Fill Out Your Csa Dental Form
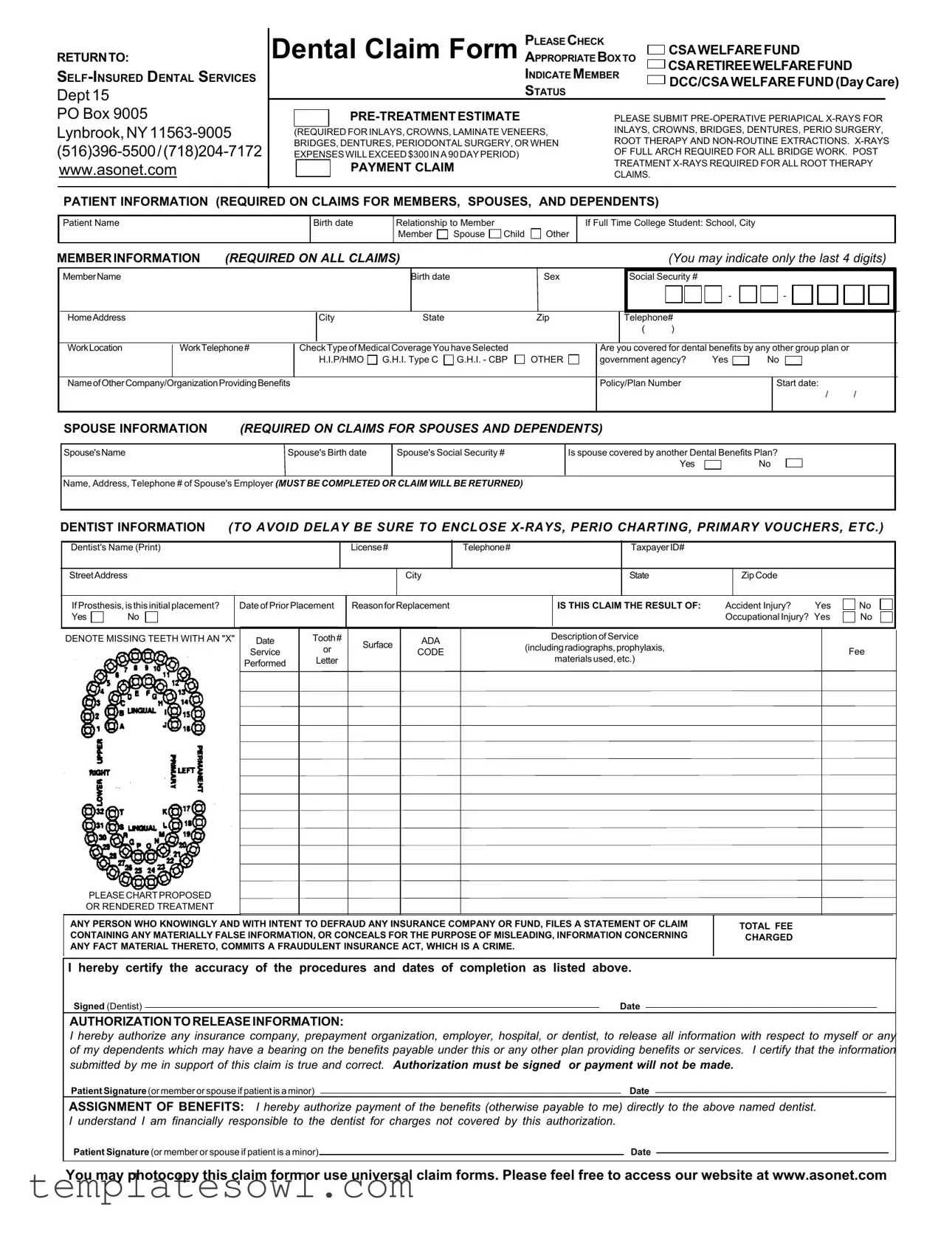
The CSA Dental form serves as a vital tool for individuals seeking to maximize their dental benefits through various plans. It encompasses essential sections for gathering personal information from the patient, member, and spouse, ensuring that every claim is accurate and comprehensive. Information required includes names, Social Security numbers, and relationships to the member, along with details about any preceding dental coverage. The form places particular emphasis on the inclusion of pre-treatment estimates, necessitating the submission of specific x-rays for various procedures such as crowns, bridges, and dentures. Moreover, a thorough section dedicated to dental provider information is included, which requires the dentist's license details and relevant treatment history. This ensures that claims are processed smoothly and efficiently. Another significant aspect of the form is the authorization section, allowing for the release of crucial information necessary for processing claims. By formally signing these sections, patients and members certify the accuracy of the information provided, thereby supporting the integrity of the claims process. Overall, the CSA Dental form is structured to facilitate a seamless experience for members and their families while catering to the requirements of insurance providers.
