Fill Out Your Da 4036 Form
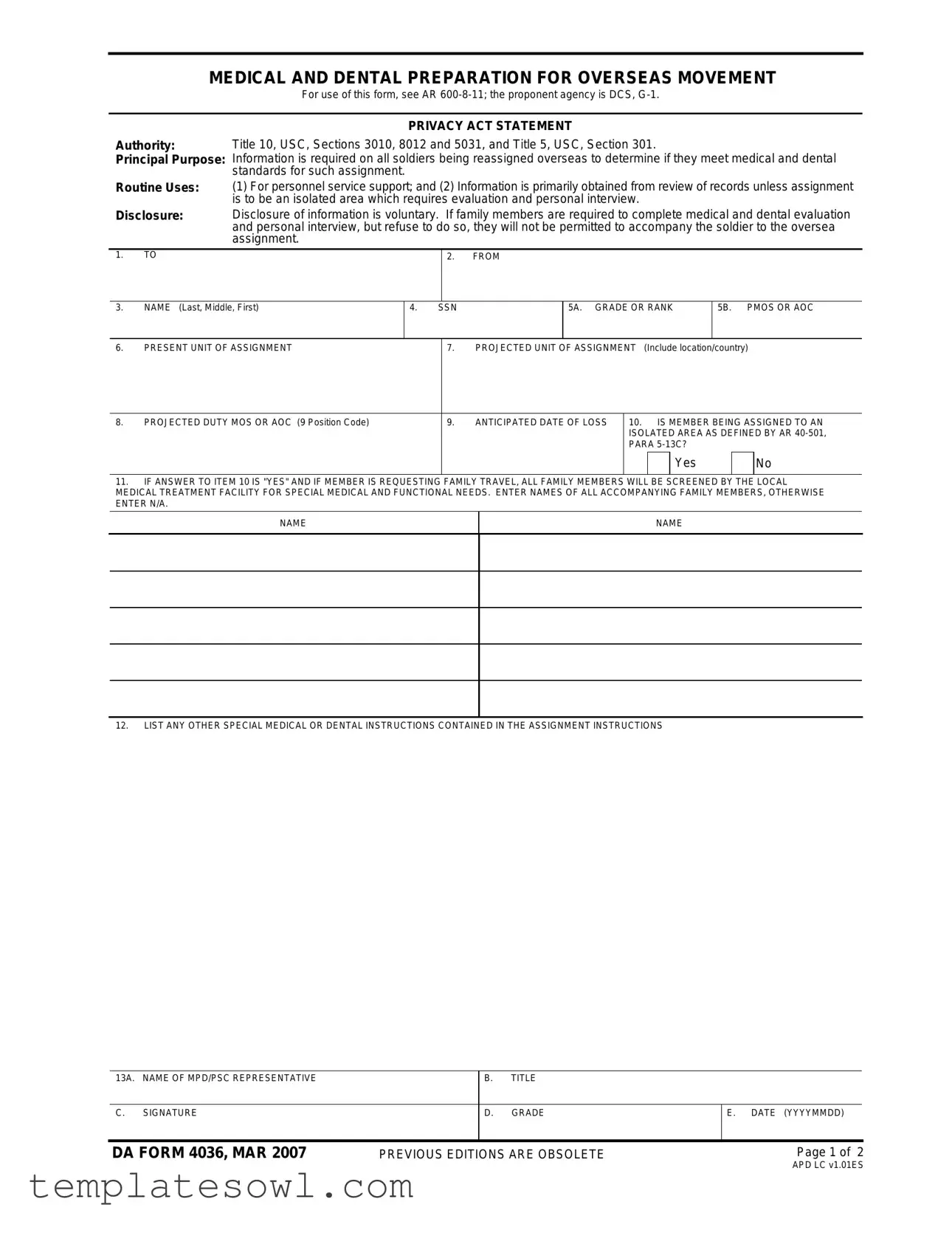
The DA 4036 form, officially titled "Medical and Dental Preparation for Overseas Movement," is crucial for soldiers being reassigned overseas. It helps determine if they and their family members meet the necessary medical and dental standards for their upcoming assignments. Information collected on this form is vital for personnel service support and primarily comes from existing medical records. However, if the assignment involves an isolated area, the form requires additional evaluations and personal interviews. The DA 4036 also emphasizes the importance of family members completing their medical assessments; those who refuse will not be able to accompany the soldier. Key sections of the form collect personal details such as the soldier's name, rank, unit assignment, anticipated date of loss, and any special medical instructions related to the assignment. Medical and dental statuses are also reviewed, ensuring that any limitations or required treatments are documented. Thus, proper completion and timely submission of the DA 4036 form are essential steps in ensuring a successful overseas deployment for soldiers and their families.
