Fill Out Your Erd 991 Form
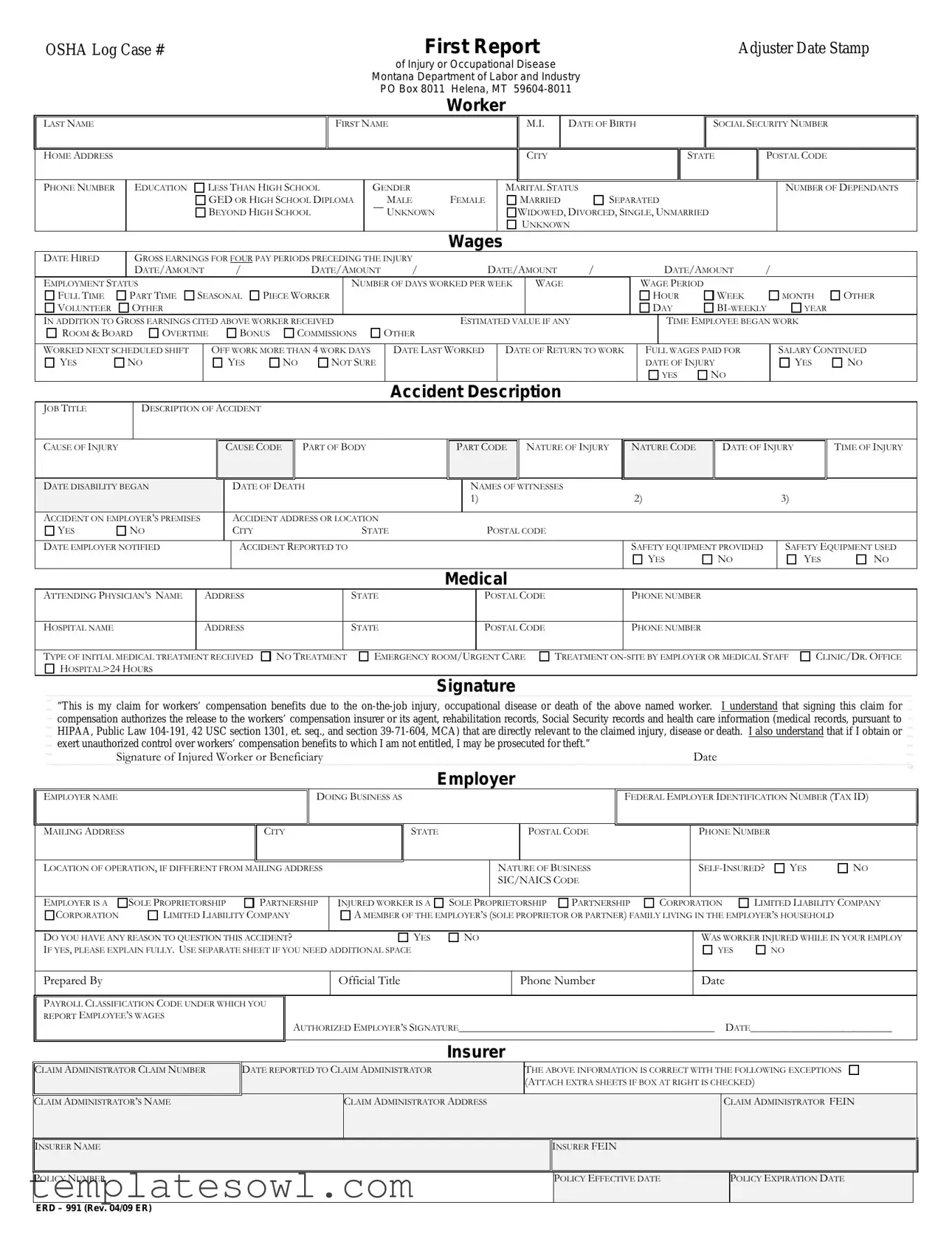
The ERD 991 form plays a crucial role in the workers' compensation process in Montana, capturing essential information related to workplace injuries, occupational diseases, and fatalities. This form is designed to be completed by both the injured worker and the employer, detailing pertinent information such as the worker's personal details, education level, and employment status. It includes sections for documenting the specifics of the injury, like the date, time, and cause, as well as an account of the accident itself. Additionally, the ERD 991 collects data on the medical treatment received, alongside any witnesses to the incident, fostering a thorough understanding of the circumstances surrounding each claim. Each section is purposefully crafted to ensure clarity and comprehensiveness, from capturing gross earnings to outlining the employer's obligations regarding safety equipment. The signature at the end of the form indicates the worker or beneficiary's acknowledgment of the claim and the implications of submitting false information. Understanding the ERD 991 is vital for all stakeholders in the workers' compensation system, ensuring that legitimate claims are processed efficiently and effectively while protecting both workers and employers alike.
