Fill Out Your Dd 2494 1 Form
The DD Form 2494-1 is a crucial document used by active duty military personnel to enroll their family members in the Supplemental TRICARE Active Duty Family Member Dental Plan (FMDP). This form facilitates dental insurance coverage for eligible family members and is completed voluntarily, though it is important to provide all required information to avoid delays in enrollment. The form outlines specific conditions when it should be filled out, such as when family members live in different locations or when there are multiple dependents under the age of four. Enrollment in the FMDP is typically for a minimum of two years, highlighting the need for accurate and current information as changes in family status must be reported promptly. Essential to the process is the Defense Enrollment Eligibility Reporting System (DEERS), which maintains eligibility records for TRICARE. The form also addresses important reminders about deductions and eligibility verification, ensuring that family members receive timely dental care coverage. A complete understanding of this form contributes significantly to maintaining the health and well-being of active duty personnel's families.
Dd 2494 1 Example
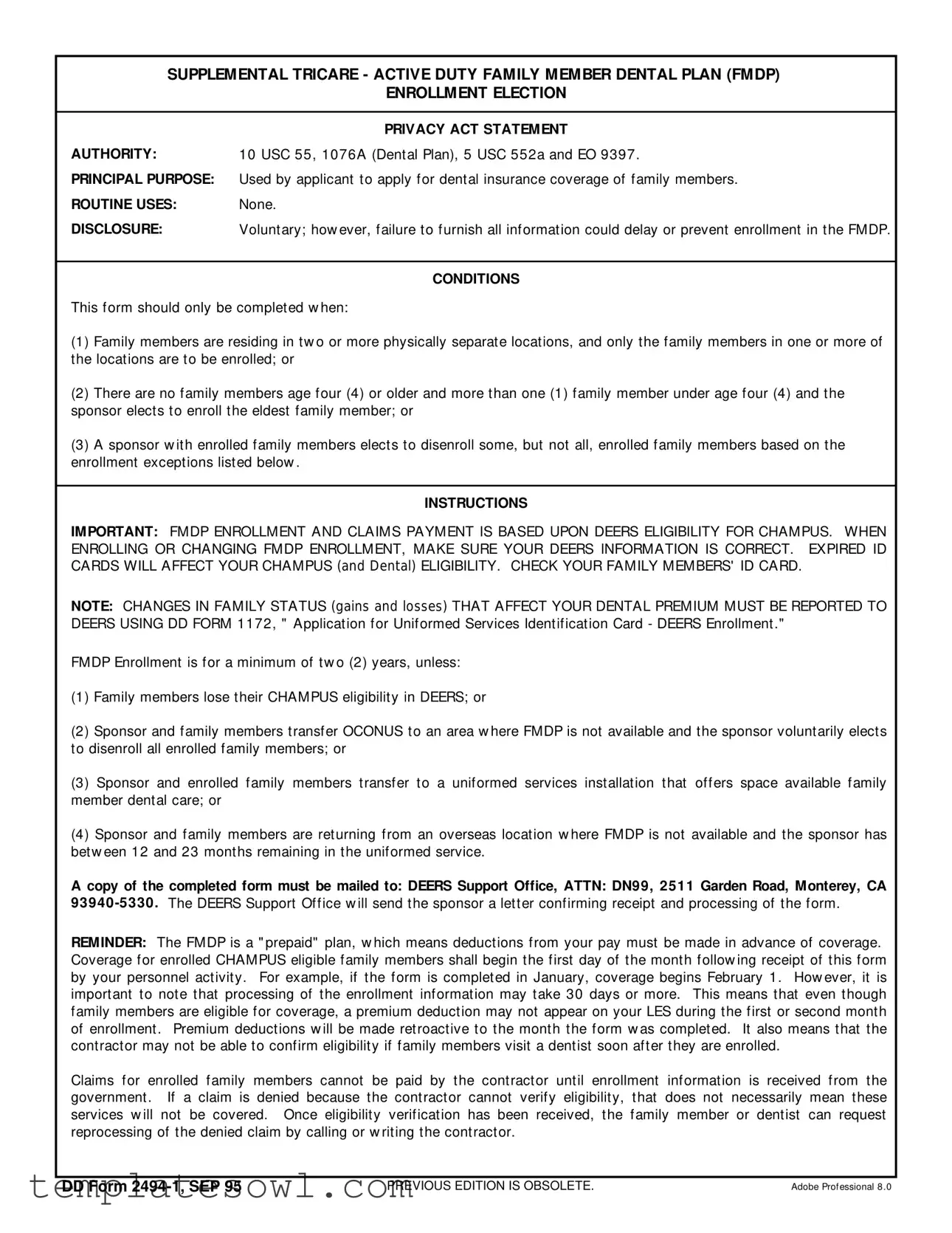
SUPPLEMENTAL TRICARE - ACTIVE DUTY FAMILY MEMBER DENTAL PLAN (FMDP)
ENROLLMENT ELECTION
|
PRIVACY ACT STATEMENT |
AUTHORITY: |
10 USC 55, 1076A (Dent al Plan), 5 USC 552a and EO 9397 . |
PRINCIPAL PURPOSE: |
Used by applicant t o apply f or dent al insurance coverage of f amily members. |
ROUTINE USES: |
None. |
DISCLOSURE: |
Volunt ary; how ever, f ailure t o f urnish all inf ormat ion could delay or prevent enrollment in t he FMDP. |
CONDITIONS
This f orm should only be complet ed w hen:
(1) Family members are residing in t w o or more physically separat e locat ions, and only t he f amily members in one or more of t he locat ions are t o be enrolled; or
(2)There are no f amily members age f our (4) or older and more t han one (1) f amily member under age f our (4) and t he sponsor elect s t o enroll t he eldest f amily member; or
(3)A sponsor w it h enrolled f amily members elect s t o disenroll some, but not all, enrolled f amily members based on t he enrollment except ions list ed below .