Da 4036 Example
MEDICAL AND DENTAL PREPARATION FOR OVERSEAS MOVEMENT
For use of this form, see AR
Authority: Principal Purpose:
Routine Uses:
PRIVACY ACT STATEMENT
Title 10, USC, Sections 3010, 8012 and 5031, and Title 5, USC, Section 301.
Information is required on all soldiers being reassigned overseas to determine if they meet medical and dental standards for such assignment.
(1)For personnel service support; and (2) Information is primarily obtained from review of records unless assignment is to be an isolated area which requires evaluation and personal interview.
Disclosure: Disclosure of information is voluntary. If family members are required to complete medical and dental evaluation and personal interview, but refuse to do so, they will not be permitted to accompany the soldier to the oversea assignment.
1.TO
2.FROM
3.NAME (Last, Middle, First)
4.SSN
5A. GRADE OR RANK
5B. PMOS OR AOC
6. |
PRESENT UNIT OF ASSIGNMENT |
7. |
PROJECTED UNIT OF ASSIGNMENT (Include location/country) |
8. |
PROJECTED DUTY MOS OR AOC (9 Position Code) |
9. |
ANTICIPATED DATE OF LOSS |
10. IS MEMBER BEING ASSIGNED TO AN |
||||
|
|
|
|
ISOLATED AREA AS DEFINED BY AR |
||||
|
|
|
|
PARA |
|
|
||
|
|
|
|
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
11.IF ANSWER TO ITEM 10 IS "YES" AND IF MEMBER IS REQUESTING FAMILY TRAVEL, ALL FAMILY MEMBERS WILL BE SCREENED BY THE LOCAL MEDICAL TREATMENT FACILITY FOR SPECIAL MEDICAL AND FUNCTIONAL NEEDS. ENTER NAMES OF ALL ACCOMPANYING FAMILY MEMBERS, OTHERWISE ENTER N/A.
NAME
NAME
12.LIST ANY OTHER SPECIAL MEDICAL OR DENTAL INSTRUCTIONS CONTAINED IN THE ASSIGNMENT INSTRUCTIONS
13A. NAME OF MPD/PSC REPRESENTATIVE |
|
B. |
TITLE |
|
|
|
|
|
|
|
|
C. SIGNATURE |
|
D. |
GRADE |
E. DATE (YYYYMMDD) |
|
|
|
|
|
|
|
DA FORM 4036, MAR 2007 |
PREVIOUS EDITIONS ARE OBSOLETE |
Page 1 of 2 |
|||
APD LC v1.01ES
Complete the medical and dental status portions below, return the original and one copy to the MDP/PSC within 21 calendar days of the date shown in item 13E, and forward one copy to the address in item 6.
