Fill Out Your Dads 3647 Form
The DADS 3647 form, also known as the Assisted Living Disclosure Statement, is an essential tool for individuals and families considering assisted living options in Texas. This form outlines a facility's services and policies in a standardized format, allowing for easy comparison across different locations. It includes crucial information about the facility's admission and discharge processes, available services, and amenities included in the base rate. Additionally, the form reveals details about pre-admission evaluations, communication provisions for residents with special needs, and how ongoing care is planned and administered. It emphasizes transparency and ensures that prospective residents are informed about their options. Importantly, while the DADS 3647 form provides valuable information, it does not replace the necessity of visiting the facility, interacting with staff, and speaking with current residents. Each facility's unique offerings will be defined, but it’s essential to understand that the form is not a guarantee of services provided. Instead, it serves as a guideline to foster informed decision-making for individuals seeking support in assisted living environments.
Dads 3647 Example
Texas Department of Aging |
Form 3647 |
and Disability Services |
July |
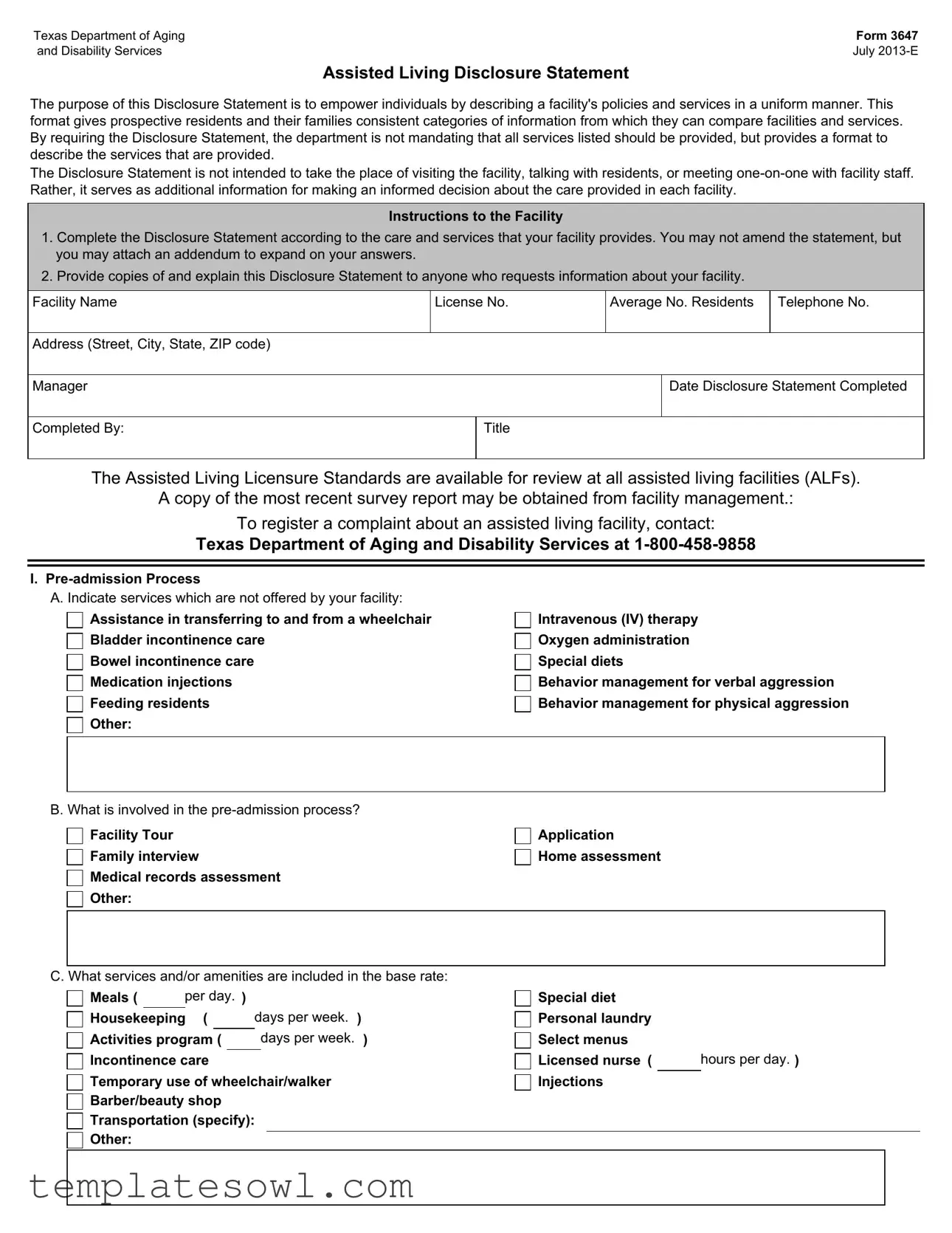
Assisted Living Disclosure Statement
The purpose of this Disclosure Statement is to empower individuals by describing a facility's policies and services in a uniform manner. This format gives prospective residents and their families consistent categories of information from which they can compare facilities and services. By requiring the Disclosure Statement, the department is not mandating that all services listed should be provided, but provides a format to describe the services that are provided.
The Disclosure Statement is not intended to take the place of visiting the facility, talking with residents, or meeting
Instructions to the Facility
1.Complete the Disclosure Statement according to the care and services that your facility provides. You may not amend the statement, but you may attach an addendum to expand on your answers.
2.Provide copies of and explain this Disclosure Statement to anyone who requests information about your facility.