INSTRUCTIONS
IMPORTANT: FMDP ENROLLMENT AND CLAIMS PAYMENT IS BASED UPON DEERS ELIGIBILITY FOR CHAMPUS. WHEN ENROLLING OR CHANGING FMDP ENROLLMENT, MAKE SURE YOUR DEERS INFORMATION IS CORRECT. EXPIRED ID CARDS WILL AFFECT YOUR CHAMPUS (and Dental) ELIGIBILITY. CHECK YOUR FAMILY MEMBERS' ID CARD.
NOTE: CHANGES IN FAMILY STATUS (gains and losses) THAT AFFECT YOUR DENTAL PREMIUM MUST BE REPORTED TO DEERS USING DD FORM 1172, " Applicat ion f or Unif ormed Services Ident if icat ion Card - DEERS Enrollment ."
FMDP Enrollment is f or a minimum of t w o (2) years, unless:
(1) Family members lose t heir CHAMPUS eligibilit y in DEERS; or
(2) Sponsor and f amily members t ransf er OCONUS t o an area w here FMDP is not available and t he sponsor volunt arily elect s t o disenroll all enrolled f amily members; or
(3)Sponsor and enrolled f amily members t ransf er t o a unif ormed services inst allat ion t hat of f ers space available f amily member dent al care; or
(4) Sponsor and f amily members are ret urning f rom an overseas locat ion w here FMDP is not available and t he sponsor has bet w een 12 and 23 mont hs remaining in t he unif ormed service.
A copy of the completed form must be mailed to: DEERS Support Office, ATTN: DN99, 2511 Garden Road, Monterey, CA 93940
REMINDER: The FMDP is a " prepaid" plan, w hich means deduct ions f rom your pay must be made in advance of coverage. Coverage f or enrolled CHAMPUS eligible f amily members shall begin t he f irst day of t he mont h f ollow ing receipt of t his f orm by your personnel act ivit y. For example, if t he f orm is complet ed in January, coverage begins February 1. How ever, it is import ant t o not e t hat processing of t he enrollment inf ormat ion may t ake 30 days or more. This means t hat even t hough f amily members are eligible f or coverage, a premium deduct ion may not appear on your LES during t he f irst or second mont h of enrollment . Premium deduct ions w ill be made ret roact ive t o t he mont h t he f orm w as complet ed. It also means t hat t he cont ract or may not be able t o conf irm eligibilit y if f amily members visit a dent ist soon af t er t hey are enrolled.