MEDICAL STATUS
14A. PHYSICAL PROFILE SERIAL CODE |
B. PHYSICAL CATEGORY CODE |
|
C. |
MEDICAL RECORDS REVEAL THE FOLLOWING ASSIGNMENT |
||||||||||||
|
|
(PULHES) |
|
|
|
|
|
|
|
|
LIMITATIONS |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
YES |
|
NO |
|
N/A |
|
|
|
|
|
ITEM |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
15A. |
Does the member meet the medical fitness |
|
B. IF CONDITION IS TEMPORARY, EXPECTED DATE |
||||||
|
|
|
|
|
|
|
standards outlined in AR |
MEMBER WILL BE ELIGIBLE FOR ASSIGNMENT |
||||||||
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16A. |
Has member completed HIV screening? |
|
B. |
DATE, TIME AND LOCATION OF APPOINTMENT |
|||||
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17A. |
Is the member pregnant? |
|
|
|
B. |
IF "YES", EXPECTED DATE OF DELIVERY |
|||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
18A. |
All active duty and reserve personnel of PCS |
B. IF "YES", INDICATE DATE, TIME, AND LOCATION OF |
|||||||
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
assignment to Korea will be vaccinated with hepatitis |
|
APPOINTMENT |
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
B vaccine. Does the member require immunization? |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. |
IF "YES", INDICATE DATE, TIME, AND LOCATION OF |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
19A. |
Does the member require remedial medical care? |
APPOINTMENT |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
20A. |
Is the member currently undergoing alcohol or |
B. IF "YES", INDICATE DATE THE MEMBER ENTERED |
|||||||
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
drug abuse rehabilitation? |
|
|
|
THE REHABILITATION PROGRAM |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
21A. |
If item 10 is checked "yes", can the member be |
B. IF "YES", THE MEMBER (and family members, if |
|||||||
|
|
|
|
|
|
|
assigned to an area where medical facilities are limited or |
applicable) MUST BE SCHEDULED FOR A |
||||||||
|
|
|
|
|
|
|
EVALUATION OF MEDICAL STATUS WITHIN 30 CALENDAR |
|||||||||
|
|
|
|
|
|
|
nonexistent? |
|
|
|
|
DAYS OF THE ANTICIPATED DATE OF LOSS (Item 9). |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INDICATE DATE, TIME AND LOCATION OF APPOINTMENT(S) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||||||
22. |
Medical Records Indicate the Member Requires the Following |
(Check those appropriate) |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||
REQUIRES |
|
HAS |
MISSING |
|
ITEM |
|
|
DATE, TIME AND LOCATION OF APPOINTMENT, IF NEEDED |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
Two pairs of spectacles |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. |
Protective mask spectacle |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
insert |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C. |
Two hearing aids |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D. |
Medical warning tag |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
23A. |
NAME OF MEDICAL OFFICER |
|
|
|
B. |
TITLE |
|
|
||||||||
C.SIGNATURE
D.GRADE
E. DATE (YYYYMMDD)
DENTAL STATUS (Complete only if Item 10 is checked "Yes" or if required by item 12.)
|
YES |
|
|
NO |
|
|
B. |
IF "NO", BRIEFLY EXPLAIN. IF CONDITION IS TEMPORARY, EXPECTED |
|
|||
|
|
|
|
|
||||||||
|
|
|
24A. |
Is the member dentally qualified? |
DATE THE MEMBER WILL BE ELIGIBLE FOR ASSIGNMENT |
|||||||
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
25A. |
Does the member require remedial dental |
B. IF "YES", INDICATE DATE, TIME, AND LOCATION OF APPOINTMENT |
|||
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
care? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
26A. |
If item 10 is checked "yes", can the member |
B. IF "YES", THE MEMBER (and family members, if applicable) MUST BE |
|||
|
|
|
|
|
|
|
be assigned to an area where dental facilities are |
SCHEDULED FOR A |
||||
|
|
|
|
|
|
|
30 CALENDAR DAYS OF THE ANTICIPATED DATE OF LOSS (Item 9). INDICATE |
|||||
|
|
|
|
|
|
|
limited or nonexistent? |
DATE, TIME, AND LOCATION OF APPOINTMENT(S) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
27A. NAME OF DENTAL OFFICER |
B. |
TITLE |
|
|
|||||||
|
|
|
|
|
|
|
|
|||||
|
C. |
SIGNATURE |
|
D. |
GRADE |
E. DATE (YYYYMMDD) |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
DA FORM 4036, MAR 2007 |
|
|
Page 2 of 2 |
|||||||||
APD LC v1.01ES
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Purpose | The DA 4036 form is utilized to assess the medical and dental readiness of military personnel assigned for overseas movement. |
| Governing Law | This form follows guidelines outlined in Army Regulation (AR) 600-8-11 and AR 40-501. |
| Mandatory Information | All soldiers being reassigned overseas must provide information required to determine compliance with medical and dental standards. |
| Disclosure Policy | Disclosure of the required information is voluntary. Non-compliance by family members may restrict their travel with the soldier. |
| Filling Timeline | The completed form must be submitted within 21 calendar days from the date indicated on the form. |
| Privacy Act Statement | The form is governed by the Privacy Act, ensuring that personal information is managed appropriately. |
| Screening for Isolated Areas | If assigned to isolated areas, all accompanying family members undergo screening for special medical and functional needs. |
| Medical Record Review | The majority of information is gathered from existing medical records unless specific evaluations are required. |
| Last Update | The DA Form 4036 was last updated in March 2007, and previous editions should not be used. |
Guidelines on Utilizing Da 4036
The DA 4036 form is essential for soldiers being reassigned overseas, focusing on their medical and dental preparations. Below are the steps to fill out this form accurately, ensuring compliance with military standards and requirements.
