Fill Out Your Dcss 0054 Form
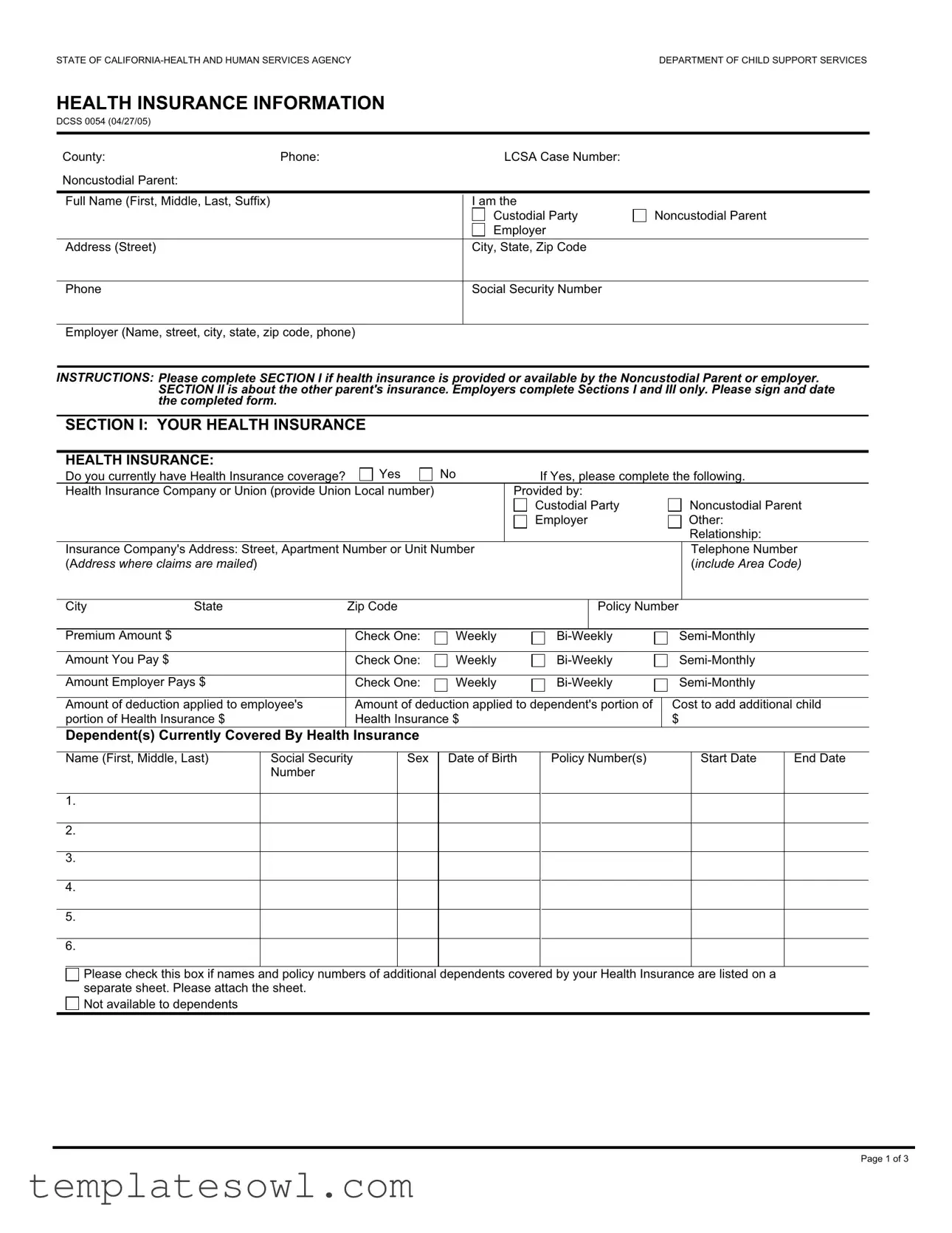
The DCSS 0054 form serves a critical function in the management of child support agreements by gathering comprehensive health insurance information. This document is essential in determining the availability of health, dental, and vision insurance for children involved in custody arrangements. The form is divided into clear sections, allowing custodial and noncustodial parents to provide relevant insurance details. Section I seeks to collect information regarding the insurance held by the noncustodial parent or their employer, including company name, policy numbers, and coverage specifics. Moreover, it asks about additional costs, such as premiums paid by both parties. Section II addresses the insurance provided by the other parent, ensuring that all relevant parties are accounted for in the child's health coverage. A third section is dedicated to confirming the submission of insurance cards or related documentation. Privacy concerns are also acknowledged within the form, emphasizing the importance of collected personal information solely for child support purposes. With direct instructions guiding the user through each section, this form aims to facilitate transparency and coordination between parents in fulfilling their responsibilities towards children’s health care needs.