Claims f or enrolled f amily members cannot be paid by t he cont ract or unt il enrollment inf ormat ion is received f rom t he government . If a claim is denied because t he cont ract or cannot verif y eligibilit y, t hat does not necessarily mean t hese services w ill not be covered. Once eligibilit y verif icat ion has been received, t he f amily member or dent ist can request reprocessing of t he denied claim by calling or w rit ing t he cont ract or.
DD FORM |
PREVIOUS EDITION IS OBSOLETE. |
Adobe Prof essional 8 .0 |
SECTION I - ACTIVE DUTY MEMBER ELIGIBILITY INFORMATION
1 . SPONSOR' S NAME (LAST, First, Middle Initial) |
|
2 . SPONSOR' S SOCIAL SECURITY NUMBER |
3. SPONSOR' S GRADE |
|||
|
|
|
|
|
||
4 . SPONSOR' S UNIT |
|
|
5. DATE OF EXPIRATION OF SERVICE OR |
|||
|
|
|
|
|
CONTRACT (As extended) (YYMMDD) |
|
|
|
|
|
|
|
|
|
|
|
SECTION II - COVERAGE INFORMATION |
|
||
|
|
|
|
|
|
|
6. ELECTION OF COVERAGE (Use additional copies of this form if needed for enrolling more family members.) |
|
|||||
|
|
|
|
|
|
|
5 |
|
I have one (1) geographically separat ed f amily member f or w hom I am elect ing coverage. |
|
|||
|
|
|
|
|
|
|
6 |
|
I have more t han one (1) geographically separat ed f amily member f or w hom I am elect ing coverage. |
|
|||
|
|
|
|
|
|
|
SPONSORS WITH 12 TO 23 MONTHS RETENTION RETURNING FROM AN OCONUS AREA WHERE FMDP WAS NOT AVAILABLE:
NOTE: These enrollment codes may only be used f or sponsors enrolling f amily members ret urning f rom an OCONUS area w here FMDP w as not available. If t he f amily members did not accompany t he sponsor on t he OCONUS t our, t he sponsor may not enroll t he f amily members.
T |
|
|
OCONUS Ret urnee. I have one (1) geographically separat ed f amily member f or w hom I am elect ing coverage. |
|||
|
|
|
|
|||
U |
|
|
OCONUS Ret urnee. I have more t han one (1) geographically separat ed f amily member f or w hom I am elect ing coverage. |
|||
|
|
|
|
|
||
List only t hose f amily members t o be enrolled in t he blocks below . |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
FULL CURRENT ADDRESS |
|
DATE OF BIRTH |
|
|
NAME (Last, First, Middle Initial) |
(Number, Street, City, State, ZIP Code) |
|
(YYMMDD) |
|
|
|
|
a. |
b. |
|
c. |
|
|
|
|
|
|
|
(1) |
|
|
|
|
|
|
|
|
|
|
|
|
|
(2) |
|
|
|
|
|
|
|
|
|
|
|
|
|
(3) |
|
|
|
|
|
|
|
|
|
|
|
|
|
(4) |
|
|
|
|
|
|
|
|
|
|
|
|
|
(5) |
|
|
|
|
|
|
|
|
|
|
|
|
|
(6) |
|
|
|
|
|
|
|
|
|
|
|
|
|
7. STATEMENT OF UNDERSTANDING |
|
|
|
|||
|
|
|
|
|
||
|
I have checked my f amily member inf ormat ion in DEERS and verif ied t he accuracy of t he DEERS inf ormat ion. |
I underst and t hat I must |
||||
complet e a new enrollment f orm if I w ant t o change t he enrollment st at us of my f amily members (such as adding family members not listed on this form). I also underst and I may not t erminat e enrollment based on a change in f amily size. If my DEERS record indicat es a f amily member is no longer eligible, a change w ill occur aut omat ically w it h no act ion on my part . I f urt her underst and t hat t he premium rat e f or t his program is subject t o change. I also underst and t hat during t he t w o year minimum enrollment period I cannot disenroll due t o a change in premium rat e. I underst and t hat enrollment in FMDP aut omat ically t erminat es t he last day of t he mont h of act ive dut y or upon terminat ion of basic pay. I aut horize payroll deduct ions t o be t aken f rom my pay based upon t he inf ormat ion in DEERS and my coverage elect ion specif ied above.
