Fill Out Your First Report Of Injury Florida Form
When an employee suffers an injury or illness in the workplace in Florida, prompt reporting is essential for ensuring that their rights and benefits are protected. Completing the First Report of Injury form is a crucial step in this process. This form not only captures vital details about the incident, such as the employee's name, Social Security number, and occupation, but also provides essential information regarding the nature of the accident, including the time and place it occurred and the part of the body affected. Employers are required to fill this form out accurately, as it serves as a key document in the Workers' Compensation system. Additionally, it helps to determine whether the employee will receive wage replacement and what medical assistance is necessary. Notably, the form also includes sections to document the employer's details and actions taken following the incident, ensuring compliance with state regulations. Submitting this document triggers the claims process so that affected employees can receive the support they need promptly.
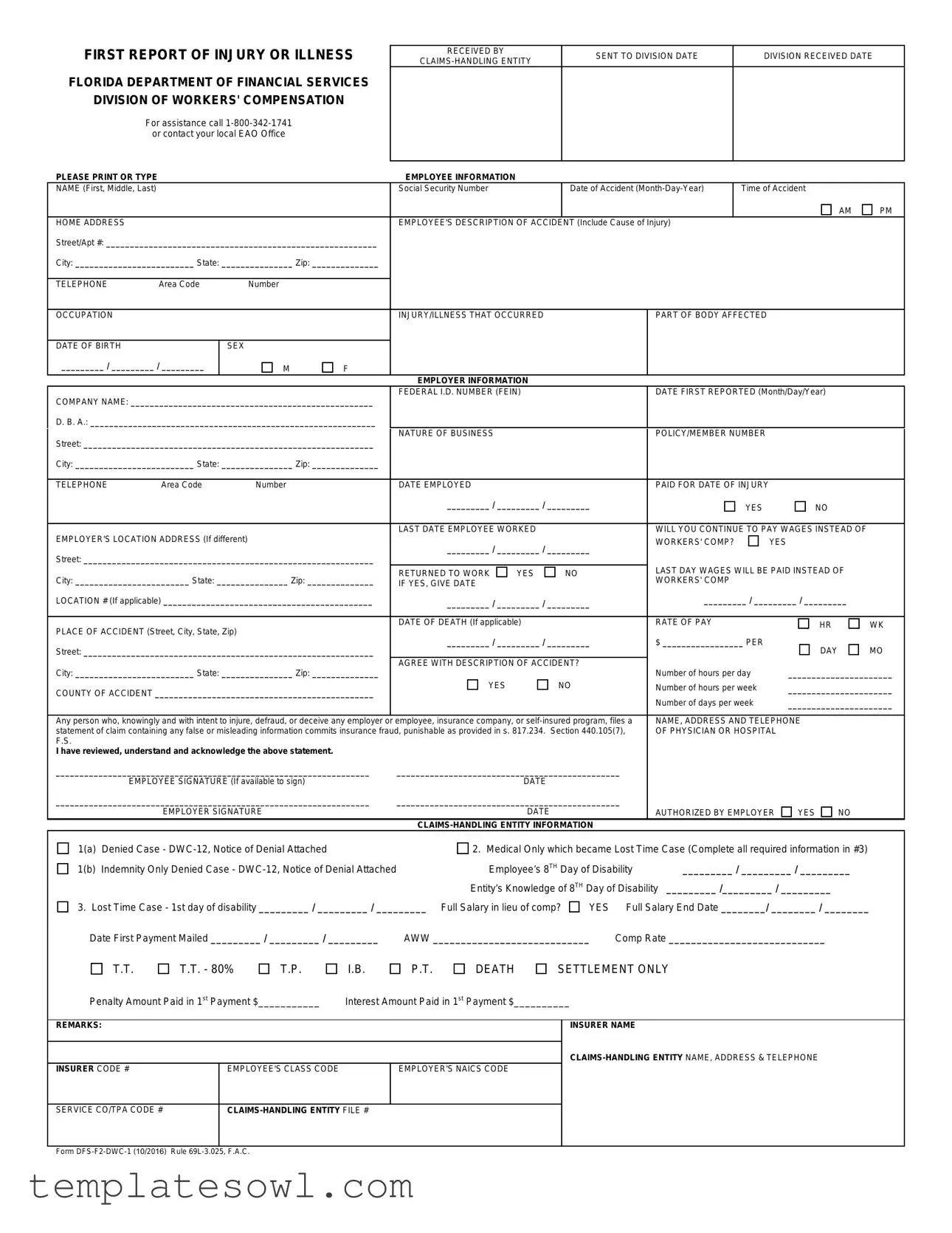
First Report Of Injury Florida Example
FIRST REPORT OF INJURY OR ILLNESS
FLORIDA DEPARTMENT OF FINANCIAL SERVICES
DIVISION OF WORKERS' COMPENSATION
For assistance call
PLEASE PRINT OR TYPE
RECEIVED BY |
SENT TO DIVISION DATE |
DIVISION RECEIVED DATE |
|
|
|
||
|
|
|
EMPLOYEE INFORMATION
NAME (First, Middle, Last) |
|
|
|
Social Security Number |
|
|
Date of Accident |
|
Time of Accident |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
AM |
PM |
HOME ADDRESS |
|
|
|
EMPLOYEE'S DESCRIPTION OF ACCIDENT (Include Cause of Injury) |
|
|
|
|
|||||
Street/Apt #: _________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|||
City: _________________________ State: _______________ Zip: ______________ |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
Area Code |
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
OCCUPATION |
|
|
|
INJURY/ILLNESS THAT OCCURRED |
|
|
PART OF BODY AFFECTED |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
|
SEX |
|
|
|
|
|
|
|
|
|
|
|
_________ / _________ / _________ |
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYER INFORMATION |
|
|
|
|
|
|
|
|
|
COMPANY NAME: ___________________________________________________ |
FEDERAL I.D. NUMBER (FEIN) |
|
|
DATE FIRST REPORTED (Month/Day/Year) |
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||
D. B. A.: ____________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|||