Erd 991 Example
OSHA Log Case #
First Report |
Adjuster Date Stamp |
of Injury or Occupational Disease
Montana Department of Labor and Industry PO Box 8011 Helena, MT
Worker
LAST NAME
HOME ADDRESS
FIRST NAME
M.I. |
DATE OF BIRTH |
|
|
CITY |
|
|
|
SOCIAL SECURITY NUMBER
STATE |
POSTAL CODE |
|
|
PHONE NUMBER
EDUCATION
LESS THAN HIGH SCHOOL
GED OR HIGH SCHOOL DIPLOMA
BEYOND HIGH SCHOOL
GENDER
MALE
UNKNOWN
FEMALE
MARITAL STATUS
MARRIED 
 SEPARATED
SEPARATED
WIDOWED, DIVORCED, SINGLE, UNMARRIED
UNKNOWN
NUMBER OF DEPENDANTS
Wages
|
DATE HIRED |
|
GROSS EARNINGS FOR FOUR PAY PERIODS PRECEDING THE INJURY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
DATE/AMOUNT |
/ |
|
|
|
DATE/AMOUNT |
|
/ |
|
|
|
DATE/AMOUNT |
/ |
|
|
|
DATE/AMOUNT |
/ |
|
|
|||||||||||||
|
EMPLOYMENT STATUS |
|
|
|
|
|
|
|
|
|
|
|
NUMBER OF DAYS WORKED PER WEEK |
WAGE |
|
|
|
WAGE PERIOD |
|
|
|
|
|
|
|||||||||||
|
FULL TIME |
PART TIME |
SEASONAL |
PIECE WORKER |
|
|
|
|
|
|
|
|
|
|
|
|
|
HOUR |
|
WEEK |
|
|
MONTH |
OTHER |
|||||||||||
|
VOLUNTEER |
OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DAY |
|
YEAR |
|
||||||
|
IN ADDITION TO GROSS EARNINGS CITED ABOVE WORKER RECEIVED |
|
|
|
|
ESTIMATED VALUE IF ANY |
|
|
|
|
TIME EMPLOYEE BEGAN WORK |
|
|||||||||||||||||||||||
|
ROOM & BOARD |
OVERTIME |
|
|
|
BONUS |
|
COMMISSIONS |
OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
WORKED NEXT SCHEDULED SHIFT |
|
|
OFF WORK MORE THAN 4 WORK DAYS |
|
DATE LAST WORKED |
|
DATE OF RETURN TO WORK |
|
FULL WAGES PAID FOR |
|
|
SALARY CONTINUED |
||||||||||||||||||||||
|
YES |
NO |
|
|
|
|
|
YES |
|
NO |
NOT SURE |
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF INJURY |
|
|
YES |
NO |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accident Description |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
JOB TITLE |
|
DESCRIPTION OF ACCIDENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
CAUSE OF INJURY |
|
|
|
|
|
|
|
CAUSE CODE |
|
|
PART OF BODY |
|
|
|
PART CODE |
NATURE OF INJURY |
|
NATURE CODE |
|
DATE OF INJURY |
TIME OF INJURY |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE DISABILITY BEGAN |
|
|
|
|
|
|
DATE OF DEATH |
|
|
|
|
NAMES OF WITNESSES |
|
|
2) |
|
|
|
|
|
3) |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1) |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
ACCIDENT ON EMPLOYER’S PREMISES |
|
|
|
ACCIDENT ADDRESS OR LOCATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
YES |
NO |
|
|
|
|
|
|
CITY |
|
|
|
|
STATE |
|
|
|
|
POSTAL CODE |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
DATE EMPLOYER NOTIFIED |
|
|
|
|
|
|
ACCIDENT REPORTED TO |
|
|
|
|
|
|
|
|
|
|
|
SAFETY EQUIPMENT PROVIDED |
|
|
SAFETY EQUIPMENT USED |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
NO |
|
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medical
ATTENDING PHYSICIAN’S NAME |
ADDRESS |
|
STATE |
POSTAL CODE |
|
PHONE NUMBER |
|
|
|
|
|
|
PHONE NUMBER |
HOSPITAL NAME |
ADDRESS |
|
STATE |
POSTAL CODE |
|
|
|
|
|
|
|
|
|
TYPE OF INITIAL MEDICAL TREATMENT |
RECEIVED |
NO TREATMENT |
EMERGENCY ROOM/U |
RGENT CARE |
TREATMENT ON |
|
HOSPITAL>24 HOURS |
|
|
|
|
|
|
CLINIC/DR. OFFICE
Signature
“This is my claim for workers’ compensation benefits due to the
Signature of Injured Worker or Beneficiary |
Date |
Employer
EMPLOYER NAME
DOING BUSINESS AS
FEDERAL EMPLOYER IDENTIFICATION NUMBER (TAX ID)