a. SPONSOR SIGNATURE |
|
|
b. DATE SIGNED |
|
|
|
|
|
(YYMMDD) |
|
|
|
||
8 . |
WITNESSING OFFICIAL (Give the sponsor a signed copy of this form.) |
|
||
|
|
|
|
|
a. |
NAME (Last, First, Middle Initial) |
b. GRADE |
c. SIGNATURE |
d. DATE SIGNED |
|
|
|
|
(YYMMDD) |
|
|
|
|
|
DD Form 2494
Form Characteristics
| Fact Name | Details |
|---|---|
| Form Purpose | This form is used to enroll active duty family members in the TRICARE dental plan. |
| Governing Authority | The form operates under 10 USC 55, 1076A, 5 USC 552a, and EO 9397. |
| Enrollment Conditions | Enrollments are allowed under specific conditions related to family member locations and ages. |
| Disclosure | Providing all requested information is important; missing details can delay enrollment. |
| Minimum Enrollment Period | Enrollment lasts a minimum of two years, subject to certain eligibility conditions. |
| Processing Time | Processing may take 30 days or more; premiums will be retroactive to the month the form is completed. |
| Submission Address | The completed form should be sent to DEERS Support Office at a designated address in Monterey, CA. |
Guidelines on Utilizing Dd 2494 1
Once you have gathered the necessary information, you can begin filling out the DD Form 2494-1 for the Supplemental TRICARE Active Duty Family Member Dental Plan. This form is essential for enrolling your eligible family members in dental coverage. Follow these steps carefully to ensure all required sections are completed accurately.
- In Section I, provide the following details about the active duty sponsor:
- 1. Enter the sponsor's name, listing the last name first followed by the first and middle initial.
- 2. Input the sponsor's Social Security Number.
- 3. Indicate the sponsor's military grade.
- 4. Provide the sponsor's unit information.
- 5. Enter the date of expiration of service or contract, formatted as YYMMDD.
- In Section II, indicate coverage information:
- 6. Choose the appropriate election of coverage based on the number of geographically separated family members. Use additional copies of the form if necessary.
- 7. If applicable, fill in the returnee options if the sponsor is returning from an OCONUS area and select the number of family members.
- 8. List the full current address and date of birth for each family member being enrolled.
- Review the Statement of Understanding in Section II to confirm comprehension and agreement with the terms.
- At the bottom of the form, the sponsor must:
- a. Provide a signature.
- b. Input the date signed in YYMMDD format.
- Have an official witness sign the form, including:
- a. Name of the witnessing official (last, first, middle initial).
- b. Their grade.
- c. Signature.
- d. Date signed in YYMMDD format.
- Make a copy of the completed form before mailing it to the specified address: DEERS Support Office, ATTN: DN99, 2511 Garden Road, Monterey, CA 93940-5330.
After submitting the form, expect confirmation from the DEERS Support Office regarding the processing of your enrollment. It may take time for your coverage to activate, so keep this in mind as you await further instructions.
What You Should Know About This Form
What is the purpose of the DD Form 2494-1?
The DD Form 2494-1 is used by active duty service members to enroll their family members in the Supplemental TRICARE - Active Duty Family Member Dental Plan (FMDP). By completing this form, you can apply for dental insurance coverage for your eligible family members. This process is important to ensure your family members receive the dental care they need.
Who should complete the DD Form 2494-1?
This form should be filled out when specific situations arise for your family. For example, if family members live in different locations and only some need coverage, or if there are multiple family members under age four, and you choose the eldest for coverage, then this form is applicable. Additionally, if you are a sponsor who wants to disenroll some but not all enrolled family members, you should also complete this form.
How long does coverage last once I enroll my family members?
When you enroll your family members in the FMDP, the enrollment is for at least two years. However, there are exceptions that may allow termination earlier. These exceptions include the loss of CHAMPUS eligibility, transferring to an area without FMDP, or changes in your active duty status. Understanding these conditions can help you manage your family's health care more effectively.
What should I do if my family status changes after enrolling?
If your family situation changes, such as gaining or losing a family member, you must report these changes to the Defense Enrollment Eligibility Reporting System (DEERS). This is done using DD Form 1172. Remember, you cannot terminate enrollment based solely on a change in family size during the minimum enrollment period.