Facility Name
License No.
Average No. Residents
Telephone No.
Address (Street, City, State, ZIP code)
Manager
Date Disclosure Statement Completed
Completed By:
Title
The Assisted Living Licensure Standards are available for review at all assisted living facilities (ALFs).
A copy of the most recent survey report may be obtained from facility management.:
To register a complaint about an assisted living facility, contact:
Texas Department of Aging and Disability Services at
I.
A. Indicate services which are not offered by your facility:
Assistance in transferring to and from a wheelchair Bladder incontinence care
Bowel incontinence care
Medication injections
Feeding residents
Other:
Intravenous (IV) therapy
Oxygen administration
Special diets
Behavior management for verbal aggression Behavior management for physical aggression
B. What is involved in the
Facility Tour
Family interview
Medical records assessment
Other:
Application Home assessment
C. What services and/or amenities are included in the base rate:
Meals ( |
|
per day. ) |
|
|
||
Housekeeping ( |
|
days per week. ) |
||||
Activities program ( |
|
|
days per week. ) |
|||
Incontinence care
Temporary use of wheelchair/walker
Barber/beauty shop
Transportation (specify):
Other:
Special diet Personal laundry Select menus
Licensed nurse ( hours per day. )
Injections
D. What additional services can be purchased?
Beauty/barber services
Incontinence care
Incontinence products
Injections
Other:
Form 3647
Page 2 /
Companion
Transportation to doctor visits
Minor nursing services provided by facility staff Home health services
E. Do you charge more for different levels of care? |
Yes |
No |
||
II. Admission Process |
|
|
||
A. Does the facility have a written contract for services? |
Yes |
No |
||
B. Is there a deposit in addition to rent? |
Yes |
No |
||
If yes, is it refundable? |
Yes |
No |
||
If yes, when? |
|
|
||
|
|
|
|
|
C. Do you have a refund policy if the resident does not remain for the entire prepaid period? |
Yes |
No |
||
If yes, explain? |
|
|
||
|
|
|
|
|
D. What is the admission process for new residents? |
|
|
||
Doctors' orders
Other:
Residency agreement
History and physical
Deposit/payment
E. Does the facility have provisions for special resident communication needs?
Staff who can sign for the deaf
Other:
