary Identifier or Social Security Number.
- Complete Within 45 Days: Submit the form within 45 days of the patient's dialysis treatment start date.
- Check All Relevant Boxes: Mark all applicable items regarding the patient’s medical history and current conditions.
- Ensure Signatures: Obtain signatures from both the physician and the patient where required.
- Double-check for any missing information before submission.
- Review eligibility criteria for Medicare benefits carefully.
- Do Not Leave Fields Blank: Every section should have a response if applicable.
- Avoid Abbreviations: Do not use abbreviations that may cause confusion.
- Never Submit for Acute Renal Failure: This form should not be completed for patients with acute renal failure.
Misconceptions
Understanding the CMS 2728 U3 form is crucial for patients with End-Stage Renal Disease (ESRD) who are seeking Medicare benefits. However, misconceptions about this form abound, leading to confusion and potential issues during the application process. Here’s a look at seven common misconceptions:
- This form is only for patients who are currently on dialysis. Many believe that the CMS 2728 U3 form is reserved solely for patients already undergoing dialysis. In reality, it must also be completed for individuals who are about to start dialysis or are applying for a kidney transplant.
- Completing the form guarantees immediate Medicare coverage. Some patients think that filling out the CMS 2728 U3 form automatically enrolls them in Medicare. While this form is essential for determining entitlement, it does not guarantee prompt coverage. Approval depends on various factors, including eligibility assessments.
- Only doctors can fill out the entire form. Many assume that only physicians have the authority to complete the CMS 2728 U3 form. However, it can also be filled out by qualified healthcare professionals, such as nurse practitioners or social workers who are involved in the patient’s care.
- All sections of the form must be completed in every case. While thoroughness is important, not every section of the form is necessary for all patients. For instance, sections on training for self-dialysis are only required for those who are specifically going through that process.
- The form is unnecessary if the patient has been treated for kidney issues in the past. Some individuals think that previous treatments or diagnoses exempt them from submitting the CMS 2728 U3 form. However, any new application for Medicare benefits related to ESRD must involve this form, regardless of past medical history.
- The information collected is solely for Medicare purposes. There is a belief that the data gathered through the CMS 2728 U3 form is only used for Medicare enrollment. In fact, the information can also inform medical research and public health initiatives designed to improve care for patients with ESRD.
- Submitting incorrect information is not a serious issue. Some patients feel that small mistakes on the form won’t matter. However, providing inaccurate or incomplete information can lead to delays or denials of Medicare coverage, which can significantly affect patient care.
By addressing these misconceptions, patients can be better prepared to navigate the Medicare application process effectively and ensure their needs are met.
Key takeaways
The CMS 2728 U3 form is essential for patients with End Stage Renal Disease (ESRD) seeking Medicare benefits. Here are key takeaways to understand how to fill it out and utilize it effectively:
- Purpose of the Form: This form is used to establish a patient's entitlement to Medicare benefits related to ESRD, including dialysis and kidney transplants.
- Who Should Fill It Out: The attending physician, head nurse, or social worker involved in a patient’s treatment must complete specific sections, while other sections are to be filled out by the patient.
- Required Information: Patients must provide their legal name, Medicare Beneficiary Identifier (or Social Security Number if not yet assigned), date of birth, mailing address, and phone number.
- Ethnic and Racial Identification: It is necessary for patients to identify their ethnicity and race to comply with Federal statistics. Options include categories like Hispanic or Latino, White, Black or African American, among others.
- Medical Coverage: Patients should indicate current medical coverage options, such as Medicaid, Medicare, or other health insurance plans.
- Employment Status: The section regarding employment status is important to capture the patient's current work situation, which may affect eligibility for benefits.
- Co-Morbid Conditions: The form requires listing any additional health conditions alongside ESRD, which can impact treatment plans and eligibility.
- Laboratory Values: Recent lab values related to renal function must be reported within 45 days prior to the most recent ESRD episode, ensuring a comprehensive medical history is attached to the application.
- Submissions: After completing the form, it must be submitted to the appropriate Social Security office and retained by the dialysis facility's records.
Browse Other Templates
Meta Ad Specs - Name: Jenna Robinson, an enthusiastic hiker conquering every trail.
Genealogy Research Forms - Occupational information allows for a deeper understanding of family roles and societal contributions.