Street: _____________________________________________________________ |
NATURE OF BUSINESS |
|
|
|
POLICY/MEMBER NUMBER |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||
City: _________________________ State: _______________ Zip: ______________ |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||
TELEPHONE |
Area Code |
Number |
|
DATE EMPLOYED |
|
|
|
PAID FOR DATE OF INJURY |
|
|
|
||
|
|
|
|
_________ / _________ / _________ |
|
|
YES |
|
NO |
|
|||
|
|
|
|
|
|
|
|
|
|
||||
EMPLOYER'S LOCATION ADDRESS (If different) |
|
LAST DATE EMPLOYEE WORKED |
|
|
WILL YOU CONTINUE TO PAY WAGES INSTEAD OF |
|
|||||||
|
_________ / _________ / _________ |
WORKERS' COMP? |
|
YES |
|
||||||||
|
|
|
|
|
|
||||||||
Street: _____________________________________________________________ |
|
|
|
|
|
|
|||||||
|
|
|
|
LAST DAY WAGES WILL BE PAID INSTEAD OF |
|
||||||||
|
|
|
|
RETURNED TO WORK |
YES |
|
NO |
|
|||||
City: ________________________ State: _______________ Zip: ______________ |
|
WORKERS' COMP |
|
|
|
|
|||||||
IF YES, GIVE DATE |
|
|
|
|
|
|
|
||||||
LOCATION # (If applicable) ____________________________________________ |
_________ / _________ / _________ |
_________ / _________ / _________ |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
RATE OF PAY |
|
|
|
|
||
PLACE OF ACCIDENT (Street, City, State, Zip) |
|
DATE OF DEATH (If applicable) |
|
|
|
|
HR |
WK |
|||||
|
|
|
|
|
|
|
|
|
|||||
|
_________ / _________ / _________ |
$ _________________ PER |
|
|
|
||||||||
Street: _____________________________________________________________ |
|
DAY |
MO |
||||||||||
|
|
|
|
|
|
|
|
||||||
City: _________________________ State: _______________ Zip: ______________ |
AGREE WITH DESCRIPTION OF ACCIDENT? |
Number of hours per day |
______________________ |
||||||||||
|
|
|
|
||||||||||
COUNTY OF ACCIDENT ______________________________________________ |
YES |
|
NO |
Number of hours per week |
______________________ |
||||||||
|
|
|
|
Number of days per week |
______________________ |
||||||||
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|||||||||
Any person who, knowingly and with intent to injure, defraud, or deceive any employer or |
employee, insurance company, or |
NAME, ADDRESS AND TELEPHONE |
|
||||||||||
statement of claim containing any false or misleading information commits insurance fraud, punishable as provided in s. 817.234. Section 440.105(7), |
OF PHYSICIAN OR HOSPITAL |
|
|||||||||||
F.S. |
|
|
|
|
|
|
|
|
|
|
|
|
|
I have reviewed, understand and acknowledge the above statement.
