Fill Out Your Cologuard Order Form
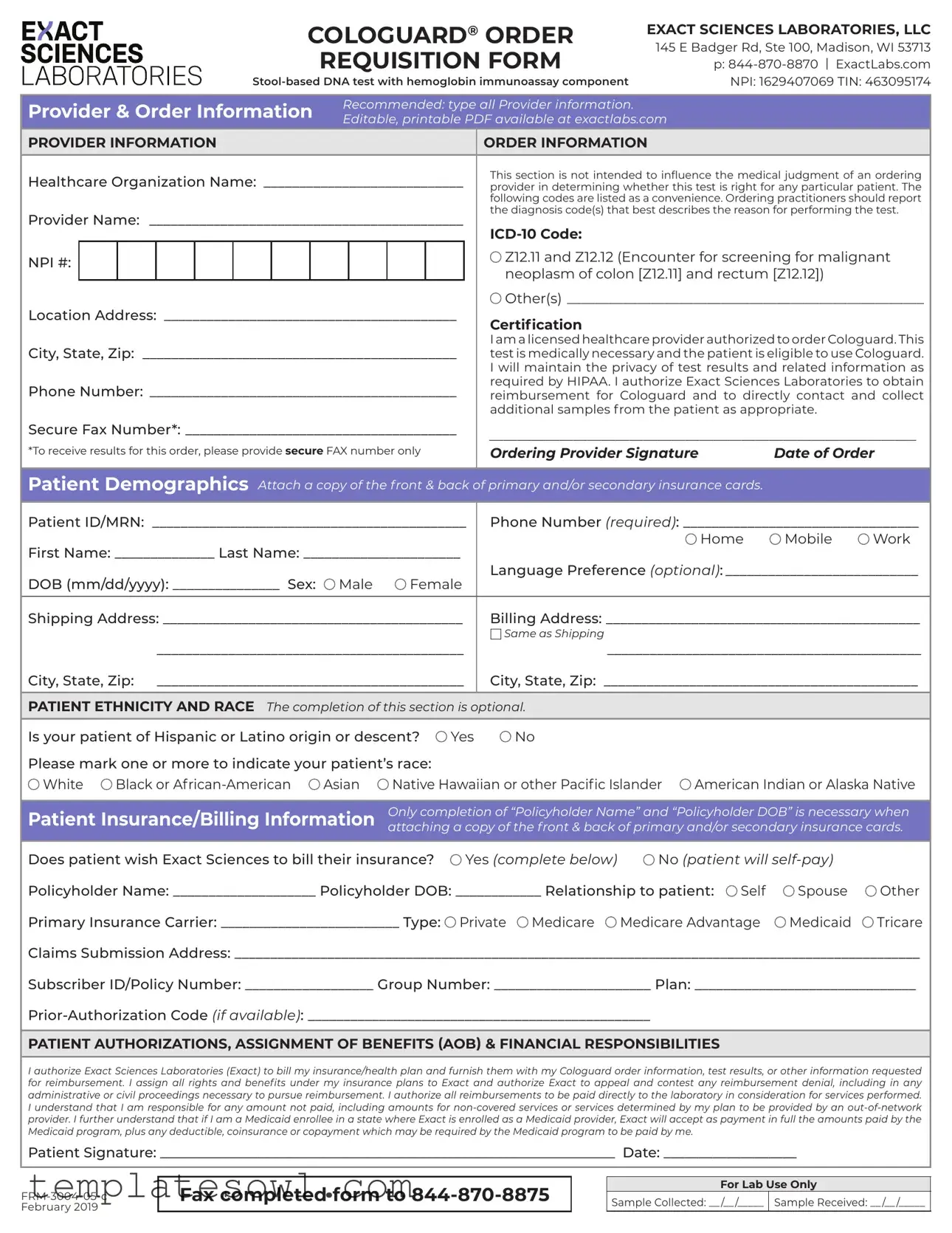
The Cologuard Order form is an essential document designed for healthcare providers to facilitate the ordering of the Cologuard test, a stool-based DNA examination that offers an innovative approach to colon cancer screening. This requisition form is produced by Exact Sciences Laboratories and outlines critical information pertaining to the provider, patient demographics, insurance billing, and necessary authorizations for test processing. Each section of the form plays a pivotal role: the provider information mandates key details that confirm the healthcare professional's credentials, while the patient demographics collect vital information for the test and insurance coverage. The form emphasizes the importance of patient consent through signatures, ensuring that results remain confidential in compliance with HIPAA regulations. Additionally, the order form includes sections for insurance billing, allowing patients to decide whether they prefer to have their insurance billed or wish to self-pay. With a focus on thorough documentation, the Cologuard Order form ensures that healthcare providers can efficiently navigate the process of ordering the test, providing a streamlined experience for their patients. The layout is user-friendly, featuring editable fields for ease of completion and the opportunity to attach necessary insurance documentation, helping to make the entire process simpler and more efficient for both providers and patients alike.