MAILING ADDRESS |
|
CITY |
|
STATE |
|
|
|
POSTAL CODE |
|
PHONE NUMBER |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
LOCATION OF OPERATION, IF DIFFERENT FROM MAILING ADDRESS |
|
|
|
NATURE OF BUSINESS |
|
YES |
NO |
||||||||
|
|
|
|
|
|
|
SIC/NAICS CODE |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
LIMITED LIABILITY COMPANY |
||||
EMPLOYER IS A |
SOLE PROPRIETORSHIP |
PARTNERSHIP |
INJURED WORKER IS A |
SOLE P |
ROPRIETORSHIP |
PARTNERSHIP |
CORPORATION |
||||||||
CORPORATION |
LIMITED LIABILITY COMPANY |
A MEMBER OF THE EMPLOYER’S (SOLE PROPRIETOR OR PARTNER) FAMILY LIVING IN THE EMPLOYER’S HOUSEHOLD |
|
||||||||||||
|
|
|
|
|
|
|
|
WAS WORKER INJURED WHILE IN YOUR EMPLOY |
|||||||
DO YOU HAVE ANY REASON TO QUESTION THIS ACCIDENT? |
|
YES |
NO |
|
|
||||||||||
IF YES, PLEASE EXPLAIN FULLY. USE SEPARATE SHEET IF YOU NEED ADDITIONAL SPACE |
|
|
|
|
|
|
YES |
NO |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Prepared By |
|
|
|
Official Title |
|
|
|
Phone Number |
|
Date |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
PAYROLL CLASSIFICATION CODE UNDER WHICH YOU |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
REPORT EMPLOYEE’S WAGES |
|
AUTHORIZED EMPLOYER’S SIGNATURE_______________________________________________ |
DATE__________________________ |
||||||||||||
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurer
CLAIM ADMINISTRATOR CLAIM NUMBER
DATE REPORTED TO CLAIM ADMINISTRATOR
THE ABOVE INFORMATION IS CORRECT WITH THE FOLLOWING EXCEPTIONS (ATTACH EXTRA SHEETS IF BOX AT RIGHT IS CHECKED)
CLAIM ADMINISTRATOR’S NAME |
CLAIM ADMINISTRATOR ADDRESS |
|
CLAIM ADMINISTRATOR FEIN |
|
|
|
|
|
|
|
|
INSURER NAME |
|
INSURER FEIN |
|
|
|
|
|
|
|
|
|
POLICY NUMBER |
|
POLICY EFFECTIVE DATE |
|
POLICY EXPIRATION DATE |
|
|
|
|
|
|
|
ERD – 991 (Rev. 04/09 ER)
Form Characteristics
| Fact Name | Details |
|---|---|
| Form Purpose | The ERD 991 form is utilized to file a claim for workers' compensation benefits following an injury, occupational disease, or death that occurs on the job. |
| Governing Law | This form is subject to the laws of Montana, specifically under the Montana Workers' Compensation Act. |
| Injury Reporting | It requires detailed information about the injury, including timestamps for the accident and the initial medical treatment received. |
| Employee Information | The form collects comprehensive personal information about the injured worker, including their name, address, Social Security number, and employment details. |
| Employer Obligations | Employers must accurately complete sections of the form, affirming the nature of business and whether the employee was injured while working for them. |
| Signature Requirement | The injured worker or their beneficiary must sign the form, acknowledging the authorization for medical record releases and the seriousness of the claim. |
| Insurance Notification | Once completed, the ERD 991 form needs to be submitted to the insurance carrier or claims administrator within required deadlines to ensure timely processing of benefits. |
Guidelines on Utilizing Erd 991
Completing the ERD 991 form is an important step to ensure workers' compensation claims are processed accurately. This form collects essential information regarding the worker, the accident, and employer details that are crucial for determining eligibility for benefits.