Csa Dental Example
RETURNTO:
PLEASE CHECK
Dental Claim Form APPROPRIATE BOX TO  CSAWELFAREFUND
CSAWELFAREFUND
CSARETIREEWELFAREFUND
Dept 15
INDICATE MEMBER
STATUS
DCC/CSAWELFAREFUND(DayCare)
PO Box 9005
|
|
PLEASE SUBMIT |
||
|
|
|
INLAYS, CROWNS, BRIDGES, DENTURES, PERIO SURGERY, |
|
(REQUIRED FOR INLAYS, CROWNS, LAMINATE VENEERS, |
||||
ROOT THERAPY AND |
||||
BRIDGES, DENTURES, PERIODONTAL SURGERY, OR WHEN |
||||
OF FULL ARCH REQUIRED FOR ALL BRIDGE WORK. POST |
||||
EXPENSES WILLEXCEED$300INA 90 DAY PERIOD) |
||||
TREATMENT |
||||
|
|
PAYMENT CLAIM |
||
|
|
CLAIMS. |
||
|
|
|
||
|
|
|
||
PATIENT INFORMATION (REQUIRED ON CLAIMS FOR MEMBERS, SPOUSES, AND DEPENDENTS)
Patient Name
Birth date
Relationship to Member |
|
|
Member |
Spouse |
Child |
Other
If Full Time College Student: School, City
MEMBERINFORMATION (REQUIRED ON ALL CLAIMS) |
(You may indicate only the last 4 digits) |
MemberName
Birth date |
Sex |
|
|
Social Security #
-
-
|
HomeAddress |
|
|
City |
State |
|
Zip |
|
Telephone# |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
WorkLocation |
WorkTelephone# |
CheckTypeofMedicalCoverageYouhaveSelected |
|
Are you covered for dental benefits by any other group plan or |
|
|
|
|||||||||||
|
|
|
|
H.I.P/HMO |
G.H.I. Type C |
G.H.I. - CBP |
OTHER |
government agency? |
Yes |
|
No |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NameofOtherCompany/OrganizationProvidingBenefits |
|
|
|
|
|
Policy/Plan Number |
|
|
|
Start date: |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SPOUSE INFORMATION (REQUIRED ON CLAIMS FOR SPOUSES AND DEPENDENTS)
Spouse'sName |
Spouse's Birth date |
Spouse's Social Security # |
|
|
|
Is spouse covered by another Dental Benefits Plan?
Yes |
|
No |
Name, Address, Telephone # of Spouse's Employer (MUST BE COMPLETED OR CLAIM WILL BE RETURNED)
DENTIST INFORMATION (TO AVOID DELAY BE SURE TO ENCLOSE
Dentist's Name (Print)
License#
Telephone#
TaxpayerID#
StreetAddress
City
State
ZipCode
IfProsthesis,isthisinitialplacement? |
|
DateofPrior Placement |
ReasonforReplacement |
|
IS THIS CLAIM THE RESULT OF: |
Accident Injury? |
Yes |
No |
|||
Yes |
No |
|
|
|
|
|
|
|
Occupational Injury? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
DENOTE MISSING TEETH WITH AN "X" |
Date |
Tooth# |
Surface |
ADA |
DescriptionofService |
|
|
|
|||
|
|
|
Service |
or |
CODE |
(includingradiographs,prophylaxis, |
|
|
Fee |
||
|
|
|
|
|
|
||||||
|
|
|
Performed |
Letter |
|
|
|
materialsused,etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLEASECHARTPROPOSED
OR RENDERED TREATMENT
ANY PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD ANY INSURANCE COMPANY OR FUND, FILES A STATEMENT OF CLAIM CONTAINING ANY MATERIALLY FALSE INFORMATION, OR CONCEALS FOR THE PURPOSE OF MISLEADING, INFORMATION CONCERNING ANY FACT MATERIAL THERETO, COMMITS A FRAUDULENT INSURANCE ACT, WHICH IS A CRIME.