- In the top section, fill in the information from "TO" and "FROM" including the appropriate unit information.
- Provide your full name in the "NAME" section, using last, middle, and first name formats.
- Enter your Social Security Number (SSN) in the designated field.
- For "GRADE OR RANK," specify your current military grade or rank.
- Indicate your Primary Military Occupational Specialty (PMOS) or Area of Concentration (AOC).
- State your present unit of assignment and the projected unit of assignment, including the location or country.
- Fill out the projected duty MOS or AOC and include the position code.
- Indicate the anticipated date of loss.
- Answer whether you are being assigned to an isolated area by selecting “Yes” or “No.”
- If you selected “Yes” for the previous question, list the names of all accompanying family members or note "N/A" if not applicable.
- Document any special medical or dental instructions as outlined in the assignment instructions.
- Complete the details of the MPD/PSC representative, including name, title, signature, grade, and date in the appropriate fields.
- Next, complete the medical status section, starting with the physical profile serial code and physical category code.
- Indicate whether medical records reveal specific assignment limitations. Answer the questions related to medical fitness and HIV screening as applicable.
- If pregnant, provide the expected date of delivery; likewise, answer the immunization questions accurately.
- Document any remedial medical care requirements and issues related to alcohol or drug rehabilitation.
- Fill out the details regarding dental status only if the isolated area question was answered “Yes” or if specified in the instructions.
- Conclude with the required endorsements from medical and dental officers by filling in their names, titles, signatures, grades, and dates.
Upon completion, submit the original form and one copy to the appropriate MPD/PSC within 21 calendar days. Forward an additional copy to the address indicated in item 6. Ensure accuracy to prevent potential delays in your overseas assignment.
What You Should Know About This Form
What is the purpose of the DA 4036 form?
The DA 4036 form is used to ensure that soldiers are medically and dentally fit for overseas assignments. It gathers information from soldiers being reassigned, helping to determine whether they meet the appropriate standards required for deployment. This includes evaluating any special medical or dental needs that may affect their ability to serve in isolated areas or countries.
Who needs to complete the DA 4036 form?
All soldiers who are being reassigned overseas must complete the DA 4036 form. Additionally, if family members are accompanying the soldier, they will also need to undergo medical and dental evaluations. Failure to complete these evaluations may prevent families from traveling with the soldier.
What happens if information is missing or if a soldier does not meet medical standards?
It is essential that the DA 4036 form is completed thoroughly and accurately. If there are missing pieces of information or if a soldier does not meet medical standards, it may delay or prevent deployment. Soldiers are advised to provide any necessary documentation or to explain any temporary conditions on the form to clarify their medical status.
Are there any consequences for not disclosing medical conditions?
Yes, it is crucial to disclose all relevant medical conditions. Failing to do so can result in serious consequences, including the possibility of being deemed unfit for the assigned military duties. Furthermore, if family members decline to complete their necessary evaluations, they may be prohibited from accompanying the soldier to their overseas assignment.