- Obtain the ERD 991 form. Make sure you have access to a blank copy of the form, which can often be found online or requested from the appropriate agency.
- Fill in the OSHA Log Case number. Locate this section at the top of the form and write in the assigned case number.
- Provide details about the worker. Include the worker's last name, first name, middle initial, date of birth, social security number, home address, phone number, and education level.
- Indicate the worker's gender and marital status. Select one option from the provided choices for both categories.
- Input the number of dependents. State how many dependents the worker has.
- Enter wage information. Provide the gross earnings for the four pay periods preceding the injury, including the dates and amounts.
- Specify employment status. Determine and indicate the worker's employment status and wage period.
- Document any additional earnings. If applicable, list the estimated value of any benefits received besides gross earnings.
- State accident details. Fill out the date of injury, accident description, job title, cause of injury, part of the body affected, and nature of the injury.
- Complete the medical section. Provide the details of the attending physician and the type of medical treatment received.
- Sign the form. The injured worker or their beneficiary must sign and date the declaration regarding the claim.
- Fill in employer information. Include the employer's name, mailing address, and other requested details, such as their tax ID and nature of business.
- Complete insurer information. Provide details about the claim administrator and insurer, including their names and associated identifiers.
- Review the form. Before submission, double-check all sections for accuracy to prevent delays in processing.
What You Should Know About This Form
What is the purpose of the ERD 991 form?
The ERD 991 form is used to report a worker’s compensation claim due to an on-the-job injury or illness in Montana. This form collects essential information about the worker, the details of the incident, and the nature of the injury to facilitate the claims process with the appropriate authorities.
Who needs to fill out the ERD 991 form?
Both the injured worker and the employer need to complete relevant sections of the ERD 991 form. The injured worker provides personal information and details about the injury, while the employer verifies employment details and the circumstances of the injury.
When should the ERD 991 form be submitted?
The form should be submitted as soon as possible after the injury occurs. Prompt reporting helps ensure that the injured worker can receive timely medical treatment and potentially compensation for lost wages and medical expenses. Generally, it is advised to submit the form within 30 days after the injury.
What information is required from the worker on the ERD 991 form?
Workers need to provide several details, including their name, date of birth, Social Security number, home address, education level, number of dependents, work status, and details about the injury. Specifically, the form asks for the date of injury, a description of the accident, and the nature of the injury, among other things.
How does the employer contribute to the ERD 991 form?
The employer must supply information such as the business name, address, nature of business, employee classification, and details about the injury's circumstances. The employer also signs the form, confirming the accuracy of the provided information.
What if there are discrepancies in the information submitted?
If discrepancies occur in the information provided, the form allows for exceptions to be noted. If box for exceptions is checked, additional sheets should be attached to clarify what information is incorrect or needs additional explanation.
What happens after the ERD 991 form is submitted?
Once the ERD 991 form is submitted to the appropriate claims administrator, they will review the information and determine the eligibility of the worker for benefits. The claimant will then be contacted regarding any further steps, which may include medical examination or additional documentation requests.
Is there a way to check the status of the claim after submitting the ERD 991 form?
Yes, once the ERD 991 form is submitted, workers can follow up with the claim administrator or their employer to inquire about the status of their claim. The claim administrator typically contacts the worker for any updates or requirements that might arise during the review process.
What if the worker’s injury does not require medical treatment?
Even if no medical treatment is necessary, the ERD 991 form should still be filed if the injury occurred in the workplace. This ensures that there is a record of the incident in case complications arise later or if the worker needs to seek compensation for any future medical expenses related to the injury.