Dcss 0054 Example
STATE OF
HEALTH INSURANCE INFORMATION
DCSS 0054 (04/27/05)
County: |
Phone: |
LCSA Case Number: |
|
Noncustodial Parent: |
|
|
|
|
|
|
|
Full Name (First, Middle, Last, Suffix) |
|
I am the |
|
|
|
Custodial Party |
Noncustodial Parent |
|
|
Employer |
|
Address (Street) |
|
City, State, Zip Code |
|
Phone
Social Security Number
Employer (Name, street, city, state, zip code, phone)
INSTRUCTIONS: Please complete SECTION I if health insurance is provided or available by the Noncustodial Parent or employer. SECTION II is about the other parent's insurance. Employers complete Sections I and III only. Please sign and date the completed form.
SECTION I: YOUR HEALTH INSURANCE
HEALTH INSURANCE:
Do you currently have Health Insurance coverage? |
Yes |
No |
If Yes, please complete the following. |
||||
Health Insurance Company or Union (provide Union Local number) |
|
Provided by: |
|
|
|||
|
|
|
|
Custodial Party |
|
Noncustodial Parent |
|
|
|
|
|
Employer |
|
Other: |
|
|
|
|
|
|
|
|
Relationship: |
Insurance Company's Address: Street, Apartment Number or Unit Number |
|
|
|
Telephone Number |
|||
(Address where claims are mailed) |
|
|
|
|
|
(include Area Code) |
|
|
|
|
|
|
|
|
|
City |
State |
Zip Code |
|
|
Policy Number |
||
|
|
|
|
|
|
|
|
Premium Amount $ |
|
Check One: |
Weekly |
||||
|
|
|
|
|
|
|
|
Amount You Pay $ |
|
Check One: |
Weekly |
||||
|
|
|
|
|
|
|
|
Amount Employer Pays $ |
Check One: |
Weekly |
|||||
|
|
|
|
|
|
||
Amount of deduction applied to employee's |
Amount of deduction applied to dependent's portion of |
Cost to add additional child |
|||||
portion of Health Insurance $ |
Health Insurance $ |
|
|
$ |
|
||
Dependent(s) Currently Covered By Health Insurance
|
Name (First, Middle, Last) |
Social Security |
Sex |
Date of Birth |
Policy Number(s) |
Start Date |
End Date |
|
|
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please check this box if names and policy numbers of additional dependents covered by your Health Insurance are listed on a separate sheet. Please attach the sheet.
Not available to dependents
Page 1 of 3
The Policy covers the following: (Check all that apply) |
|
|
|
Doctor Visits |
Medicare Supplemental |
Specific Illness |
Prescription Drugs |
Long Term Care |
Hospital Stays |
Hospital Outpatient |
Other (Specify): |
|
|
(i.e., lab work, physical therapy) |
|
DENTAL INSURANCE:
|
Do you currently have Dental Insurance coverage? |
Yes |
No |
|
|
If Yes, please complete the following. |
|
|
|||||||
|
Dental Insurance Company |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Dental Insurance Company's Address: Street, Apartment Number or Unit Number (address where claims are mailed) |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
State |
Zip Code |
|
|
|
|
Policy Number |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Premium Amount $ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Check One: |
Weekly |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Amount You Pay $ |
|
|
Check One: |
Weekly |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Amount Employer Pays $ |
|
|
Check One: |
Weekly |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Amount of deduction applied to employee's |
Amount of deduction applied to dependent's |
|
Cost to add additional child |
|||||||||||
|
portion of Health Insurance $ |
|
|
portion of health insurance $ |
|
$ |
|
|
|
|
|||||
|
Dependent(s) Covered by Dental Insurance |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Name (First, Middle, Last) |
|
Social Security |
Sex |
Date of Birth |
|
Policy Number(s) |
|
|
Start Date |
|
End Date |
|||
|
|
|
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please check this box if names and policy numbers of additional dependents covered by your Dental Insurance are listed on a separate sheet of paper. Please attach the sheet.