TOTAL FEE CHARGED
I hereby certify the accuracy of the procedures and dates of completion as listed above.
Signed (Dentist) |
|
Date |
|
AUTHORIZATIONTORELEASEINFORMATION:
I hereby authorize any insurance company, prepayment organization, employer, hospital, or dentist, to release all information with respect to myself or any of my dependents which may have a bearing on the benefits payable under this or any other plan providing benefits or services. I certify that the information submitted by me in support of this claim is true and correct. Authorization must be signed or payment will not be made.
Patient Signature(or member or spouse if patient is a minor) |
|
Date |
|
ASSIGNMENT OF BENEFITS: I hereby authorize payment of the benefits (otherwise payable to me) directly to the above named dentist. I understand I am financially responsible to the dentist for charges not covered by this authorization.
Patient Signature (or member or spouse if patient is a minor) |
|
Date |
You may photocopy this claim form or use universal claim forms. Please feel free to access our website at www.asonet.com
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Purpose | This form is a Dental Claim Form used for submitting claims for dental services under CSA Dental services. |
| Member Information | It requires member details including name, birth date, social security number, and contact information. |
| Dependent Information | Claims must include patient information for members, spouses, and dependents. This includes names and relationships. |
| Pre-Treatment Estimates | Patients must submit pre-operative x-rays for specific treatments, such as crowns and root therapy, to avoid complications. |
| Authorization Requirement | The form includes authorization to release information for processing claims. Without the signature, claims may not be paid. |
| Fraud Warning | There’s a clear statement indicating consequences of filing fraudulent claims, highlighting the importance of accuracy. |
| Assignment of Benefits | The form allows for benefits to be paid directly to the dentist, ensuring that the dentist is compensated appropriately. |
| State-Specific Regulations | The rules governing the form may vary by state; refer to your state’s insurance regulations for specifics. |
Guidelines on Utilizing Csa Dental
Filling out the CSA Dental Claim Form can feel overwhelming, but it is an essential step in ensuring that you receive the benefits you deserve. Following the steps outlined below can help streamline the process, making it manageable and efficient. Be thorough and accurate in your responses, as incomplete forms may delay your claims.
- Begin by selecting the appropriate box at the top of the form, indicating whether you are submitting a claim to the CSA Welfare Fund, CSA Retiree Welfare Fund, or for Self-Insured Dental Services.
- Indicate your member status by choosing either DCC or CSA Welfare Fund (DayCare).
- Provide the required patient information. Include the patient’s name, birth date, and relationship to the member. If the patient is a full-time college student, include the school name and city.
- Fill in the member information. Enter the member’s name, birth date, sex, and the last four digits of their Social Security number. Additionally, provide the member's home address, city, state, zip code, and telephone numbers for both home and work.
- Tick the box indicating the type of medical coverage selected. Answer whether the member is covered for dental benefits by any other group plan or government agency, and if so, provide the necessary company information.
- Complete the information for the spouse, if applicable. Include their name, birth date, Social Security number, and check if they are covered by another dental benefits plan. Provide the spouse's employer's name, address, and telephone number.
- Enter the dentist's information. Include their name, license number, telephone number, taxpayer ID number, and address. If the treatment involves prosthesis, indicate whether it is the initial placement and provide details about prior placements if applicable.
- Answer questions regarding any accidents or occupational injuries that may relate to the claim.
- Denote any missing teeth with an "X" and chart the proposed or rendered treatment, including the procedure or service codes, descriptions, dates, and fees associated with the services performed.
- Read and understand the statement regarding fraudulent claims, ensuring that you provide accurate information.
- Have the dentist sign and date the form, certifying the accuracy of the procedures and dates listed.
- Sign the form to authorize the release of information necessary for processing the claim. If the patient is a minor, a member or spouse must sign on their behalf.
- Fill out the assignment of benefits, allowing payment directly to the dentist, and ensuring you understand your financial responsibility for any non-covered charges.
After completing the form, double-check all information for accuracy and completeness. Gather any required documents, such as X-rays or treatment plans, and send everything to the appropriate address. You can also visit the provider's website for additional support or questions regarding your submission.