__________________________________________________________________ |
_______________________________________________ |
|
|
|
|||
|
EMPLOYEE SIGNATURE (If available to sign) |
DATE |
|
|
|
|
|
__________________________________________________________________ |
_______________________________________________ |
|
|
|
|||
|
EMPLOYER SIGNATURE |
DATE |
|
AUTHORIZED BY EMPLOYER |
YES |
NO |
|
|
|
|
|
|
|
||
1(a) |
Denied Case - |
2. Medical Only which became Lost Time Case (Complete all required information in #3) |
|||||
1(b) |
Indemnity Only Denied Case - |
Employee’s 8TH Day of Disability |
_________ / _________ / _________ |
||||
|
|
Entity’s Knowledge of 8TH Day of Disability |
_________ /_________ / _________ |
|
|||
3. Lost Time Case - 1st day of disability _________ / _________ / _________ Full Salary in lieu of comp? |
YES |
Full Salary End Date ________/ ________ / ________ |
|||||
Date First Payment Mailed _________ / _________ / _________ |
AWW ____________________________ |
Comp Rate ____________________________ |
|
||||
T.T.
T.T. - 80%
T.P.
I.B.
P.T.
DEATH
SETTLEMENT ONLY
Penalty Amount Paid in 1st Payment $___________ |
Interest Amount Paid in 1st Payment $__________ |
REMARKS:
INSURER CODE # |
EMPLOYEE'S CLASS CODE |
EMPLOYER'S NAICS CODE |
|
|
|
INSURER NAME
SERVICE CO/TPA CODE #
Form
The collection of the social security number on this form is specifically authorized by Section 440.185(2), Florida Statutes. The social security number will be used as a unique identifier in Division of Workers' Compensation database systems for individuals who have claimed benefits under Chapter 440, Florida Statutes. It will also be used to identify information and documents in those database systems regarding individuals who have claimed benefits under Chapter 440, Florida Statutes, for internal agency tracking purposes and for purposes of responding to both public records requests and subpoenas that require production of specified documents. The social security number may also be used for any other purpose specifically required or authorized by state or federal law.
Form Characteristics
| Fact Name | Description |
|---|---|
| Governing Law | The form is governed by Florida Statutes Chapter 440, which pertains to workers' compensation. |
| Purpose | This form is used to report work-related injuries or illnesses to the Florida Division of Workers' Compensation. |
| Contact Information | For assistance, individuals can call 1-800-342-1741 or contact their local Employee Assistance Office. |
| Social Security Number | The collection of Social Security Numbers is authorized under Section 440.185(2), Florida Statutes. |
| Employee Information Required | Essential details include the employee's name, Social Security Number, date of the accident, and a description of the incident. |
| Employer Information Required | Companies must provide their name, Federal ID number, nature of business, and contact information. |
| Claims-Handling Entity | Details pertaining to the claims-handling entity must be included, such as their name and contact information. |
| Fraud Warning | The form includes a warning regarding the serious consequences of committing workers' compensation fraud, as outlined in Section 440.105(7), Florida Statutes. |
Guidelines on Utilizing First Report Of Injury Florida
Once the First Report of Injury form in Florida is completed, it should be submitted to the relevant claims-handling entity for processing. This initial step is critical for ensuring that claims are handled efficiently and accurately, allowing both employees and employers to move forward in the event of an injury or illness.