Services for persons who are blind
F. Is there a trial period for new residents? |
Yes |
No |
|
If yes, how long? |
|
|
|
|
|
|
|
III.Discharge/Transfer
A. What could cause temporary transfer from specialized care?
Medical condition requiring
Drug stabilization
Other:
Unacceptable physical or verbal behavior
Resident requires services the facility does not provide
B. The need for the following services could cause permanent discharge:
Assistance in transferring to and from wheelchair Behavior management for verbal aggression Behavior management for physical aggression Other:
Sitters
Bowel incontinence care Bladder incontinence care Intravenous (IV) therapy
Medication Injections Feeding by staff Oxygen administration Special diets
C. Who would make this discharge decision?
Facility manager
Other:
D. Do families have input into these discharge decisions?...................................................................
E. Is there an avenue to appeal these decisions?..............................................................................
F. Do you assist families in making discharge plans? .........................................................................
Yes
Yes
Yes
No
No
No
Form 3647
Page 3 /
IV. Planning and Implementation of Care (check all that apply)
A. Who is involved in the service plan process?
Resident |
Family member |
Licensed nurses |
Social worker |
Other: |
|
Activity director Dietary
Attendants Physician
Manager
B. Does the service plan address the following?
Medical needs
Nursing needs
Activities of daily living
Psychosocial status
Nutritional status
Dental Services
Other:
C. How often is the service plan assessed?
Monthly
Other:
Quarterly
Annually
As Needed
D. How many hours of structured activities are scheduled per day?
E. What types of programs are scheduled?
8+ Hours
Music program
Other:
Arts program
Crafts
Exercise
Cooking
F. Who assists/administers medications?
RN
Other:
V. Aging in Place
LVN
Medication aide
Attendant
Department of Aging and Disability Services (DADS) Rules
An inappropriately placed resident is a resident who was appropriate when admitted to the ALF, but whose condition has changed. All residents must be appropriate for the ALF licensure type when admitted to the facility. After admission, if the resident's condition changes, the resident may no longer be appropriate for the facility's license. An ALF is not required to keep a resident who is no longer appropriate for the facility's license.
An inappropriately placed resident may be identified by the ALF or by DADS.
There are two situations which a resident may be determined to be inappropriate:
•Resident experiences a change in condition, needs additional services and meets evacuation criteria.
•Resident experiences a change in condition and does not meet evacuation criteria.
What are the ALF's policies and procedures for aging in place?
Resident experiences a change in condition and meets evacuation criteria. Documentation is submitted to DADS. Resident experiences a change in condition and does not meet evacuation criteria. Waiver request submitted to DADS. No documentation submitted to DADS. Resident is discharged.
An ALF is not required to keep a resident who is no longer appropriate for the facility’s license. A facility will determine its ability to accommodate a resident and decide if it will apply for a waiver request on a case by case basis. DADS rules about inappropriately placed residents may be found in the Licensing Standards for Assisted Living Facilities at 40 Texas Administrative Code Chapter 92, Subchapter 92.41
(f). The following link will direct you to the Licensing Standards for Assisted Living Facilities:
VI. Change In Condition Issues
What special provisions do you allow aging in place?
Sitters
Other:
VII. Staff Training
Additional services agreements
Hospice
Home health
Yes 
 No
No
A. What training do new employees receive?
Orientation: hours
Other:
Review of resident service plan
|
hours |
|
|
|
|
|
|
|
Form 3647 |
||
|
|
|
Page 4 / |
||
B. Is staff trained in CPR? |
Yes |
No |
|||
|
If no, please explain why you do not require CPR training: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C. How much ongoing training is provided and how often? (Example: 30 minutes monthly): |
|
|
|
|
|
D. Who gives the training and what are their qualifications? |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
E. What type of training do volunteers receive? |
|
|
|
|
|
Orientation: hours
Other:
F. In what type of endeavors are volunteers engaged?
Activities |
Meals |
Religious services |
Other:
Entertainment
Visitation
G. List volunteer groups involved with the family?
VIII. Physical Environment
A. What safety features are provided in your building?
Emergency call systems
Sprinkler system
Fire alarm system
Other:
Wander Guard or similar system
Built according to NFPA Life Safety Code, Chapter 12, Health Care
Built according to NFPA Life Safety Code, Chapter 21, Board and Care
B. Does the facility's environment include the following?
Plants
Other:
Pets
Vegetable/flower gardens for use by residents
C. Are the residents allowed to have:
Plant's |
Pets |
IX. Staffing Patterns
A. What are the qualifications of the manager?
No
Yes How much? .......