Not available to dependents
VISION INSURANCE:
Do you currently have Vision Insurance coverage? |
Yes |
No |
If Yes, please complete the following. |
Vision Insurance Company |
|
|
|
Vision Insurance Company's Address: Street, Apartment Number or Unit Number (Address where claims are mailed)
City |
State |
|
Zip Code |
|
|
Policy Number |
|
|
|
|
|
|
|
|
|
Premium Amount $ |
|
|
Check One: |
Weekly |
|||
|
|
|
|
|
|
|
|
Amount You Pay $ |
|
|
Check One: |
Weekly |
|||
Amount Employer Pays $ |
|
|
Check One: |
Weekly |
|||
|
|
|
|
|
|||
Amount of deduction applied to employee's |
Amount of deduction applied to dependent's portion |
Cost to add additional child |
|||||
portion of Health Insurance $ |
|
of health insurance $ |
|
|
|
$ |
|
Dependent(s) Covered by Vision Insurance
Name (First, Middle, Last) |
Social Security |
Sex |
|
Number |
|
1. |
|
|
|
|
|
2. |
|
|
|
|
|
3. |
|
|
|
|
|
4. |
|
|
|
|
|
5. |
|
|
|
|
|
6. |
|
|
|
|
|
Date of Birth
Policy Number(s)
Start Date
End Date
Please check this box if names and policy numbers of additional dependents covered by your Vision Insurance are listed on a separate sheet. Please attach the sheet.
Not available to dependents
HEALTH INSURANCE INFORMATION |
Page 2 of 3 |
|
|
DCSS 0054 (04/27/05) |
|
SECTION II: OTHER PARENT'S INSURANCE
HEALTH INSURANCE:
Does the other parent currently provide Health Insurance coverage for the child(ren) or you?  Yes If Yes, please complete the following information.
Yes If Yes, please complete the following information.
No
Health Insurance Company
Health insurance Company's Address: Street, Apartment Number or Unit Number (Address where claims are mailed)
City |
State |
Zip Code |
|
|
|
|
|
|
|
DENTAL INSURANCE: |
|
|
|
|
Does the other parent currently provide Dental Insurance coverage for the child(ren) or you? |
Yes |
No |
||
If Yes, please complete the following information. |
|
|
|
|
Dental Insurance Company |
|
|
|
|
Dental Insurance Company's Address: Street, Apartment Number or Unit Number (Address where claims are mailed)
City |
State |
Zip Code |
|
|
|
|
|
|
|
VISION INSURANCE: |
|
|
|
|
Does the other parent currently provide Vision Insurance coverage for the child(ren) or you? |
Yes |
No |
||
If Yes, please complete the following information. |
|
|
|
|
Vision Insurance Company |
|
|
|
|
Vision Insurance Company's Address: Street, Apartment Number or Unit Number (Address where claims are mailed)
City |
State |
Zip Code |
SECTION III: (MUST BE COMPLETED)
I have enclosed the insurance card(s)/information about the coverage for the child(ren).
At this time I do not have the insurance cards/information about the coverage for the child(ren). I will send the information to you when I get it from the insurance company.

 At this time there is no health insurance coverage available. I understand that if it becomes available, I will have to add my child(ren) onto the plan and then notify the local child support agency of the coverage. Coverage is unavailable because:
At this time there is no health insurance coverage available. I understand that if it becomes available, I will have to add my child(ren) onto the plan and then notify the local child support agency of the coverage. Coverage is unavailable because:
Not offered
Seasonal
Refused enrollment
Unreasonable in cost
Probationary period/date eligible
PRIVACY STATEMENT
The information Practices Act of 1997 (Civil Code Section 1798.17) and the Federal Privacy Act of 1974 (Public Law
Social Security Number information is mandatory and will be kept on file at the local child support agency to locate and identify individuals and assets for the purpose of establishing, modifying, and enforcing child support obligations. Enrolling a child in health insurance may require the release of the child's Social Security Number and mailing address to the other parent's employer or the release of the child's Social Security Number to the other parent.