Common mistakes
When filling out the DA 4036 form, individuals often overlook critical sections which can lead to complications in their overseas assignments. One common mistake is failing to provide accurate personal information, such as their full legal name or Social Security Number (SSN). Omitting or incorrectly entering these details can delay processing times and create issues with identification during the transition.
Another frequent error is neglecting to check the status of family members when applicable. If the soldier is requesting family travel, all accompanying family members must be screened for medical and functional needs. Some applicants mistakenly leave this section blank or enter "N/A" without ensuring all necessary family member evaluations have been conducted. Such oversights can hinder family members from accompanying the soldier.
Many individuals also make the mistake of inaccurately reporting their medical status. When asked if they meet medical fitness standards, some may inadvertently indicate "yes" without considering their complete health history. It is important to provide truthful responses. Any discrepancies can result in the soldier being found unfit for duty after reaching their assignment.
Completing the dental status section is equally vital and often mishandled. Individuals may skip this part altogether if it is not deemed necessary during their assessment. However, if the member is being assigned to an area with limited dental facilities, this information must be duly filled out. Neglecting this could lead to severe consequences if dental issues arise while stationed abroad.
Properly scheduling follow-up evaluations is another crucial aspect that can be easily overlooked. The form specifies that those assigned to isolated areas where medical facilities are limited must receive follow-up evaluations. Failure to indicate these appointments clearly can result in gaps in healthcare support, ultimately jeopardizing the health of soldiers and their families.
Lastly, many overlook the importance of signatures and dates throughout the form. Each section requiring a signature or date must be completed correctly, as missing this information can render the form incomplete. Ensuring that everything is properly signed and dated is essential for maintaining compliance with military documentation protocols.
Documents used along the form
The DA Form 4036 is an essential document used to evaluate medical and dental preparedness for military personnel being assigned overseas. To ensure a smooth transition, several other forms and documents often accompany it during the reassignment process. Below is a list of these commonly used documents, each serving a specific purpose.
- DA Form 2408-14: This form, known as the Equipment Control Record, is used to document maintenance and status updates on equipment assigned to military personnel. It ensures that all necessary gear is accounted for and ready for overseas movement.
- DA Form 5500: The Body Fat Content Worksheet helps assess whether a service member meets the Army's body composition standards. It becomes especially important for overseas assignments where physical fitness is a priority.
- DA Form 3349: The Physical Profile form outlines any medical restrictions a soldier may have. This document is critical for determining the soldier’s suitability for specific duties in a new geographic location.
- DA Form 7822: The Active Duty Service Member's Review Certificate compiles a member's service data, including deployments and assignments. This document helps review a member’s history to ensure they are cleared for the new assignment.
- SF 600: The Chronological Record of Medical Care captures a soldier's medical history and ongoing health issues. It provides a comprehensive overview for medical personnel at the new duty station.
- DA Form 4856: The Developmental Counseling Form outlines counseling sessions to address performance or behavioral issues. It helps document past concerns and ensures that these are taken into account in the new assignment.
- DA Form 2028: The Recommended Changes to Publications form is used to suggest changes to Army manuals and other publications. It ensures that personnel have the most up-to-date resources while overseas.
Completing the DA Form 4036 along with these documents is crucial for a successful transition. Each form serves to confirm that the soldier is medically and administratively prepared to take on new challenges in their overseas assignment.
Similar forms
- DA Form 7349: This form, known as the Medical and Dental Clearance for Deployment, is utilized to assess the medical fitness of service members prior to deployment. Like DA 4036, it ensures that personnel meet necessary health standards required for overseas assignments.
- DA Form 5888: The Family Member Deployment Screening Form collects information about family members’ health to determine their eligibility to accompany the service member. It shares the purpose of assessing whether family members meet specific medical requirements for overseas movement.
- DA Form 8003: The Medical and Dental Readiness Report serves to evaluate the medical readiness of soldiers. Similar to the DA 4036, it focuses on documenting medical conditions that could impact assignment readiness.
- SF 600: The Chronological Record of Medical Care logs individual patient visits and treatments. It parallels DA 4036’s aim of collecting and reviewing medical data crucial for determining fitness for overseas assignment.