Cologuard Order Example
|
|
|
|
|
|
|
COLOGUARD® ORDER |
EXACT SCIENCES LABORATORIES, LLC |
|||||||||
|
|
|
|
|
|
|
|
|
REQUISITION FORM |
145 E Badger Rd, Ste 100, Madison, WI 53713 |
|||||||
|
|
|
|
|
|
|
|
|
|
p: |
|||||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
NPI: 1629407069 TIN: 463095174 |
||||||||||
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Provider & Order Information |
Recommended: type all Provider information. |
|
|
||||||||||||||
Editable, printable PDF available at exactlabs.com |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||
PROVIDER INFORMATION |
|
|
|
|
|
ORDER INFORMATION |
|
||||||||||
Healthcare Organization Name: _____________________________ |
This section is not intended to influence the medical judgment of an ordering |
||||||||||||||||
provider in determining whether this test is right for any particular patient. The |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
following codes are listed as a convenience. Ordering practitioners should report |
|||
Provider Name: _____________________________________________ |
the diagnosis code(s) that best describes the reason for performing the test. |
||||||||||||||||
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
NPI #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Z12.11 and Z12.12 (Encounter for screening for malignant |
|||
|
|
|
|
|
|
|
|
|
|
|
|
neoplasm of colon [Z12.11] and rectum [Z12.12]) |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Location Address: __________________________________________ |
Other(s)____________________________________________________ |
||||||||||||||||
Certification |
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
City, State, Zip: _____________________________________________ |
I am a licensed healthcare provider authorized to order Cologuard. This |
||||||||||||||||
test is medically necessary and the patient is eligible to use Cologuard. |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I will maintain the privacy of test results and related information as |
|||
Phone Number: ____________________________________________ |
required by HIPAA. I authorize Exact Sciences Laboratories to obtain |
||||||||||||||||
reimbursement for Cologuard and to directly contact and collect |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
additional samples from the patient as appropriate. |
|||
Secure Fax Number*: ______________________________________ |
_____________________________________________________________ |
||||||||||||||||
*To receive results for this order, please provide secure FAX number only |
|||||||||||||||||
Ordering Provider Signature |
Date of Order |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Demographics Attach a copy of the front & back of primary and/or secondary insurance cards.