Are there any penalties for providing false information on the ERD 991 form?
Yes, providing false information on the ERD 991 form can lead to serious repercussions. Workers may face prosecution for theft or fraud if they receive benefits to which they are not entitled. Therefore, it’s crucial to accurately complete and sign the form.
Common mistakes
Filling out the ERD 991 form accurately is crucial for ensuring a smooth claims process in workers' compensation cases. However, many individuals make common mistakes that can lead to delays or denials of their claims. Understanding these errors can help improve the quality of submissions and facilitate a more efficient review by the relevant authorities.
One significant mistake involves providing incomplete or missing personal information. Essential details such as the worker's full name, social security number, and date of birth must be clearly filled out. An incomplete form may result in processing delays or the need for follow-up, potentially causing frustration for both the claimant and the claims administrator.
Another frequent error is related to the reporting of wages. Workers are expected to detail their gross earnings for the four pay periods prior to the injury accurately. Failure to include this information or miscalculating these figures can cause complications. It is important to provide precise amounts and to fill out all required fields, as even minor discrepancies may raise questions about the validity of the claim.
Additionally, individuals often overlook providing a thorough description of the accident. It is not enough to simply state that an injury occurred; the form requires a detailed account of the events leading to the injury, including the job title, cause of injury, and type of injury sustained. Vague or abbreviated descriptions can leave the claims administrator without the necessary context, leading to potential misunderstandings or disputes.
Moreover, not disclosing prior medical treatment can also create issues. When filling out the section on medical treatment, it is important to be honest and detailed about any medical care received related to the injury or occupational disease. Omitting this information can appear deceptive and could jeopardize the integrity of the claim.
Lastly, failing to obtain the required signatures can result in the rejection of the claim. All relevant parties, including the injured worker or beneficiary, and the employer, must sign the document. It is essential to double-check that signatures are present where necessary before submission, as a missing signature could halt the entire process.
Documents used along the form
The ERD 991 form is an essential document used in workers' compensation claims, specifically for reporting injuries or occupational diseases in Montana. Several other forms and documents frequently accompany the ERD 991 to ensure a thorough process for both the injured worker and the employer. The following list outlines these additional documents.
- First Report of Injury (FROI): This form provides initial details about the employee's injury, including the circumstances surrounding it, and is typically required for the claims process.
- Claimant's Authorization for Release of Medical Records: This document allows medical providers to share the injured worker's health information with the insurer, ensuring relevant medical history is used in the claim review.
- Proof of Employment: This may include pay stubs or an employment verification letter confirming the worker's job title, duties, and wages, which supports the compensation claim.
- Medical Reports: Detailed reports from healthcare providers that outline the diagnosis, treatment, and recovery expectations are crucial to determining the extent of the injury and necessary benefits.
- Witness Statements: Testimonies from colleagues or bystanders who observed the incident can be influential in validating the claim and the circumstances surrounding the injury.
- Employer's Report of Injury: This document, completed by the employer, details their account of the accident, emphasizing their perspective and any safety measures in place at the time.
- Return to Work Form: This form indicates when the injured worker is authorized to resume their job, often including any limitations or modifications to their duties due to the injury.
- Workers' Compensation Claim File Documents: These can include notes, correspondence, and additional paperwork related to the claim filed with the court or insurance carrier, aiding in the full understanding of the case.
- Rehabilitation Services Authorization: If applicable, this form allows for access to rehabilitation services, which can assist workers in recovering and returning to work effectively.
These forms and documents help create a comprehensive view of the injury, ensuring all parties are informed and that the workers' compensation claim is processed effectively. Proper documentation supports the worker’s rights and the employer's responsibilities in handling such claims.
Similar forms
-
First Report of Injury (FROI): This document serves as an initial notification of an injury or occupational disease to the workers' compensation system. Similar to the ERD 991 form, both collect details about the injured worker, the nature of the injury, and circumstances surrounding the event.
-
OSHA Incident Report: Like the ERD 991, this report documents work-related injuries or illnesses. It provides a record of incidents that occurred in the workplace, focusing on safety compliance and prevention measures.
-
Workers' Compensation Claim Form: This form is used by employees to apply for benefits. Both the claim form and the ERD 991 ask for similar information about the worker’s background, injury specifics, and employer details.