The information in your case may be discussed with or given to the State, other agencies that can legally receive such information, and to the other parent or his/her attorney to the extent required by law.
SIGNATURE |
|
DATE |
|
|
|
|
|
|
|
|
PRINTED NAME |
TELEPHONE (include Area Code) |
|
|
|
|
|
|
|
|
TITLE |
|
|
|
|
|
|
|
|
HEALTH INSURANCE INFORMATION |
|
Page 3 of 3 |
|
|
DCSS 0054 (04/27/05) |
|
|
|
|
Form Characteristics
| Fact Name | Fact Description |
|---|---|
| Form Title | DCSS 0054 is the Health Insurance Information form used by California's Department of Child Support Services. |
| Governing Law | The form is governed under California Family Code sections related to child support and health insurance obligations. |
| Purpose | The purpose of the form is to collect health insurance information for the child(ren) from parents involved in child support cases. |
| Sections | The form consists of three sections: Health Insurance, Dental Insurance, and Vision Insurance. |
| Completion Requirement | Section I must be completed by the noncustodial parent or their employer if health insurance is available. |
| Dependent Coverage | The form allows for listing of dependents covered under the insurance plans, ensuring compliance with child support orders. |
| Privacy Statement | A privacy statement is included, informing about the confidentiality of personal information collected under California and federal law. |
| Date of Issue | The version of the form in use is dated April 27, 2005. |
| Signature Requirement | A signature, date, printed name, and contact information must be included upon completion of the form. |
Guidelines on Utilizing Dcss 0054
Completing the DCSS 0054 form is essential when you need to provide health insurance information related to child support matters. Make sure all sections are filled accurately, as this helps the relevant agencies process the information efficiently.
- Gather Necessary Information: Before starting the form, collect all required documents, such as insurance cards, your Social Security Number, and any necessary employer details.
- Fill Out Basic Information: In the top section, provide the county name, phone number, local child support agency (LCSA) case number, and the full name of the noncustodial parent.
- Indicate Your Role: Check the box for whether you are the custodial party or the noncustodial parent.
- Complete Section I: If the noncustodial parent or their employer provides health insurance, answer the questions regarding the health insurance. Include details like the insurance company name, address, policy number, and premiums.
- List Dependents: Provide names, Social Security numbers, dates of birth, and policy numbers for each dependent covered by the health insurance. Attach a separate sheet if necessary.
- Fill Out Dental and Vision Insurance: If applicable, complete the sections about dental and vision insurance in the same format. Make sure to follow the same protocol for listing dependents.
- Complete Section II: Answer questions about the other parent's insurance. If they provide coverage, fill in the necessary details.
- Complete Section III: Choose the appropriate options regarding the availability of health insurance coverage. Ensure you indicate whether you have enclosed insurance cards or need to provide that information later.
- Review for Accuracy: Double-check all entries for accuracy. Ensure names, numbers, and addresses are correct to avoid complications.
- Sign and Date: Finally, sign and date the form. Print your name and provide your contact number.
- Submit the Form: Send the completed form to the designated local child support agency office or according to the provided instructions.
What You Should Know About This Form
What is the DCSS 0054 form?
The DCSS 0054 form, also known as the Health Insurance Information form, is used in California by the Department of Child Support Services. It collects details about health, dental, and vision insurance plans available for custodial and noncustodial parents and their children. This form helps to ensure that health coverage is provided as part of child support obligations.
Who needs to fill out the DCSS 0054 form?
The form is generally completed by noncustodial parents or their employers if health insurance is available. Custodial parents may also fill out the form to provide information about their own health coverage and any available insurance for the child. It's essential for both parties involved in a child support case to understand and report the health insurance situation.
What information will I need to provide on the form?
You will need to provide personal details such as your name, contact information, and Social Security number. If applicable, you should also include information about health, dental, and vision insurance policies, the names of dependents covered, premiums, and employer contributions. The form has sections to specify each type of insurance coverage, so gather any necessary documents before filling it out.
What if I don’t have health insurance?
If you or the other parent do not have health insurance coverage for the child(ren), the form allows you to indicate this. You will still need to complete the relevant sections, explaining why coverage is unavailable, such as job conditions or cost issues. It is crucial to keep the local child support agency informed about changes regarding health insurance to ensure compliance with child support obligations.
Are there consequences for not completing the form?