Patient ID/MRN: ____________________________________________ |
Phone Number (required): _________________________________ |
||||||||||
First Name: ______________ Last Name: ______________________ |
|
|
Home |
Mobile |
Work |
||||||
Language Preference (optional):____________________________ |
|||||||||||
DOB (mm/dd/yyyy): _______________ Sex: |
Male |
Female |
|||||||||
|
|
|
|
|
|
||||||
Shipping Address: __________________________________________ |
Billing Address: ____________________________________________ |
||||||||||
|
|
|
|
|
Same as Shipping |
|
|
|
|
|
|
|
___________________________________________ |
____________________________________________ |
|||||||||
City, State, Zip: ___________________________________________ |
City, State, Zip: ____________________________________________ |
||||||||||
|
|
|
|
|
|
|
|||||
PATIENT ETHNICITY AND RACE The completion of this section is optional. |
|
|
|
|
|
||||||
Is your patient of Hispanic or Latino origin or descent? |
Yes |
No |
|
|
|
|
|
||||
Please mark one or more to indicate your patient’s race: |
|
|
|
|
|
|
|
||||
White |
Black or |
Asian |
Native Hawaiian or other Pacific Islander |
American Indian or Alaska Native |
|||||||
|
|
|
|
|
|||||||
Patient Insurance/Billing Information |
Only completion of “Policyholder Name” and “Policyholder DOB” is necessary when |
||||||||||
attaching a copy of the front & back of primary and/or secondary insurance cards. |
|||||||||||
|
|
|
|
|
|||||||
Does patient wish Exact Sciences to bill their insurance? |
Yes (complete below) |
No (patient will |
|
||||||||
Policyholder Name: ____________________ Policyholder DOB: ____________ Relationship to patient: |
Self |
Spouse |
Other |
||||||||
Primary Insurance Carrier: _________________________ Type: |
Private Medicare |
Medicare Advantage |
Medicaid |
Tricare |
|||||||
Claims Submission Address: ________________________________________________________________________________________________
Subscriber ID/Policy Number: __________________ Group Number: ______________________ Plan: _______________________________
PATIENT AUTHORIZATIONS, ASSIGNMENT OF BENEFITS (AOB) & FINANCIAL RESPONSIBILITIES
I authorize Exact Sciences Laboratories (Exact) to bill my insurance/health plan and furnish them with my Cologuard order information, test results, or other information requested for reimbursement. I assign all rights and benefits under my insurance plans to Exact and authorize Exact to appeal and contest any reimbursement denial, including in any administrative or civil proceedings necessary to pursue reimbursement. I authorize all reimbursements to be paid directly to the laboratory in consideration for services performed. I understand that I am responsible for any amount not paid, including amounts for
Patient Signature: _________________________________________________________________ Date: ___________________
Fax completed form to
For Lab Use Only
Sample Collected: __ /__ /_____ Sample Received: __ /__ /_____
Form Characteristics
| Fact Name | Details |
|---|---|
| Test Type | Cologuard is a stool-based DNA test with a hemoglobin immunoassay component. |
| Provider Information | All provider information must be typed and is editable via an online PDF form. |
| ICD-10 Codes | Relevant codes for colon cancer screening include Z12.11 and Z12.12. |
| Healthcare Provider Certification | Providers must confirm their licensure and test necessity for patient eligibility. |
| Patient Demographics | Essential details such as Patient ID, name, and DOB must be completed. |
| Patient Insurance Information | If applicable, includes necessary details such as policyholder name and insurance type. |
| Fax Number Requirement | A secure fax number is mandatory to receive results for the Cologuard order. |
Guidelines on Utilizing Cologuard Order
Once you have the Cologuard Order form in hand, you'll want to ensure that each section is filled out correctly. Gathering the necessary information before starting can help streamline the process. This step-by-step guide will assist you in completing the form efficiently.
- Begin by filling in the Provider Information section, including the Healthcare Organization Name, Provider Name, NPI number, and contact details.
- In the Order Information section, provide the required diagnostic codes and confirm that you are a licensed healthcare provider authorized to order Cologuard.
- Next, sign and date the order to validate it.
- Move to the Patient Demographics section. Enter details such as Patient ID/MRN, phone number, name, date of birth, and sex.
- Complete the Shipping Address and Billing Address sections, noting if they are the same.
- For the Patient Ethnicity and Race section, indicate if the patient is Hispanic or Latino and check the appropriate boxes for their race.
- In the Patient Insurance/Billing Information section, fill out the necessary fields, including the Policyholder's information only if you’re attaching the insurance cards.
- Complete the Patient Authorizations, Assignment of Benefits (AOB) & Financial Responsibilities section by signing and dating the authorization to bill your insurance.
- Finally, ensure the completed form is sent to the designated fax number (844-870-8875).
After submitting the form, the next steps involve the processing of the order, including insurance verification and sample collection scheduling. All information should remain confidential, adhering to proper privacy guidelines.
What You Should Know About This Form
What is the Cologuard Order form and its purpose?