- Obtain the Form: Download the First Report of Injury form from the Florida Department of Financial Services website or your employer’s resources.
- Print or Type: Fill out the form using clear print or type all required information. This ensures readability and prevents errors.
- Complete Employee Information: Start by entering the employee's full name, social security number, date and time of the accident, and home address, including city, state, and zip code.
- Description of the Accident: Provide a detailed account of the incident, including the cause of the injury, telephone number, occupation, type of injury or illness, and part of the body affected.
- Employee Personal Details: Record the employee's date of birth and sex.
- Employer Information: Fill in the company name, federal I.D. number, date first reported, "doing business as" (D.B.A.) name, and address along with the nature of the business and policy/member number.
- Employment Details: Specify the date the employee was hired, if they were paid for the date of injury, and the location address of the employer if it differs from the main address.
- Payment Information: Indicate if the employer will continue paying wages instead of workers' compensation and provide the last date wages will be paid.
- Place of Accident: Enter the street, city, state, and zip code where the accident occurred, along with details about the employee’s rate of pay.
- Accident Affirmation: Check the appropriate box to indicate if there is agreement with the description of the accident.
- Complete Physician Information: Provide the name, address, and telephone number for any physician or hospital that treated the employee.
- Signatures: If available, the employee should sign and date the form. The employer or an authorized individual should also sign and date the form confirming their approval.
- Claims-Handling Entity Information: Fill out any relevant information pertaining to claims handling as per your situation, including denied cases or lost time cases.
- Review: Before submitting, review the completed form for accuracy and completeness to prevent any delays in processing.
- Submit the Form: Send the completed form to the relevant claims-handling entity as per your company protocols.
What You Should Know About This Form
What is the First Report Of Injury Florida form?
The First Report Of Injury Florida form is a document used to report work-related injuries or illnesses to the Florida Division of Workers' Compensation. It collects essential information about the employee, the incident, and the employer. This report is a critical step in initiating a claim for workers' compensation benefits in Florida.
Who needs to complete the First Report Of Injury Florida form?
The form must be completed by the employer or their claims-handling entity when an employee suffers a work-related injury or illness. Employees may also provide input on the description of the accident section. Accurate information is crucial for claims processing and to ensure compliance with state regulations.
What information is required on the form?
The form requires details about the employee, including name, social security number, date of birth, and home address. Information about the accident, such as the date, time, and place of the injury, is also necessary. The employer must provide their company name and employee's occupation. Additionally, data about the nature of the injury and the affected body part should be provided.
How is the information used once submitted?
The submitted information is used by the Florida Division of Workers' Compensation to track claims and manage employees' benefits. It serves as a unique identifier for each claimant. The information aids in processing benefits under Chapter 440 of Florida Statutes and can also be utilized in response to public records requests and subpoenas.
What should be done if the form contains inaccurate information?
If there is any inaccurate information on the form, it may lead to delays or denials of claims. It is advisable to contact the claims-handling entity immediately to rectify any errors. Prompt communication can help ensure that the claim remains valid and that the necessary benefits are received without interruption.
What are the consequences of providing false information on the form?
Providing false information on the First Report Of Injury Florida form is considered insurance fraud. Florida law imposes penalties for any individual who intentionally submits misleading information with the intent to deceive. Such actions can lead to criminal prosecution and may have further implications for the individual's ability to receive benefits.
Common mistakes
Filling out the First Report Of Injury Florida form can be a crucial aspect of initiating a workers' compensation claim. However, people often make mistakes that can delay the process or even jeopardize their claims. One common error is providing an incomplete description of the accident. When detailing how the injury occurred, it is essential to include all relevant information, such as the cause and the exact circumstances. An ambiguous description may lead to questions or disputes later on, complicating the claim further.