B. Please list the facility's normal
1.the attached chart; or
2.a separate attachment which explains your facility's unique staffing policies and patterns.
|
|
|
Form 3647 |
|
|
|
|
Page 5 / |
|
X. Residents's Rights |
|
|
|
|
A. Do you have a Resident's Council? |
Yes |
No |
||
How often does it meet? |
|
|
|
|
|
|
|
|
|
B. Do you have a Family Council? |
Yes |
No |
||
How often does it meet? |
|
|
|
|
|
|
|
|
|
C. Does the facility have a formal procedure for responding to resident grievances and suggestions for improvement?
Is there a Grievance Committee? ...................................................................................................
Is there a suggestion box? ............................................................................................................
D. How can the company that owns the facility be contacted?
Yes
Yes Yes
No
No No
Shift Times and Staffing Patterns at the Facility
Shifts |
|
|
|
Number of Staff Per Shift |
|
|||
(Enter the hours of |
|
|
|
|
|
|
|
|
R.N.s |
L.V.N.s |
Attendants |
Medication Aides |
Activity Workers |
Universal Workers |
Other Workers |
||
each of your facility's shifts.) |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Shifts |
|
|
|
Number of Staff Per Shift |
|
|||
(Enter the hours of |
|
|
|
|
|
|
|
|
R.N.s |
L.V.N.s |
Attendants |
Medication Aides |
Activity Workers |
Universal Workers |
Other Workers |
||
each of your facility's shifts.) |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose of Disclosure Statement | This statement helps individuals understand a facility's services and policies, allowing for easier comparison between different assisted living options. |
| Licensing Authority | The Texas Department of Aging and Disability Services (DADS) governs the regulations pertaining to assisted living facilities in Texas. |
| Pre-Admission Process | Facilities must outline their pre-admission processes, which may include tours, medical assessments, and family interviews. |
| Service Fees | Residents can expect to see service fees listed for provided amenities, such as meals, housekeeping, and nursing care. |
| Admission Contracts | Many facilities utilize written contracts that detail the services offered, which prospective residents must review before admission. |
| Discharge Policy | Facilities must explain their discharge policies, including potential reasons for discharge and whether families have a say in these decisions. |
| Aging in Place | The form addresses how facilities can accommodate residents whose needs change over time, including processes for documenting changes to care requirements. |
| Staff Training | Ongoing training is mandatory for staff, encompassing areas such as CPR and special resident needs, contributing to a higher standard of care. |
| Safety Features | Facilities must implement safety features such as fire alarm systems and emergency call systems to safeguard residents effectively. |
| Residents' Rights | The form emphasizes the importance of residents' rights, including their ability to participate in councils and provide feedback on facility services. |
Guidelines on Utilizing Dads 3647
Completing the Dads 3647 form requires attention to detail to ensure that all information reflects the services and policies of the facility accurately. This process enables prospective residents and their families to make well-informed decisions regarding care options. Following the steps outlined below will assist you in successfully filling out the form.
- Begin with the Facility Information section. Enter the facility name, license number, average number of residents, telephone number, and address including street, city, state, and ZIP code.
- Fill in the details of the Manager, including their name and title, along with the date the Disclosure Statement was completed.
- Indicate the Pre-admission Process. List any services your facility does not offer in the designated area.
- Describe the steps involved in the pre-admission process, such as facility tours and family interviews.
- Outline the services and amenities that are included in the base rate, such as meals, housekeeping, and licensed nurse availability.