The Cologuard Order form is a requisition form used by healthcare providers to order Cologuard, a stool-based DNA test combined with a hemoglobin immunoassay. This test is designed to screen for colorectal cancer in patients who meet specific criteria. The form collects essential information about the provider, the patient, and insurance details, ensuring that all parties have the necessary documentation for testing and billing purposes.
How do I fill out the Cologuard Order form?
Filling out the Cologuard Order form requires careful attention to detail. Start by entering all provider information at the top section, including the healthcare organization name and the provider’s NPI (National Provider Identifier) number. Proceed to the order section, where you'll provide the ICD-10 code that best represents the reason for the test. Make sure to complete the patient demographics, including contact information and insurance details. Remember to attach copies of the patient’s insurance cards if relevant, and ensure that you, as the ordering provider, confirm your authority to order this test by signing and dating the form.
Is insurance billing available for Cologuard, and how does it work?
Yes, insurance billing is available for Cologuard. When completing the order form, you have the option to indicate whether the patient wishes to have their insurance billed. If so, you must provide the policyholder’s name and date of birth, along with other necessary insurance details such as the primary insurance carrier and policy numbers. The submitted form allows Exact Sciences to bill the insurance company directly for reimbursement. If any costs are not covered by insurance, the patient is informed of their financial responsibilities before proceeding with the test.
What happens to my patient’s test results?
The patient's test results from Cologuard will be handled with the utmost care following HIPAA privacy regulations. Upon completion of the test, results will be sent to the secure fax number provided on the order form. This protects the confidentiality of the patient’s information while ensuring that the healthcare provider receives the results to discuss with the patient. It’s essential that the ordering provider maintains the patient's privacy and follows all relevant guidelines regarding the handling of sensitive information.
What if the patient does not have insurance or prefers to self-pay?
If the patient prefers to self-pay or does not have insurance, the ordering provider should select the option on the Cologuard Order form that indicates the patient will self-pay. In this case, you do not need to provide insurance information. It is essential for the provider to inform the patient about the costs involved and any financial responsibilities that come with opting for the self-pay route to ensure that there are no surprises later on.
Common mistakes
When completing the Cologuard Order form, errors can lead to delays in testing and potentially impact patient care. First, individuals often overlook the complete provider information. It is critical to provide all required details, including the healthcare organization name, provider name, and NPI number. Missing or incorrect information may lead to difficulties in processing the test or retrieving results.
Another common mistake occurs in the patient demographic section. Incomplete or inaccurate data here can affect reimbursement and test handling. Ensure patient details such as ID, phone number, and date of birth are filled out clearly. Pay attention to correct spelling of names to avoid complications with insurance billing and communications.
Additionally, individuals frequently neglect the insurance information portion of the form. Failing to provide accurate details about the policyholder, insurance carrier, and any required codes can result in delays or the rejection of claims. Double-check that all fields are filled correctly before submission.
Lastly, not signing the order form can be a critical oversight. The ordering provider’s signature and date of order are essential for validating the request. Without these, the form may be considered incomplete, halting the testing process. Always review the form thoroughly to ensure everything is properly signed and dated.
Documents used along the form
The Cologuard Order form is essential for patients undergoing the stool-based DNA test. However, there are several other documents that are often used in conjunction with this form to ensure a smooth process. Here are some of the common forms you might encounter.
- Patient Authorization Form: This document gives healthcare providers permission to disclose the patient's medical information required for testing and billing purposes. It ensures that the patient's data remains confidential while allowing necessary communication between the laboratory and insurance companies.
- Insurance Information Form: A crucial document, this form collects detailed information about the patient’s insurance coverage. This includes policyholder information, insurance carrier details, and claims submission addresses, which will assist in processing billing more efficiently.
- ICD-10 Coding Reference Guide: This guide provides healthcare professionals with the appropriate diagnosis codes used to justify the medical necessity of the Cologuard test. It offers a quick reference to ensure that the correct codes are reported, facilitating accurate billing and preventing reimbursement issues.
- Privacy Notice: This document outlines how the patient's health information will be protected under HIPAA guidelines. It communicates the rights patients hold concerning their medical records and assures them that their data will be handled responsibly.