Another frequent oversight is failing to report the injury within the required time frame. The date of the accident must be accurately recorded in the designated field. Timing is critical; delays in reporting can lead to a denial of the claim. Similarly, neglecting to include personal information, such as the correct social security number, may hinder the processing of the claim. It is vital to double-check these details to ensure accuracy and completeness.
Providing inaccurate employer information poses another significant risk. The company name, federal I.D. number, and the nature of the business should be accurately stated. Missing or incorrectly stated employer details can lead to delays in review and may even trigger additional questions about the legitimacy of the claim. Furthermore, individuals sometimes overlook their employment details, such as the date first reported and the last date worked. These dates are crucial for establishing the timeline of events and should be completed precisely.
Another mistake is failing to specify the part of the body affected by the injury. Indicating this clearly on the form helps in the assessment of the claim. Garden-variety descriptors may not suffice, and it is best to be as explicit as possible, detailing whether multiple areas were impacted. Additionally, answering yes or no questions incorrectly can create misunderstandings. For instance, if you indicate that the employer will continue to pay wages instead of workers' compensation without confirming it, you could set up a mismatch in expectations later on.
People sometimes make the mistake of rushing through the employer’s location information. Ensuring that this address is complete and correctly entered is essential for the claims-handling entity to verify information. Finally, individuals may neglect to review the form for possible omissions. Such reviewers should check not only for missing information but also for typos or data that may clash with other details provided. Taking the time to scrutinize the document ensures all information aligns and strengthens the case.
Documents used along the form
In the process of filing a workers' compensation claim in Florida, various forms and documents complement the First Report of Injury. Each of these documents serves a distinct role in ensuring that all relevant information is captured and processed effectively. Below is a list of commonly used documents.
- DWC-12, Notice of Denial: This document is used when an insurance claim is denied. It outlines the reasons for denial and is essential for the employee to understand why their claim may not be paid.
- Medical Authorization Form: This form permits medical providers to share the employee’s medical information with the insurance company, which is necessary to assess the injury.
- Claim for Compensation (Form DFS-F2-DWC-1): This form is typically used to file a formal claim for workers’ compensation benefits after an injury occurs, ensuring compliance with state requirements.
- Employee’s Sworn Statement: This statement provides a detailed description of the accident and the resulting injuries. It is critical for establishing the context of the claim.
- Medical Bills and Records: These documents provide a record of the treatments received by the employee, including costs, which are necessary for reimbursement and benefits calculations.
- Return-to-Work Notice: This form is used when an employee is ready to resume work after an injury. It ensures that the employer and insurer are aware of the employee’s status.
- Wage Statements: These documents reflect the employee’s earnings prior to the injury. They are used to calculate compensation rates for benefits.
Each of these forms plays a vital role in navigating the complexities of workers' compensation processes. Understanding their purposes can make the filing and claims experience smoother for all parties involved.
Similar forms
The First Report Of Injury Florida form is essential for workers' compensation claims. It shares similarities with several other important documents. Here are seven documents that are comparable and how they relate:
- OSHA Form 301: This form helps in reporting workplace injuries and illnesses. Like the Florida form, it outlines details about the employee, the injury, and how it occurred.
- Employer's Report of Injury or Illness: This document captures the employer's perspective on the incident, similar to the employer information section of the Florida form, ensuring a comprehensive view of the injury.
- Florida DWC-12, Notice of Denial: If a claim is denied, this form must be filled out. Both documents are critical for tracking the progress of a claim and the reasons behind denial.
- Claim Adjustment Notice: Issued by insurance companies, this notice details any adjustments made to a claim, like payment amounts. The First Report helps set the stage for these adjustments.
- Medical Authorization Form: This form allows insurers to obtain medical records. Both documents emphasize the need for thorough documentation in the claims process.
- Independent Medical Examination (IME) Report: An IME assesses the extent of an injury, linking back to the specifics gathered in the First Report regarding injury details and effects on the employee.
