Fill Out Your Deltacare Usa Form
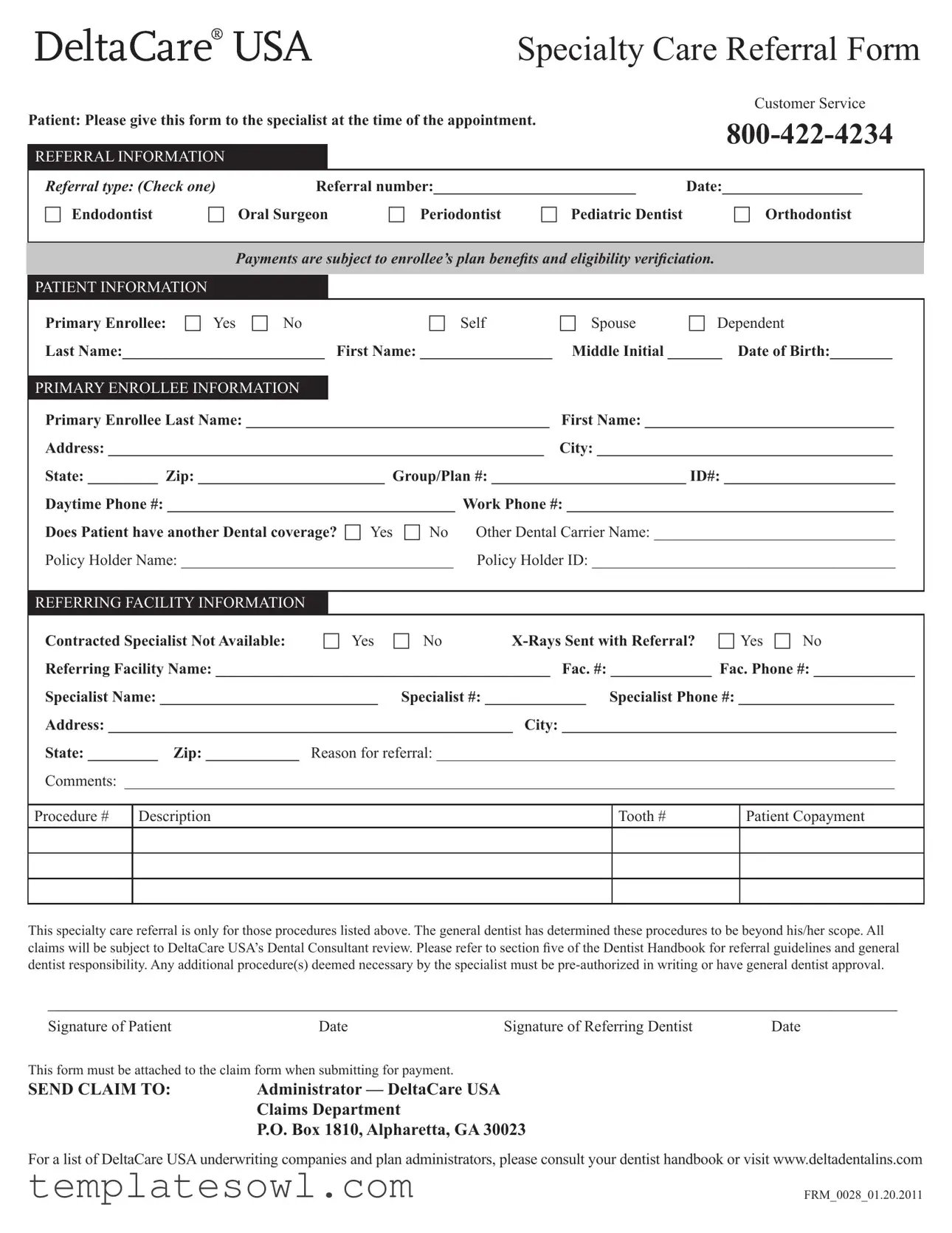
The Deltacare USA form serves a vital role in ensuring patients receive appropriate specialty dental care through a structured referral process. This form is utilized when a general dentist identifies that a patient's needs exceed their practice capabilities, prompting a referral to a specialist such as an endodontist, oral surgeon, or orthodontist. It captures essential details, including patient information, referring dentist facts, and the specific type of specialist required. Additionally, it inquires about existing dental coverage to facilitate financial arrangements and clarify copayment responsibilities. Importantly, patients are required to present the form at their specialty appointments, thus streamlining the process between the general dentist, the specialist, and the insurance provider. Moreover, it emphasizes the necessity of pre-authorization for any additional treatments deemed necessary post-referral, thereby safeguarding both patient and provider interests. The form must also accompany any claims submitted for payment, ensuring compliance with DeltaCare USA's administrative protocols.