- DA Form 3349: The Release from Active Duty (RA) Physical Profiling form outlines a soldier's physical limitations and capabilities. This aligns with DA 4036’s assessment of a member's medical standards before overseas deployment.
- DA Form 705: The Army Physical Fitness Test Scorecard tracks physical fitness testing results. It complements the DA 4036, as physical fitness is a critical component of medical readiness for overseas assignments.
- DD Form 2766: The Adult Preventive and Chronic Care Flowsheet includes health history and preventive care measures. Like the DA 4036, it focuses on ensuring that all medical evaluations are recorded accurately to support safe overseas movement.
Dos and Don'ts
When filling out the DA Form 4036, it is essential to take certain actions and avoid others to ensure accuracy and compliance. Below is a list detailing what you should and shouldn't do.
- Do carefully read the entire form before beginning.
- Do provide accurate and complete information for all sections.
- Do adhere to the submission deadline of 21 calendar days.
- Do confirm that all medical and dental evaluations are up to date.
- Do consult with a medical or personnel officer if you have questions.
- Don't leave any mandatory fields blank; fill in all required information.
- Don't submit the form without a thorough review for errors or omissions.
- Don't ignore specific instructions related to isolated area assignments.
- Don't falsify any information; this can lead to serious consequences.
- Don't forget to retain a copy for your personal records.
Misconceptions
Here are seven common misconceptions about the DA 4036 form, which is related to medical and dental preparation for overseas movement.
- Only active-duty soldiers need to fill out the form. This is incorrect. Reserve personnel also need to complete the DA 4036 form if they are being reassigned overseas.
- The form is optional and can be ignored. In reality, the DA 4036 form is mandatory for soldiers who are moving overseas. It determines their medical and dental eligibility.
- Medical evaluations are only required for the soldiers. This is misleading. Family members must also undergo medical evaluation if they accompany the soldier. Without it, they cannot go along.
- The form is only for isolated duty assignments. While it is critical for isolated areas, it is also necessary for any overseas assignments to determine overall medical fitness.
- Submissions of the form are not time-sensitive. This is false. Soldiers must return the completed DA 4036 form within 21 calendar days from a specified date.
- HIV screening is optional. On the contrary, all members being assigned to certain locations, like Korea, are required to complete HIV screening.
- Only doctors need to complete portions of the form. This is not true. Soldiers themselves must provide essential medical information as well, in addition to their healthcare providers filling out relevant sections.
Understanding these misconceptions can help ensure compliance and a smooth transition for soldiers and their families moving overseas.
Key takeaways
Filling out the DA 4036 form is crucial for soldiers being reassigned overseas, particularly to ensure they meet specific medical and dental standards. Here are some key takeaways to keep in mind when working with this form.
- Understand the Purpose: The DA 4036 form is used to assess the medical and dental readiness of military personnel for overseas assignments.
- Timeliness is Key: Submit the completed form along with supporting documents to the appropriate Personnel Support Center (PSC) within 21 calendar days.
- Information is Mandatory: Comprehensive details about the soldier’s medical history and status are required, as this affects their capability for overseas deployment.
- Isolation Area Considerations: If assigned to an isolated area, family members must undergo screening by local medical treatment facilities.
- Clarify Special Needs: Clearly list any special medical or dental instructions as they relate to the soldier’s overseas assignment.
- Follow-Up Appointments: Ensure to document follow-up evaluations for any medical or dental concerns identified during the review.
- Privacy Matters: Be aware that while providing your information is voluntary, refusal can impact a soldier's ability to take family members abroad.
Completing the DA 4036 form accurately can make a significant difference in ensuring that soldiers are fully prepared for overseas assignments. This readiness not only affects the individual soldier but also their family and unit. A thorough understanding of this form helps in smooth transitions and operational effectiveness.
Browse Other Templates
Uc-44fr - Participation in the public comment period is a vital step in the rulemaking process.
When a Veteran Dies Who Gets the Flag - This application helps honor veterans’ service by obtaining a flag for burial purposes.
Cg719s - Using the CG-719S can help in advancing one's maritime career by providing essential documentation.