-
Medical Treatment Records: These records document the medical care provided to injured workers. They align with the ERD 991 as both require information about the attending physician and the type of treatment received after an injury.
Dos and Don'ts
When filling out the ERD 991 form, attention to detail is crucial. This form is a vital document for claiming workers’ compensation benefits, so taking care to follow proper guidelines is essential. Here’s a list of things you should and shouldn't do while completing it:
- Do double-check all personal information for accuracy, including name, address, and Social Security number.
- Do provide detailed information about the injury or illness. Be clear in your accident description and the nature of the injury.
- Do include all relevant dates, such as the date of injury, the date you last worked, and the expected date to return to work.
- Do ensure the signature is present at the end of the form, indicating your understanding and agreement of the claim.
- Do attach any necessary documentation that may support your claim, such as medical records or witness statements.
- Don't leave any sections blank. Every part of the form must be filled out to avoid delays in processing.
- Don't use abbreviations or shorthand that may not be understood by others reviewing your claim.
- Don't provide false information or exaggerate details; this can lead to serious consequences.
- Don't forget to keep a copy of the completed form for your personal records.
- Don't rush through the form; take your time to ensure all details are correct and complete.
By following these dos and don’ts, you can help ensure that your form is completed correctly and that your claim is processed smoothly.
Misconceptions
- Misconception 1: The ERD 991 form is only for severe injuries.
- Misconception 2: Only employees can use the ERD 991 form.
- Misconception 3: The ERD 991 form needs to be submitted immediately after an injury.
- Misconception 4: All medical treatments must be reported on the form.
- Misconception 5: The form guarantees compensation.
- Misconception 6: The ERD 991 form is complicated and long.
- Misconception 7: Incomplete forms automatically lead to rejection.
- Misconception 8: The employer is responsible for filling out the entire form.
This form is applicable for any work-related injury or occupational disease, regardless of severity. It serves to document all types of incidents.
While the form is primarily for employees, it can also be utilized by dependents of a deceased worker seeking benefits or compensation related to a workplace incident.
While timely reporting is important, there may be specific deadlines that vary by state or employer. Delays can be acceptable, but prompt action is encouraged to ensure proper processing.
Only treatments related to the injury or disease at hand need to be documented. General medical treatments unrelated to the case are not necessary.
Filing the ERD 991 form initiates the claims process, but it does not automatically result in compensation. Each claim is reviewed on its merits before a decision is made.
Although the form involves several sections, many are straightforward. Each part aims to gather relevant information efficiently. Attention to detail ensures accurate submissions.
While thoroughness is crucial, many jurisdictions allow for corrections or additional information submissions. It is wise to ensure all sections are filled to avoid issues.
Both the worker and employer have roles in completing the ERD 991 form. Workers provide personal details, while employers fill in information about the business and incident.
Key takeaways
When filling out and using the Erd 991 form, there are several important points to consider:
- The form is used for reporting workplace injuries and occupational diseases to the Montana Department of Labor and Industry.
- Accurate details of the injured worker must be provided, including their full name, date of birth, and social security number.
- Information regarding the worker’s employment status, such as full-time or part-time, must be clearly indicated.
- Gross earnings for the four pay periods prior to the injury should be documented carefully.
- Complete the accident description section to provide clarity about what happened. Include the job title and the cause of the injury.
- The date and time of the injury, as well as the subsequent medical treatment details, must be captured accurately.
- Witness information is critical. If there are others who saw the accident, their names should be listed.
- Obtain the necessary signatures from the injured worker or beneficiary. This formally submits the claim.
- Ensure that the employer’s information, including name and address, is filled out correctly.
- Review the completed form for any errors or missing information before submission to avoid delays in processing the claim.
Utilizing the Erd 991 form correctly helps ensure that claims for workers' compensation benefits are processed efficiently.
Browse Other Templates
Wrap Around Mortgage - This instrument is a significant part of multi-party real estate transactions.
Job Search Activity Log,Work Search Contact Record,Employment Search Tracking Form,Job Hunt Documentation Sheet,Work Seeking Record,Employment Inquiry Log,Job Application Contact Sheet,Work Search Reporting Form,Job Search Progress Tracker,Employment - Reached out to a recruiter through LinkedIn for job leads.