Utilizing these documents alongside the Cologuard Order form helps streamline the testing process and ensures compliance with regulatory requirements. It is essential to have all necessary documentation in order to prevent delays and complications.
Similar forms
- Prescription Form: Much like the Cologuard Order form, a prescription form gathers essential patient and provider information. Both documents require the provider’s signature and demonstrate medical necessity. They serve as formal instructions for patients to receive necessary medical tests or medications.
- Referral Form: A referral form is similar in structure as it includes patient demographics and reason for referral. Just like the Cologuard Order form, it is used to authorize the consultation with another healthcare provider, facilitating patient care continuity.
- Insurance Claim Form: This form captures detailed information related to insurance coverage, just as the Cologuard Order form collects billing information. Both documents require patient and policyholder details and are essential for the reimbursement process, ensuring that healthcare services are billed correctly.
- Health History Form: The health history form seeks comprehensive information about a patient’s medical background, similar to how the Cologuard Order form collects demographics. Both documents aim to provide essential data that health professionals need to deliver effective and tailored patient care.
Dos and Don'ts
When filling out the Cologuard Order form, attention to detail is crucial. Here is a list of things to do and avoid:
- Do ensure that all provider information is typed clearly to minimize errors.
- Do attach a copy of the front and back of the primary and/or secondary insurance cards as required.
- Do check that the Patient ID/MRN and all contact information are filled out accurately.
- Do indicate the patient's ethnicity and race if information is available and appropriate to disclose.
- Don't leave any required fields blank, as this may delay processing.
- Don't use illegible handwriting; typed information is preferred.
- Don't forget to sign and date the order; an unsigned form cannot be processed.
- Don't provide a personal fax number instead of a secure one, as this violates privacy regulations.
Misconceptions
Understanding the Cologuard order form can be tricky, and several misconceptions can create confusion. Here are six common misunderstandings explained.
- Only Certain Providers Can Use the Cologuard Order Form: While the form is intended for use by licensed healthcare providers, it does not imply that only specific providers can order the test. All qualified providers can assess the patient's eligibility and determine if Cologuard is appropriate for them.
- The Form is Complicated and Hard to Fill Out: Many believe that the order form is overly complex. In reality, it has clear sections for provider and patient information which can be filled out easily, especially with a little guidance.
- Insurance Coverage is Guaranteed With the Form: Some patients assume that simply filling out the order form ensures insurance will cover the test. However, coverage depends on the patient's specific insurance plan and the medical necessity as determined by their provider.
- Patient Ethnicity and Race Information is Mandatory: There's a misconception that patients must provide information regarding their ethnicity and race. This section is completely optional, and patients can choose to skip it without any adverse effects.
- Only One Type of Insurance Can Be Billed: Another myth is that the order form can only be used for one insurance type, like Medicare or Medicaid. In fact, the form accommodates various insurance types, making it flexible for different patients' needs.
- Getting Results from Cologuard is Slow and Difficult: Many think that results from the Cologuard test take a long time to process. However, once the samples are collected and sent to Exact Sciences Laboratories, results are typically reported in a timely manner, providing peace of mind to both patients and providers.
Key takeaways
Here are seven key takeaways when filling out and using the Cologuard Order form:
- Provider Information: Ensure that all provider details are typed clearly. This includes the healthcare organization name, provider name, NPI number, and diagnosis codes.
- Authorization: The ordering provider must confirm their authorization to order Cologuard and state that the test is necessary for the patient.
- Insurance Information: Include a copy of the insurance cards for efficient billing. Key pieces, such as the policyholder's name and date of birth, are required when billing through insurance.
- Patient Consent: The patient must sign the authorization section, allowing Exact Sciences to bill insurance and handle test results.
- Contact Information: Provide accurate contact details for both the patient and the healthcare provider to ensure smooth communication.
- Privacy Compliance: Maintain compliance with HIPAA regulations by safeguarding the patient's information throughout the process.
- Faxing Instructions: After completion, fax the order form to the specified number to ensure that the test is processed promptly.
Browse Other Templates
Big R Jobs - Include your phone number for easier communication.
Authentication Form Global Affairs Canada - Each form submission must include verification through validators.