Deltacare Usa Example
Specialty Care Referral Form
|
|
|
|
|
|
Customer Service |
Patient: Please give this form to the specialist at the time of the appointment. |
|
|||||
|
|
|
|
|
|
|
REFERRAL INFORMATION |
|
|
|
|
|
|
|
|
|
|
|||
Referral type: (Check one) |
Referral number:__________________________ |
Date:__________________ |
||||
c Endodontist |
c Oral Surgeon |
c Periodontist |
c Pediatric Dentist |
c Orthodontist |
||
|
|
|
|
|
|
|
Payments are subject to enrollee’s plan beneits and eligibility veriiciation.
PATIENT INFORMATION
Primary Enrollee: c Yes c No |
c Self |
c Spouse |
c Dependent |
Last Name:__________________________ |
First Name: _________________ |
Middle Initial _______ Date of Birth:________ |
|
|
|
|
|
PRIMARY ENROLLEE INFORMATION |
|
|
|
Primary Enrollee Last Name: _______________________________________ |
First Name: ________________________________ |
||
Address: ________________________________________________________ |
City: ______________________________________ |
||
State: _________ Zip: ________________________ Group/Plan #: _________________________ ID#: ______________________
Daytime Phone #: _____________________________________ Work Phone #: __________________________________________
Does Patient have another Dental coverage? c Yes |
c No |
Other Dental Carrier Name: _______________________________ |
|
Policy Holder Name: ___________________________________ |
Policy Holder ID: _______________________________________ |
||
|
|
|
|
REFERRING FACILITY INFORMATION |
|
|
|
|
|
|
|
Contracted Specialist Not Available: |
c Yes |
c No |
|
Referring Facility Name: ___________________________________________ Fac. #: _____________ Fac. Phone #: _____________
Specialist Name: ____________________________ Specialist #: _____________ Specialist Phone #: ____________________
Address: ____________________________________________________ City: ___________________________________________
State: _________ Zip: ____________ Reason for referral: ___________________________________________________________
Comments: ___________________________________________________________________________________________________
Procedure # |
Description |
Tooth # |
Patient Copayment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
This specialty care referral is only for those procedures listed above. The general dentist has determined these procedures to be beyond his/her scope. All
claims will be subject to DeltaCare USA’s Dental Consultant review. Please refer to section ive of the Dentist Handbook for referral guidelines and general
dentist responsibility. Any additional procedure(s) deemed necessary by the specialist must be
___________________________________________________________________________________________
Signature of Patient |
Date |
Signature of Referring Dentist |
Date |
This form must be attached to the claim form when submitting for payment.
SEND CLAIM TO: |
Administrator — DeltaCare USA |
|
Claims Department |
|
P.O. Box 1810, Alpharetta, GA 30023 |
For a list of DeltaCare USA underwriting companies and plan administrators, please consult your dentist handbook or visit www.deltadentalins.com
FRM_0028_01.20.2011
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose | This form is used for specialty care referrals within the DeltaCare USA network. |
| Referral Type | Patients must select a type of specialist from several options, including Endodontist and Orthodontist. |
| Patient Information | Information collected includes the patient's name, date of birth, and dental insurance details. |
| Eligibility Verification | Payments for services will be verified against the enrollee's plan benefits and eligibility. |
| Signature Requirement | The form must be signed by both the patient and the referring dentist to be valid. |
| Submission Instructions | This form must accompany the claim form when submitting for payment to DeltaCare USA. |
| State-Specific Guidelines | Each state has its own governing laws related to dental insurance and referrals. Always check local regulations. |
Guidelines on Utilizing Deltacare Usa
To successfully complete the DeltaCare USA Specialty Care Referral Form, gather all required information beforehand. This will help ensure accuracy and efficiency during the process.
- Referral Information:
- Choose the type of referral by checking the appropriate box.
- Fill in the referral number.
- Write the date of completion.
- Patient Information:
- Indicate if the primary enrollee is the patient, spouse, or dependent.
- Provide the patient’s last name, first name, and middle initial.
- Enter the patient’s date of birth.
- Primary Enrollee Information:
- Enter the primary enrollee’s last name and first name.
- Complete the address, including city, state, and zip code.
- Fill in the group/plan number and ID number.
- Provide both daytime and work phone numbers.
- Indicate whether the patient has another dental coverage and provide the necessary details.
- Referring Facility Information:
- Indicate if a contracted specialist is not available.
- State whether X-Rays were sent with the referral.