- Specify any additional services that can be purchased by residents, such as beauty services or home health services.
- Answer whether there are different charges for different levels of care, marking “Yes” or “No” as appropriate.
- For the Admission Process, indicate whether the facility has a written contract for services and if any deposit is required.
- Provide details regarding the refund policy, if applicable, along with the admission process steps for new residents.
- Note any special provisions for resident communication needs and whether there is a trial period for new residents.
- In the Discharge/Transfer section, explain what could cause temporary transfers and permanent discharges, alongside who makes those decisions.
- Fill out the section on the Planning and Implementation of Care, detailing the individuals involved in the service plan process and the frequency of service plan assessments.
- Provide required information regarding your facility's staff training, including CPR training and ongoing training frequency.
- Detail the Physical Environment, including safety features in place and any restrictions related to pets or plants in resident living spaces.
- In the section on Residents’ Rights, indicate the existence of a Resident’s Council or Family Council and how grievances are addressed.
- Lastly, record the staffing patterns for both full-time and part-time personnel throughout the facility.
What You Should Know About This Form
What is the purpose of the DADS 3647 form?
The DADS 3647 form serves as an Assisted Living Disclosure Statement designed to empower individuals and families by detailing a facility's policies and available services. It offers a standardized method of presenting information, allowing prospective residents to compare the features of different facilities. Although it outlines expected services, it is essential to understand that the form does not guarantee availability. A personal visit to the facility and discussions with staff and current residents remain vital for understanding the care environment.
How does the pre-admission process work?
The pre-admission process typically involves several steps aimed at ensuring the facility can meet the prospective resident's needs. Most facilities will provide a tour, conduct a family interview, and assess medical records. An application and sometimes a home assessment may also be part of this process. This setup helps ensure that the individual is a good fit for the facility and that the necessary services can be accommodated.
What services and amenities are commonly included in the base rate?
Are there additional services available for purchase?
What happens if a resident's condition changes and they require a higher level of care?
What safety features should I expect in an assisted living facility?
How does the facility handle resident rights and grievances?
Common mistakes
When filling out the DADS 3647 form, some common mistakes can lead to confusion, misinformation, and potentially impact the decision-making process for prospective residents and their families. One major error is failing to accurately represent the services provided by the facility. It is crucial to check the box for each service that does not apply to ensure clarity. A vague or incomplete depiction of services can create false expectations, which might lead to dissatisfaction later on.
Another frequent issue is neglecting to specify additional services that can be purchased. When the form includes options for extra services, it's important to fill these out thoroughly. If prospective residents are unaware of the services that are available for purchase, they may feel unprepared to handle their care needs once they arrive. Therefore, being exhaustive in this section is essential to provide clear, actionable information.
People filling out the form often overlook the significance of the admission process overview. Carefully detailing the steps involved—from written contracts to deposit policies—can make a significant difference in transparency for potential residents. Omitting this information creates misunderstanding and uncertainties for families as they seek to navigate the transition for their loved ones.
Moreover, many individuals fail to include information about discharge processes. This section outlines critical aspects that may affect a resident’s stay. It is important to clarify the conditions under which discharge may occur, who is involved in these decisions, and whether families can participate in discussions about discharges. Lack of specificity in this area can lead to feelings of helplessness among families when unexpected changes occur.
Lastly, another mistake often made involves the staff training section. When detailing ongoing training and qualifications, it is vital to be specific. Generic statements do not convey the level of care and preparedness of staff. Not providing adequate information about training protocols could undermine confidence from families considering the facility for their loved ones. Ensuring each section is thorough will aid significantly in producing a clear and comprehensive information source for prospective residents and their families.
Documents used along the form
The DADS Form 3647 serves a critical function in outlining the policies and services of assisted living facilities in Texas. When considering assisted living options, several other documents can complement this form to provide a more comprehensive understanding of the facility. Below is a list of additional forms and documents that may be relevant.