What You Should Know About This Form
What is the purpose of the CSA Dental Form?
The CSA Dental Form is used to submit dental claims for reimbursement under specific welfare fund plans. It collects necessary information regarding the patient, the member, and the dental provider to ensure that claims are processed efficiently. It includes sections for pre-treatment estimates, detailed treatment information, and necessary authorizations for payment.
What information do I need to provide on the form?
You must provide several key pieces of information, including the patient’s name, birth date, relationship to the member, and the member's information such as their name, birth date, and contact details. You’ll also need to include details about any other dental benefits the member or spouse might have. Additionally, dentist information, treatment codes, and total fees charged must be documented.
Are X-rays required for all claims?
X-rays are not required for all claims, but they are mandatory for certain procedures. For services such as inlays, crowns, bridges, dentures, and other non-routine treatments, pre-operative X-rays are essential. Claims for root therapy also necessitate X-rays. Make sure to check the specifics for your treatment type to avoid any delays in processing your claim.
What happens if I fail to sign the authorization section?
If you do not sign the authorization section of the form, your claim may not be processed. This signature is crucial as it authorizes the release of information necessary for the claim evaluation. Without it, the insurance company may not be able to determine your eligibility for benefits, leading to delays or denial of your claim.
What is the process after submission of the CSA Dental Form?
Once the CSA Dental Form is submitted, it will be reviewed by the appropriate representatives from the welfare fund. They will process the claim and determine the reimbursement amount based on the submitted documentation and eligibility criteria. It is advisable to keep a copy of the submitted form and any additional documents for your records.
Common mistakes
Completing the CSA Dental claim form can be a straightforward process, but several common mistakes often lead to delays or complications in processing claims. Recognizing these errors can help individuals ensure their submissions are correct and complete.
One significant mistake is failing to provide complete patient information. The form requires the patient's name, birth date, and relationship to the member. When any of this information is missing or incorrectly filled, the claim may be returned for correction. It is crucial to double-check that all fields are filled out completely and accurately.
Another common error involves the member information section. Some individuals neglect to include the member's social security number or only provide a partial number. This oversight can hinder the claims process. Members should ensure that the social security number, especially the last four digits, are accurately reported to avoid any issues.
Additionally, some claimants fail to include the necessary documentation, such as X-rays or previous treatment details. The form specifically mentions the need for pre-operative X-rays for various types of dental work. Without these supporting materials, claims may be delayed or denied entirely. It is essential to gather all required documentation before submitting the form.
Furthermore, misunderstanding coverage can lead to mistakes. Individuals sometimes incorrectly assume they are covered under certain plans or fail to check if their spouse has additional dental benefits. This misunderstanding necessitates accurately indicating whether the patient has coverage under any other plan and providing details for that plan if applicable.
Lastly, signatures can often be overlooked. Authorization to release information and assignment of benefits both require the patient’s signature, or if the patient is a minor, the signature of a member or spouse. Claims without proper signatures can be returned, causing unnecessary delays. It is always wise to read through the entire form carefully to ensure every section, including signatures, is correctly completed.
Documents used along the form
The CSA Dental form is a critical document for processing dental claims. It helps ensure that necessary information regarding the patient, member, and dentist is collected accurately. In addition to this form, several other documents and forms are often required to facilitate the dental claims process. Below is a list of some key forms that may be used alongside the CSA Dental form.
- Dental Treatment Plan: This outlines the recommended dental treatments, estimated costs, and the timeframe for the procedures. It provides context and justification for the claims being filed.
- Pre-Treatment Estimate: Typically requested before commencing any significant dental work, this document details estimated costs and helps members understand their financial responsibilities in advance.
- X-ray Documentation: Required for certain procedures, this includes radiographic images that support the need for specific treatments detailed in the claims.
- Authorization to Release Information: This document allows the release of medical and insurance information relevant to the patient's claim, ensuring compliance with privacy regulations.
- Assignment of Benefits Form: This directs the insurance payment to the dentist, relieving the patient of the immediate financial burden associated with dental services.
- Proof of Coverage: This document verifies the patient's current dental insurance coverage and helps determine eligibility for benefits regarding the submitted claim.
Having these forms and documents ready can streamline the claims process, reducing delays and ensuring efficient reimbursement for dental services rendered. Proper documentation is essential for a smooth experience when requesting dental benefits.