Not completing the form can complicate the child support process, as it provides essential information regarding healthcare coverage. If the required information is missing, it may delay support decisions or result in enforcement actions. Timely submission helps ensure that child support includes necessary provisions for the health and well-being of the child or children involved.
How do I submit the DCSS 0054 form?
After completing the DCSS 0054 form, you should submit it to your local child support agency. Depending on the agency's guidelines, you may be able to send it via mail, fax, or electronically. Be sure to check the submission methods available to ensure prompt processing.
Is my personal information kept confidential?
Yes, the information provided on the DCSS 0054 form is subject to confidentiality provisions under both state and federal laws. However, some information may be shared with other parties involved in the child support process, including the other parent or their attorney, when required by law. Make sure to review the privacy statement included with the form to understand how your data may be used.
Can I add new health insurance information later?
Yes, if your situation changes and new health insurance becomes available, you can update the local child support agency with your new information. It's important to notify them promptly, as you may be required to add your child or children to the new plan and provide updated coverage details.
What should I do if I have questions about the form?
If you have questions about filling out the DCSS 0054 form, reach out to your local child support agency for assistance. They can provide guidance on how to complete the form correctly and ensure you include all necessary information. Additionally, you can consult with a legal expert if you need further clarification on your rights and obligations related to child support and health insurance.
Common mistakes
Completing the DCSS 0054 form accurately is essential for ensuring that child support services can operate effectively. One common mistake people make is failing to provide complete information. Each section of the form requires specific details about health insurance coverage, including the company name, policy number, and coverage amounts. Leaving out any of this crucial information can result in processing delays and may cause complications in securing necessary support.
Another frequent error involves inaccurate or outdated information. Individuals must ensure that the information they provide reflects their current situation. This includes proper addresses for insurance companies and current policy numbers. An outdated employer address or incorrect policy number can lead to confusion and difficulty in reaching the necessary parties for claims.
Many also overlook the importance of verifying dependent information. Individuals should carefully check the names, Social Security numbers, and other relevant details for each dependent listed on the form. Inaccuracies in this section can lead to complications in managing the health insurance coverage for the children involved, as well as issues with claims that may arise later.
Lastly, people sometimes neglect to sign and date the form upon completion. A missing signature can invalidate the document, requiring a new submission and further delays in processing. It is crucial to review the entire form to ensure not only that all required information is provided but also that the appropriate signatures are present before submitting it.
Documents used along the form
The DCSS 0054 form collects essential information about health insurance coverage for children in child support cases. Alongside this form, there are several other documents commonly utilized to ensure comprehensive coverage and compliance with legal requirements. Each document fulfills a specific role in the process, helping to clarify rights and obligations regarding health insurance.
- DCSS 0070 - Health Insurance Coverage Availability Form: This form aids in reporting whether health insurance is available to the noncustodial parent and identifying existing coverage options.
- DCSS 0055 - Declaration of Health Insurance Coverage: A sworn statement by the custodial parent or child support agency confirming the health insurance coverage details for the child.
- Child Support Order: This official document outlines the financial obligations of the noncustodial parent, including responsibilities for health insurance costs.
- Employer Verification Form: This form verifies employment status and benefits provided by the employer, crucial for determining health insurance availability.
- Child Medical Support Notice: A notice to ensure that both parents are aware of their duties to provide medical support for their child and explains their options for obtaining health insurance.
- Health Insurance Premium Worksheet: A tool used to calculate monthly premiums and help determine cost-sharing responsibilities associated with the child's coverage.
- Connecting for Kids - Benefits Application: An application form used to seek additional benefits or programs related to health insurance for eligible children, often through state programs.
- Insurance Card Copies: Copies of insurance cards serve as proof of coverage and assist in the processing of claims related to the child's health needs.
- Dependent Coverage Eligibility Form: A formal request to determine if a child is eligible for health insurance coverage under a parent's existing plan.
- Affidavit of Financial Support: A document completed by the custodial parent, declaring financial support specifics related to health insurance expenses.
Understanding these forms and documents ensures that all parties are adequately informed and that children receive the necessary health care coverage as mandated by law. Prompt attention to completing and submitting these documents is crucial in maintaining compliance and ensuring the welfare of the children involved.