How long does it take for my coverage to start after I submit the form?
Coverage for your enrolled family members will begin on the first day of the month following the receipt of the completed form by your personnel activity. It’s essential to note that processing may take 30 days or more. Therefore, your premium deductions may not appear on your Leave and Earnings Statement (LES) initially, but will be made retroactive to when you submitted the form.
Common mistakes
Individuals frequently make errors when completing the DD Form 2494-1, which can lead to delays or complications in enrollment in the Supplemental TRICARE Family Member Dental Plan. One common mistake is not verifying the accuracy of the personal information in the Defense Enrollment Eligibility Reporting System (DEERS) before submitting the form. This data is critical, as any discrepancies can affect eligibility.
Another error involves omitting information about additional family members who require enrollment. Each section of the form must be meticulously filled out. Failure to list all eligible family members may result in their ineligibility for coverage. It is essential to double-check all names and information for accuracy.
Some applicants also neglect to sign and date the form. The sponsor's signature is a crucial element of the application, as it signifies an understanding of the terms and conditions of enrollment. A missing signature leads to automatic rejection of the application, prolonging the enrollment process.
Additionally, individuals often misunderstand the enrollment periods. Applicants may not realize that the FMDP enrollment requires a commitment of at least two years. Misinterpreting this requirement could result in premature disenrollment or unnecessary complications during family transitions.
Another mistake involves not understanding the implications of family status changes. If a sponsor experiences a change in family size, they must report this to DEERS using the proper form, DD Form 1172. Failing to do so could lead to automatic changes in eligibility that may not align with the sponsor’s wishes.
Further, applicants might misinterpret the coverage election codes. Selecting the incorrect code can lead to significant issues regarding which family members are actually enrolled. Understanding the difference between the codes is vital for accurate enrollment.
In some cases, individuals submit the form without considering the potential waiting period for enrollment processing. It can take 30 days or more for the enrollment to be finalized, and families should not expect immediate coverage. This can lead to confusion and frustration if coverage is needed right away.
Lastly, failing to keep a copy of the submitted form may lead to complications down the line. It is advisable for the sponsor to retain a signed copy for their records. This serves as a reference in case any issues arise, helping to ensure streamlined communication with the DEERS Support Office.
Documents used along the form
The DD Form 2494-1 is an important document for enrolling eligible family members in the Supplemental Tricare Dental Plan. When completing this enrollment, there are several other forms and documents that may also be necessary to ensure compliance and proper processing. Below is a list of some of these commonly used documents along with a brief description of each.
- DD Form 1172: This form is used to apply for a Uniformed Services Identification Card and to enroll family members in the DEERS (Defense Enrollment Eligibility Reporting System). It's essential for ensuring valid eligibility for various military benefits.
- DD Form 214: This form provides a summary of a service member’s active duty service. It is often required for various benefits and enrollments, including dental and health care benefits.
- Tricare Enrollment Application: This document is necessary for enrolling in any Tricare program. It details personal and family information needed to establish coverage under Tricare plans.
- DEERS Eligibility Verification: This is often a letter or documentation showing confirmation that an individual is correctly enrolled in DEERS. It's essential for ensuring that family members can access dental benefits.
- Insurance Premium Payment Form: This document is required for setting up automatic deductions for the insurance premiums of enrolled family members. It ensures prompt payment and continued coverage.
In summary, when preparing to enroll in the Supplemental Tricare Dental Plan using the DD Form 2494-1, it is crucial to have these associated documents ready. This will help ensure a smoother enrollment process and avoid delays in accessing necessary dental services for eligible family members.
Similar forms
The DD 2494-1 form has several similar documents that also deal with military family member enrollment and benefits. Here are four of them:
- DD Form 1172: This form is used for applying for a Uniformed Services Identification Card and DEERS Enrollment. Like the DD 2494-1, it requires accurate family information to ensure that all eligible family members are recognized for benefits.
- DD Form 2754: This document serves as a Health Care Benefit Request for the TRICARE program. It shares the same goal of providing coverage for military family members and is used to enroll members in health benefit plans.
- Form SF 2809: This is the Health Benefits Election Form for federal employees. Much like the DD 2494-1, it enables individuals to elect coverage for their family members under a specific health insurance program, ensuring they receive the necessary medical benefits.