- Fill in the referring facility name, fax number, and phone number.
- Provide the specialist’s name, specialist number, and phone number.
- Complete the address for the specialist, including city, state, and zip code.
- Explain the reason for the referral and include any additional comments as needed.
- Procedure Information:
- List the procedure number and description.
- Include the tooth number and patient copayment.
- Signatures:
- Obtain the patient’s signature and the date signed.
- Obtain the referring dentist's signature and the date signed.
- Submit the Form:
- Attach this form to the claim form when submitting for payment.
- Send the completed forms to the DeltaCare USA Claims Department at the provided address.
What You Should Know About This Form
What is the DeltaCare USA Specialty Care Referral Form used for?
The DeltaCare USA Specialty Care Referral Form is designed to facilitate referrals from a general dentist to a specialist. It ensures that the necessary information is collected before the patient attends their appointment with the specialist. This includes details about the referral type, patient information, and information about the referring facility. By using this form, patients can receive the specialty care they need while complying with their dental plan guidelines.
Who needs to fill out the referral form?
The referral form must be filled out by the general dentist who is referring the patient to a specialist. It's crucial for the referring dentist to provide accurate information regarding the referral type and reason for the referral on the form. Patients should also complete their sections to provide the specialist with essential information about their dental coverage and any other relevant details. This collaborative effort ensures a smooth transition of care.
What should I do with the form once it's completed?
What happens if my child needs dental care but is also covered under another dental plan?
If your child is covered under another dental plan, it is essential to indicate this on the form. The section regarding additional dental coverage allows you to provide information about the other insurer, including the policyholder's name and ID. This information helps the specialist and your primary dental provider coordinate care and coverage effectively. Be sure to check with both insurance providers regarding their referral processes, as different plans may have unique requirements.
Common mistakes
Filling out the DeltaCare USA Specialty Care Referral Form can seem straightforward, but many people overlook critical details that can lead to delays or denials in coverage. One common mistake is neglecting to accurately complete the patient information section. This section demands precise details, including the full name, date of birth, and relationship to the primary enrollee. Notably, omitting or misspelling any of this information can complicate claims processing, ultimately causing frustration for all parties involved.
Another frequent error arises when individuals fail to check the appropriate referral type. The form provides specific boxes to check for various specialties, such as oral surgeon or orthodontist. By leaving this section incomplete, it becomes unclear what type of care is being requested. This can lead to misunderstandings and may result in the referral being invalid or unprocessed, prolonging the patient's need for care.
Moreover, many users forget to confirm whether they have another dental coverage. The section asks whether the patient has an additional plan, yet failing to indicate this can create issues later. If another coverage exists, it is crucial for the primary insurer to be aware of it to coordinate benefits effectively. Without this information, claims may be incorrectly paid, or benefits may go unutilized.
Lastly, individuals often overlook the importance of signatures on the form. Both the patient and the referring dentist are required to sign and date the document. Missing a signature can render the referral invalid. This simple but critical step cannot be emphasized enough. Failing to ensure all necessary signatures are present can slow down the referral process and complicate any subsequent claims.
Documents used along the form
The DeltaCare USA form is just one part of the overall process when it comes to obtaining specialty dental care. Depending on your specific situation, you may find yourself needing additional documents. Below are a few common forms that are often used alongside the DeltaCare USA form to help facilitate dental appointments and insurance claims.
- Claim Form: This document is essential for submitting your insurance claim after receiving services. It typically requires information about the patient, the services rendered, and any relevant billing codes. Providing accurate details helps ensure that your provider gets reimbursed promptly and correctly.
- Pre-Authorization Request: Before undergoing certain procedures, your dentist may need approval from your insurance company. This form outlines the procedure, its necessity, and your current dental health status. The insurance provider evaluates this information and decides if they will cover the costs involved.
- Patient Consent Form: This document ensures that the patient is aware of and agrees to the treatment plan proposed by the specialist. It often includes information about potential risks and benefits, allowing patients to make informed decisions about their care.
- Orthodontic Evaluation Form: If your referral is for orthodontic care, this form may be required. It gathers information about your dental condition and treatment options. Orthodontists use it to determine the best course of action and whether you are a candidate for braces or other dental appliances.
By understanding these documents, you can streamline your dental care process and ensure that all necessary information is readily available. This can lead to a more efficient experience and ultimately better care.
Similar forms
- Referral Authorization Form: Similar in purpose, this document allows patients to seek services outside their primary care provider. It facilitates the process by enabling easier access to specialized care, ensuring all necessary information is communicated effectively.