Similar forms
- Health Insurance Marketplace Application: Similar to the DCSS 0054 form, the Health Insurance Marketplace application gathers personal information regarding health insurance coverage options. Both documents emphasize the need to identify who has coverage and detail the type of insurance available.
- Employer Health Insurance Benefits Enrollment Form: This form also collects information about an individual's health insurance. Just like the DCSS 0054, it requires details about the policyholder, insurance provider, and type of coverage. Both forms help in establishing access to health benefits, particularly for dependents.
- Child Health Plus Enrollment Form: This enrollment form operates similarly, specifically focusing on children's health coverage. It requires details about available insurers and the child's eligibility, paralleling the DCSS 0054 in ensuring appropriate health coverage for minors.
- Medicaid Application: When applying for Medicaid, individuals must provide detailed information about current health coverage. As with the DCSS 0054, it assesses the individual's financial situation and health insurance availability to determine eligibility for assistance.
- Your Benefits Now Form: This form is used to apply for various public assistance programs, including healthcare. Much like the DCSS 0054, it requires personal data and details about existing health insurance for an accurate assessment of benefits and resources.
- Dependent Care Benefits Verification Form: This document helps organizations verify the benefits available for dependents. It mirrors the DCSS 0054 in gathering information about current coverage for dependents, including health, dental, and vision insurance, ensuring comprehensive care for children.
Dos and Don'ts
Things to Do When Filling Out the DCSS 0054 Form:
- Provide accurate and complete information for each required field.
- Use the correct name and social security number for both parents and children.
- Attach any additional sheets if necessary, particularly for dependents.
- Sign and date the form to validate your submission.
- Review the form thoroughly before submission to ensure there are no mistakes.
Things Not to Do When Filling Out the DCSS 0054 Form:
- Do not leave any required fields blank.
- Avoid using abbreviations or slang in addresses and names.
- Do not submit the form without all necessary attachments and documentation.
- Do not provide outdated or incorrect insurance information.
- Refrain from ignoring the instructions specific to each section of the form.
Misconceptions
Misconceptions about the DCSS 0054 form often lead to confusion. Understanding the facts can make the process clearer for everyone involved. Here are five common misconceptions:
- You must provide insurance information immediately. While it's important to share health insurance details, you can indicate on the form if you don’t currently have coverage. It's acceptable to state that you will send the information when it becomes available.
- The form is only for custodial parents. This is not true. Both custodial and noncustodial parents can fill out the DCSS 0054 form. It asks for insurance information from both parents to ensure the children’s needs are met.
- The form only requires health insurance details. In addition to health insurance, the form also addresses dental and vision insurance. It’s vital to complete all sections that apply to accurately reflect the coverage available for the children.
- Your personal information is not protected. The information you provide on the DCSS 0054 form is protected by privacy laws. It is used solely for the purpose of child support services and is not shared unnecessarily.
- You cannot update the information later. If your coverage changes or new insurance becomes available, you can update the information. It is encouraged to keep the local child support agency informed to reflect any changes in the child's insurance status.
Clearing up these misconceptions can foster better communication and understanding among parents, ensuring that children's health needs are prioritized.
Key takeaways
When filling out and using the DCSS 0054 form, there are several important points to keep in mind. Here are some key takeaways to help you through the process:
- Provide Accurate Information: Ensure that all details entered are precise and complete. Missing data can lead to delays or complications in processing.
- Complete Relevant Sections: Fill out Section I if you, as the noncustodial parent, provide health insurance. If the other parent has insurance, you will need to complete Section II as well.
- Insurance Coverage Details: Be prepared to provide specific information about the insurance company, policy numbers, premiums, and the coverage details of the insurance plan.
- List Dependents: Clearly list all dependents covered by the insurance, ensuring their names, Social Security numbers, and dates of birth are accurate.
- Signature Required: Remember to sign and date the form once it is completed. An unsigned form may be considered invalid.
- Privacy Considerations: Understand that your social security number and other personal information will be used by the Department of Child Support Services for identification and communication purposes.
By following these guidelines, you can navigate the DCSS 0054 form more effectively, helping to ensure that your child's insurance information is processed without unnecessary delays.
Browse Other Templates
What Not to Say in a Police Statement - Retain a copy of the completed form for your records if needed in the future.
Incorporate in Georgia - Certain businesses may need to update branding materials post-amendment.