- Resident Agreement: This contract outlines the terms and conditions of residency within the facility. It typically includes details on costs, services provided, and the rights of residents. Understanding this agreement is essential for clarity on what one can expect during their stay.
- Facility Survey Reports: These reports offer insight into the facility's compliance with state regulations. They highlight past inspections, any deficiencies found, and how they were resolved. Reviewing these documents can reveal a facility’s track record regarding quality and care.
- Admission Packet: Usually provided during the admission process, this packet includes important information, such as medical forms, facility rules, and a list of available services. It serves as a welcome guide for new residents and their families.
- Crisis Plan: This document outlines the procedures and protocols in place for handling emergencies and unexpected incidents within the facility. Important for safety, it helps clarify how the facility addresses various situations, ensuring that residents are protected.
- Care Plans: These individualized plans are developed for each resident, detailing specific care needs and goals. Regular assessments update these plans to reflect any changes in the resident's health or preferences, ensuring personalized care is maintained.
Understanding these documents, along with the DADS Form 3647, assists individuals and families in making informed choices about assisted living facilities. It is advisable to review them carefully to ensure that the selected facility meets specific needs and expectations.
Similar forms
The DADS 3647 form, also known as the Assisted Living Disclosure Statement, provides valuable information about the services and policies of assisted living facilities. Several other documents serve similar purposes, helping individuals and families understand options for care. Below is a list of these documents, along with their functions.
- Resident Service Plan: This document outlines the specific services and support a resident will receive, tailored to their individual needs. Like the DADS 3647, it aims to enhance understanding of care options available within the assisted living environment.
- Informed Consent Form: This form ensures that residents and their families fully comprehend the care being offered. It includes details about treatments and services, similar to how the DADS 3647 provides a comprehensive view of facility offerings.
- Facility Admission Agreement: This contract specifies the terms of residence in a facility, covering costs and services. Just as the DADS 3647 discusses admission policies, this agreement further details a resident's rights and responsibilities.
- Medication Administration Record (MAR): The MAR tracks medications prescribed to residents, ensuring safety in administration. This function aligns with the DADS 3647's attention to medication services and care levels offered by the facility.
- Emergency Plan: This document outlines procedures for emergencies, such as fire or medical situations. The DADS 3647 covers safety features, making the emergency plan an important complementary document for residents.
- Family Council Guidelines: These guidelines help establish a forum where family members can voice concerns and suggestions. This aligns with the discussion in the DADS 3647 about resident rights and family involvement in care.
- Annual Survey Report: Residents or families can request this report to learn about facility inspections and performance. It is similar to the DADS 3647’s provision for transparency regarding facility operations.
- Staff Training Records: These records indicate the qualifications and ongoing training staff receive. Like the DADS 3647, they ensure residents are cared for by trained individuals, reflecting the facility's commitment to quality care.
- Grievance Procedure Document: This document describes the process for residents to file complaints or suggestions. It mirrors the DADS 3647's emphasis on addressing resident concerns and maintaining open lines of communication.
Each of these documents works in conjunction with the DADS 3647 form to provide a holistic understanding of the services, rights, and responsibilities associated with assisted living facilities.
Dos and Don'ts
When filling out the Dads 3647 form, it's essential to pay attention to details and follow best practices. Here’s a straightforward list to keep in mind.
- Double-check all information before submitting the form to avoid errors.
- Provide complete answers to each question to give a comprehensive view of your facility.
- Be honest about the services provided to ensure transparency.
- Attach any necessary addendums for clarification or additional details as needed.
- Keep copies of the completed form for your records.
On the other hand, be careful with the following:
- Don’t omit details that could mislead prospective residents or their families.
- Don’t alter the standard format of the form; stick to the provided structure.
- Avoid using jargon that may confuse readers.
- Don’t forget to update the form whenever there are changes in services or facilities.
- Don’t bypass the family interview as part of the pre-admission process.
By following these dos and don’ts, you can ensure that the Dads 3647 form provides clear and useful information for those considering your facility.