- Final Settlement Agreement: This document finalizes a workers' compensation claim. The First Report kickstarts the process leading to potential settlement agreements and claims resolution.
Dos and Don'ts
When filling out the First Report of Injury form in Florida, following certain dos and don'ts can ensure accurate reporting, leading to timely processing and fewer complications. Here’s a list of what to keep in mind:
- DO provide complete and accurate information. This includes details about the incident, your employer, and your injury.
- DO print or type your answers clearly. Easy-to-read information can prevent misunderstandings and processing delays.
- DO include your Social Security number. It serves as a unique identifier in the workers' compensation system.
- DO double-check the dates. Make sure the date of the accident and other dates are correct to avoid confusion.
- DON'T leave any sections blank. If a section doesn’t apply, indicate that it is not applicable rather than omitting it.
- DON'T provide false or misleading information. This can lead to serious consequences, including potential fraud charges.
- DON'T forget to sign the form. An unsigned form may lead to delays or denial of your claim.
- DON'T submit the form without keeping a copy for your records. This can be useful if there are any questions or disputes later on.
Following these guidelines will not only make the process smoother for you but also help your employer and the insurance company process your claim efficiently. Stay informed about your rights and responsibilities when it comes to work-related injuries in Florida.
Misconceptions
Misconceptions about the First Report of Injury Florida form can lead to confusion and mismanagement of claims. Here are six common myths and the truths behind them:
- It’s only for severe injuries. Many believe this form is only necessary for serious accidents. In reality, all workplace injuries, no matter how minor, should be reported using this form to ensure proper documentation.
- Completing the form is optional. Some assume that submitting this report is at the employer’s discretion. However, Florida law mandates this report for all workplace injuries to ensure that employees can receive the benefits they deserve.
- The employee must fill it out themselves. There is a belief that only the injured employee can complete the form. However, employers or designated representatives can assist or fill it out on behalf of the employee if necessary.
- It must be submitted immediately after the injury. While timely reporting is important, some think the form must be submitted before any medical attention. In truth, the form should be completed as soon as possible after the injury and can follow medical evaluation.
- The information in the form is secret. Some people think the details shared in this report are confidential and never shared. While personal information is protected, the data may be subject to disclosure under certain legal circumstances.
- The form is just for insurance purposes. A common misconception is that this form serves only the insurance companies. It also establishes a record with the state’s Division of Workers’ Compensation, which monitors workplace injuries and compliance with the law.
Understanding these misconceptions helps ensure proper filing and management of injury reports, ultimately benefiting both employees and employers in Florida.
Key takeaways
Here are key takeaways about filling out and using the First Report of Injury Florida form:
- Accurate Information: Ensure all employee and employer information is filled out accurately, including names, addresses, and Social Security numbers.
- Claim Timeliness: Submit the form promptly after the injury, as timely reporting is crucial for workers' compensation claims.
- Description of Accident: Provide a clear and detailed description of how the injury occurred. This helps in assessing the claim.
- Signature Requirements: Obtain signatures from both the employee and employer where indicated, as these affirm the details provided.
- Check for Completeness: Verify that all fields are completed before submission to avoid processing delays.
- Medical Information: Note any medical treatment received and ensure it aligns with the injury reported.
- Fraud Awareness: Understand that providing false information can result in penalties and legal consequences.
- Employee's Rights: Employees have the right to file a claim for benefits if injured while working, and this form is a crucial part of that process.
- Form Submission: Submit the completed form to the appropriate claims-handling entity within your organization for processing.
Browse Other Templates
Executor Deed Example - Notaries play a critical role in validating the execution of an Executor Deed to prevent fraud.
Fictitious Business Name Renewal Form,Fictitious Name Permit Renewal Notification,California Fictitious Name Update Application,Permit Renewal for Fictitious Medical Practice,Fictitious Name Permit Hold Release Form,California Fictitious Name Mainten - The Medical Board's phone and fax numbers are provided for inquiries about the form.