- TRICARE Enrollment Form: This document is utilized for enrolling eligible family members in various TRICARE programs. Similar to the DD 2494-1, it outlines choices and requires information about each family member to process the enrollment correctly.
Dos and Don'ts
When filling out the DD Form 2494-1 for the Supplemental TRICARE - Active Duty Family Member Dental Plan (FMDP), there are important guidelines to follow. Adhering to these can help ensure a smooth enrollment process.
- Do double-check the accuracy of all the information you enter on the form.
- Do ensure that you have the correct and up-to-date DEERS information for your family members.
- Do understand that enrollment is for a minimum of two years.
- Do keep a copy of the completed form for your records.
- Don't leave out any required information; this may delay your enrollment.
- Don't assume that you can disenroll at any time based on changes in family status.
- Don't ignore any instructions regarding changes to family coverage.
- Don't forget to report any changes in family status that can affect the dental premium.
Following these do's and don'ts can help you successfully navigate the enrollment process for your family's dental coverage.
Misconceptions
Misunderstandings surrounding the DD Form 2494-1 are common. Here are ten misconceptions, along with clarifications to provide guidance:
- Misconception 1: The form is mandatory for all service members.
- Misconception 2: Submitting the form guarantees immediate dental coverage.
- Misconception 3: You can enroll or disenroll family members at any time.
- Misconception 4: All family members must be enrolled at once.
- Misconception 5: Enrollment status does not change automatically.
- Misconception 6: The form can be submitted without verifying DEERS information.
- Misconception 7: Premium payments are deducted immediately after enrollment.
- Misconception 8: Enrollment can be terminated based solely on changing premium rates.
- Misconception 9: Missing information on the form has minor consequences.
- Misconception 10: All claims will be processed regardless of eligibility verification.
The DD Form 2494-1 is only needed when specific conditions are met, such as having family members residing in multiple locations or when enrolling a family member under the age of four.
While the enrollment process starts upon submission, it may take up to 30 days for coverage to begin. Be patient during this period.
Dental enrollment typically lasts for a minimum of two years without exceptions, which include losing eligibility or transferring overseas.
It is possible to enroll just some family members, depending on your situation. Use additional forms for multiple enrollments if needed.
If DEERS indicates that a family member is no longer eligible, enrollment will automatically terminate without any required action from you.
Before submitting, it is crucial to ensure that all family member information in DEERS is accurate. This helps avoid potential enrollment delays.
Premium deductions may not appear on your pay statement until the second month of enrollment, despite coverage beginning retroactively. Ensure to check your LES carefully.
During the two-year minimum enrollment period, you cannot disenroll due to changes in premium rates. Awareness of this is important for budgeting.
Failing to provide complete information can delay or prevent enrollment in the Family Member Dental Plan. Always ensure the form is fully completed before submission.
If claims are denied due to unverified eligibility, it does not necessarily mean services are not covered. Verification must be received before reprocessing claims.
Understanding these points can help you navigate the complexities associated with the DD Form 2494-1 with greater confidence and clarity.
Key takeaways
Here are some important points to keep in mind when filling out the DD 2494-1 form:
- Purpose of the Form: This form is used to apply for dental insurance coverage for family members.
- Voluntary Disclosure: Providing information is voluntary, but not completing the form fully could delay coverage.
- Eligibility Conditions: Fill out this form only if family members are in two separate locations or if specific age-related conditions apply.
- Correct Information: Ensure that your DEERS information is accurate to avoid complications with eligibility.
- Minimum Enrollment: Enrollment is for a minimum of two years, unless certain conditions regarding relocation or loss of eligibility occur.
- Payment Structure: The FMDP is a prepaid plan, meaning payments are deducted from your pay before coverage begins.
- Processing Time: Processing of enrollment may take 30 days or longer, so expect some delays in premium deductions.
- Claims Issues: If a claim is denied due to verification issues, it doesn't mean the service won’t be covered once eligibility is confirmed.
Browse Other Templates
How Much Does It Cost to Register a Car in Ct - This special permit program is designed to assist working individuals during license suspension.
Vita Flex Fsa - Specify the relationship of each dependent to the employee for clarity.