Similar forms
- Insurance Claim Form: Similar in purpose, both forms are used to request reimbursement for medical or dental services. They typically require patient and provider information, as well as details about services rendered.
- Pre-Treatment Estimate Form: Both documents require similar details, including proposed treatments and associated costs. Patients must frequently submit this form to obtain approval before services.
- Patient Registration Form: This document collects patient information such as demographics and insurance details, reflecting a focus on establishing identity and coverage, similar to the data needed for the CSA Dental form.
- Coordination of Benefits Form: This form facilitates sharing of information between multiple insurance plans. Like the CSA Dental form, it aims to clarify which insurer will cover specific medical or dental expenses.
- Authorization for Release of Information: Both forms require consent for sharing personal health information with insurers or other entities, ensuring that necessary medical details can be exchanged for processing claims.
- Beneficiary Designation Form: Designed to outline coverage and benefits, this form may detail who should receive specific benefits, paralleling the CSA Dental form’s need to clarify member and dependent information.
- Provider Agreement Form: This document serves to establish a formal relationship between a provider and an insurance company, similar to how the CSA Dental form seeks to connect members with their dental care providers.
Dos and Don'ts
Here are eight important guidelines to follow when filling out the CSA Dental Form. Adhering to these will help avoid delays and ensure proper processing of your claim.
- Do provide complete and accurate personal information. Make sure all names, dates of birth, and social security numbers are correct.
- Do check that you have included all necessary documentation. Ensure that any required X-rays and charts are attached to avoid processing delays.
- Do verify your member status. Clearly indicate whether you are a member, spouse, or dependent.
- Do sign and date all required authorization sections. Failure to do this may result in denial of your claim.
- Don’t omit any critical information. Missing details can lead to your claim being returned for corrections.
- Don’t leave any sections blank that are marked as required. All fields must be completed to avoid a processing setback.
- Don’t use unclear abbreviations or shorthand. Clear and concise language is essential for accurate processing.
- Don’t forget to keep a copy of the completed form. Having this may assist in case of any disputes or further inquiries.
Thoroughness and accuracy matter significantly when submitting your CSA Dental Form. Follow these guidelines to facilitate a smoother claims process.
Misconceptions
Misconceptions about the CSA Dental Claim Form:
- The form is only for retired members. Many people believe that only retirees can use this form. In fact, it is available for both active members and their dependents.
- X-rays are optional for all claims. Some individuals think they can submit a claim without x-rays. However, x-rays are mandatory for certain procedures, such as inlays and crowns.
- Only one claim can be submitted at a time. This is not true. Multiple claims can be submitted together, as long as each is properly filled out.
- Missing teeth don’t need to be marked. Marking missing teeth with an "X" is crucial as it provides important information regarding the dental treatment needed.
- All claims are processed quickly. Processing times can vary. Delays often occur due to incomplete information or missing documentation.
- Only the patient can sign for the claim. If the patient is a minor, a parent or guardian may sign on their behalf, which is often misunderstood.
- Pre-treatment estimates are unnecessary. Some believe pre-treatment estimates are optional. In reality, they are required for certain types of dental work.
- Claim forms can be submitted without prior approval. Misunderstanding exists about needing pre-approval for certain treatments, which is often necessary.
- All dental services are covered under the form. Coverage may vary by plan. It’s essential to check and confirm and consult the specific coverage details.
- Submitting the claim form online is not possible. Many think that they must submit a paper form. However, electronic submission is often available through certain platforms.
Key takeaways
Filling out the CSA Dental form accurately is essential for a smooth claims process. Here are some key takeaways:
- Complete All Required Information: Make sure to fill out all sections that apply to you, including patient information, member information, and dentist information.
- Include Necessary Documentation: Submit any required x-rays or additional documents. Without these, your claim may be delayed or denied.
- Check Your Coverage: Clearly indicate whether you have other dental coverage. This ensures you receive the correct benefits.
- Sign the Authorization: Both you and your dentist must sign the authorization sections to validate the claim. Claims submitted without proper signatures will not be processed.
Following these guidelines can help you avoid common mistakes and facilitate quicker processing of your dental claim.
Browse Other Templates
Gamestop Application Pdf - Attachment of additional sheets can provide more details if needed.
Where Does Workers Comp Money Come From - Enter complete employee information, including name and date of injury.