Misconceptions
The DADS Form 3647 serves an important purpose in assisting individuals and families to evaluate assisted living facilities in Texas. However, there are several misconceptions that people often have about this form, which can lead to misunderstandings about its intent and use. Below is a list of common misconceptions, along with clarifications for each.
- All services listed on the form must be offered by the facility. While the DADS Form 3647 requires facilities to disclose information about their services, it does not mandate that they provide all services listed. Facilities may have limitations based on their licensure type.
- The form replaces the need for facility visits. The Disclosure Statement is a helpful tool, but it is not a substitute for visiting the facility, speaking with current residents, or engaging with staff. Firsthand experience is essential for making informed decisions.
- A facility must change its services if they are not listed on the form. The form specifies the services that are provided, but it does not obligate facilities to alter their service offerings. Changes may only occur at the discretion of the facility management.
- The admission process can vary greatly without any oversight. The form encourages facilities to outline their specific admission processes plainly. This ensures a consistent understanding of what families can expect when seeking admission for a resident.
- Discharge policies are uniformly applied across all facilities. Each facility may develop its own discharge policies based on individual circumstances. The format allows for disclosures, but these policies can vary significantly from one facility to another.
- The form provides detailed information about staffing qualifications. The Disclosure Statement may outline the normal staffing patterns within the facility but does not include comprehensive qualifications for individual staff members. Families should inquire directly for specific qualifications.
- Completing the form guarantees better care for residents. Although the form provides standardized information, its completion does not assure that all facilities deliver quality care. Thorough investigation and communication are key factors in this process.
- Facilities must disclose all complaints and grievances received. The form prompts facilities to discuss their procedures for handling grievances, but it does not require them to disclose each complaint or its outcome. Transparency may vary between facilities.
- All facilities have the same minimum standards of care. Facilities can have different licensure types, which may affect the standards of care they provide. The form helps identify these differences, and families should consider each facility's specific licensure status.
- A family must accept the facility's policies as final. While facilities have set policies, there often exists a dialogue with families regarding care and services. Family input is important and can influence care plans and discharge decisions.
Understanding these misconceptions can help families navigate the process of selecting the most appropriate assisted living facility for their loved ones. It is crucial to utilize the DADS Form 3647 as one of many tools in making an informed decision.
Key takeaways
The DADS 3647 form is an essential tool for understanding the services offered by assisted living facilities in Texas. Here are some key takeaways about filling out and using this form:
- Purpose and Structure: The form serves to empower individuals by providing a uniform format to describe a facility’s services and policies, allowing for easier comparisons among facilities.
- Pre-Admission Information: Facilities must indicate which services they do not provide and outline the pre-admission process. This clarity helps potential residents and their families prepare accordingly.
- Admission Details: The form includes critical information about deposits, refund policies, and special provisions, helping families understand the financial and procedural aspects of admission.
- Discharge Protocols: Facilities must specify what circumstances can lead to the discharge or transfer of a resident, as well as the decision-making process involved. This provides families with insight into resident rights and responsibilities.
- Service Plans: The form emphasizes the importance of service plans that address medical needs, daily living activities, and social engagement. Regular assessments of these plans are also indicated.
- Aging in Place: Facilities are required to outline their policies for residents whose needs change over time, ensuring that families are informed about the facility's capabilities and limitations.
- Staff Training and Environment: The form requires details about staff training and facility safety features, reflecting a commitment to resident well-being and security.
Completing and understanding the DADS 3647 form benefits everyone involved in the assisted living process. It empowers residents, families, and facility staff alike to foster a transparent and supportive community.
Browse Other Templates
Virginia Real Estate Contract for Sale by Owner - The property being sold is clearly described, including its legal description and address.
Marine Corps Family Care Documentation,Service Member Family Support Form,Military Family Care Assurance Worksheet,Dependent Care Responsibility Plan,Family Care Preparedness Document,Service Member Caregiver Designation Form,Family Assistance Planni - It is important for service members to keep this form updated to meet command requirements.