- Patient Release Forms: These forms are crucial in handling patient information. They ensure that the dentist or specialist can obtain necessary medical records from other healthcare providers, just as the Deltacare USA form does for specialists.
- Insurance Claim Form: Like the Deltacare USA form, claim forms are essential for documenting services rendered. Both require specific details related to the patient’s appointment, insurance status, and treatment types to facilitate reimbursement.
- Authorization for Treatment Form: This document secures consent from patients for specific treatments. Much like the referral form, it guarantees that patients understand and agree to the proposed services by the dentist or specialist.
- Continuing Care Plan: This outlines follow-up care after a dental procedure. The Deltacare USA form shares a similar goal of ensuring that there is a structured and clear path for patient care across different treatments and specialists.
- Patient Demographics Form: While focused more on collecting patient information, this form serves an essential role in keeping records up-to-date. The Deltacare USA form also collects vital demographic data about patients and their insurance plans.
- Specialist Consultation Form: This document is used when general dentists refer patients to specialists. It captures similar elements like the patient's referral type and insurance information, ensuring a seamless transfer of care from one provider to the next.
Dos and Don'ts
When filling out the DeltaCare USA form, adhering to guidelines can ensure the process runs smoothly. Here’s what you should and shouldn’t do.
- Do read the instructions carefully before starting.
- Do ensure all information is accurate, including names, dates, and contact numbers.
- Do keep a copy of the completed form for your records.
- Do submit the form promptly to avoid delays in care.
- Do double-check that the referring dentist has signed the form.
- Don’t leave any required fields blank as this can result in processing issues.
- Don’t provide incorrect or outdated information about your dental coverage.
- Don’t forget to specify the reason for the referral clearly.
- Don’t attach the form to the claim after the deadline.
- Don’t assume that a verbal agreement with the specialist counts; always get everything in writing.
Misconceptions
- Misconception 1: The Deltacare USA form is optional for patients.
- Misconception 2: Patients can see any specialist without a referral.
- Misconception 3: The primary enrollee does not need to be involved in the process.
- Misconception 4: The referral is a one-time requirement.
- Misconception 5: The form does not require a signature.
- Misconception 6: Submitting the form guarantees automatic payment.
In reality, presenting this form to the specialist during your appointment is essential. It ensures that the specialist has the necessary referral information to proceed with treatment.
This form functions as a formal referral. Without it, seeing a specialist under the Deltacare USA plan might not be covered, leading to unexpected costs.
In fact, the primary enrollee's information is crucial. They must verify their plan benefits and ensure eligibility, which can affect coverage for specialty services.
Each referral is specific to procedures noted on the form. Should additional procedures arise, those need separate authorizations from the general dentist.
Signatures from both the patient and the referring dentist are necessary. This agreement confirms the understanding of what services were referred.
While the form is important, all claims will undergo DeltaCare USA’s dental consultant review. Payment still hinges on plan benefits and eligibility verification.
Key takeaways
When filling out the Deltacare USA form, there are several important elements to keep in mind. Here are key takeaways to help ensure a smooth process:
- Complete the Referral Section: Make sure to check the appropriate referral type for the specialist you are visiting. Options include endodontists, oral surgeons, and more.
- Provide Accurate Patient Information: Fill in the patient's name, date of birth, and other identifying details carefully. Accuracy is crucial.
- Detail Primary Enrollee Information: Include the information for the main enrollee, including their name, address, and phone number.
- Insurance Coverage: Indicate if the patient has another dental plan. This can affect payment and processing.
- Referral Facility Information: Ensure the referring facility's information is correct, including the specialist’s name and contact details.
- Attach Necessary Documents: If applicable, include any X-rays or additional documentation required with the referral.
- Review Procedure Details: List any procedures being referred to the specialist and provide relevant tooth numbers if necessary.
- Signature Requirement: Both the patient and referring dentist must sign the form. This confirms the referral.
- Submit the Claim Correctly: Don’t forget to attach the completed referral form to the claim form when submitting for payment.
- Consult the Dentist Handbook: For more guidance and information on the referral process, check the dentist handbook or the DeltaCare USA website.
These takeaways can help streamline your experience with the Deltacare USA form. Complete the form carefully to avoid delays and ensure that you receive the specialist care you need.
Browse Other Templates
Business Personal Property Tax - Make sure all financial figures are accurate and up-to-date.
Rehabilitation Authorization Form,Vocational Training Certification,Veteran Educational Enrollment Document,Training Program Authorization Form,VA Rehabilitation Program Application,Veteran Status Certification Form,Chapter 31 Enrollment Certificatio - The VA relies on this form to issue timely payments for training costs.