Fill Out Your Food Stamp Nc Form
The Food Stamp NC form, officially known as the Notice of Expiration and Recertification Form, plays a crucial role in ensuring that eligible households in North Carolina have access to Food and Nutrition Services (FNS) benefits. This form includes essential sections where individuals are asked to provide personal information, such as their name and address, along with details about their household members. It is important to complete this form accurately, as it may affect your benefits. Timelines for submission are clearly indicated, including a due date by which the form must be returned to continue receiving assistance. Notably, the form recognizes the need for accessibility—resources for language assistance and accommodations for individuals with disabilities are available. Applicants must provide verification of income and expenses to demonstrate eligibility, and supporting documents should be attached when submitting the form. By engaging with this process, households affirm their commitment to following the rules set out by the FNS. Completing this paperwork accurately helps maintain the integrity of the program, ensuring that those in genuine need continue to receive support. Moreover, detailed inquiries about citizenship and Social Security numbers reflect the importance of compliance with federal guidelines. Understanding and following these instructions is essential for a smooth recertification process.
Food Stamp Nc Example
DSS Street Address: |
Case Identifier: ________________________ |
________________________ |
Worker: ______________________________ |
________________________ |
Date Generated: _______________________ |
|
Due Date: _____________________________ |
DSS Mailing address: |
Client Name: __________________________ |
________________________ |
Mailing Address: _______________________ |
________________________ |
_______________________ |
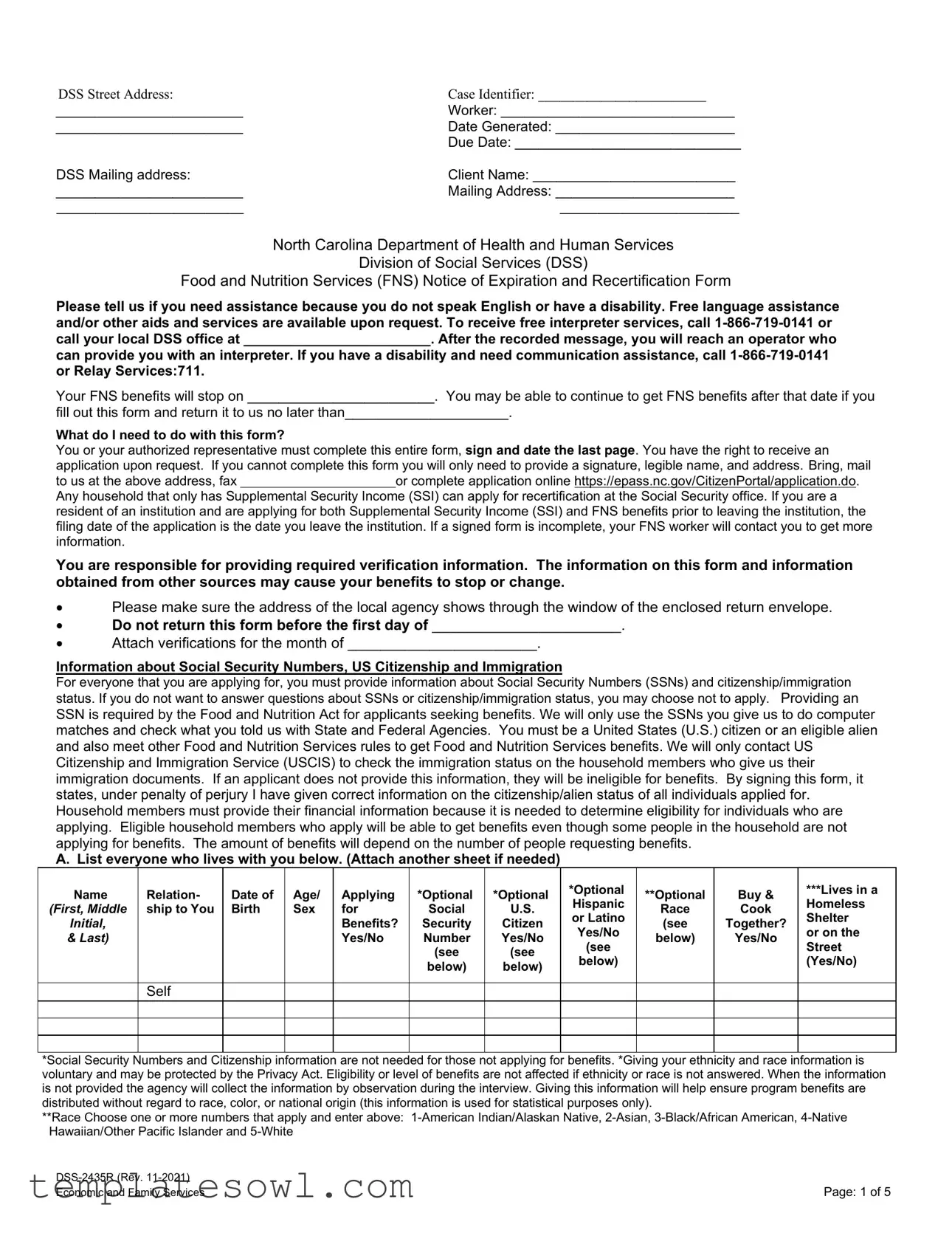
North Carolina Department of Health and Human Services
Division of Social Services (DSS)
Food and Nutrition Services (FNS) Notice of Expiration and Recertification Form
Please tell us if you need assistance because you do not speak English or have a disability. Free language assistance and/or other aids and services are available upon request. To receive free interpreter services, call
can provide you with an interpreter. If you have a disability and need communication assistance, call
Your FNS benefits will stop on ________________________. You may be able to continue to get FNS benefits after that date if you
fill out this form and return it to us no later than_____________________.
What do I need to do with this form?
You or your authorized representative must complete this entire form, sign and date the last page. You have the right to receive an application upon request. If you cannot complete this form you will only need to provide a signature, legible name, and address. Bring, mail
to us at the above address, faxor complete application online https://epass.nc.gov/CitizenPortal/application.do. Any household that only has Supplemental Security Income (SSI) can apply for recertification at the Social Security office. If you are a resident of an institution and are applying for both Supplemental Security Income (SSI) and FNS benefits prior to leaving the institution, the filing date of the application is the date you leave the institution. If a signed form is incomplete, your FNS worker will contact you to get more information.
You are responsible for providing required verification information. The information on this form and information obtained from other sources may cause your benefits to stop or change.
•Please make sure the address of the local agency shows through the window of the enclosed return envelope.
•Do not return this form before the first day of _______________________.
•Attach verifications for the month of _______________________.
Information about Social Security Numbers, US Citizenship and Immigration
For everyone that you are applying for, you must provide information about Social Security Numbers (SSNs) and citizenship/immigration status. If you do not want to answer questions about SSNs or citizenship/immigration status, you may choose not to apply. Providing an SSN is required by the Food and Nutrition Act for applicants seeking benefits. We will only use the SSNs you give us to do computer matches and check what you told us with State and Federal Agencies. You must be a United States (U.S.) citizen or an eligible alien and also meet other Food and Nutrition Services rules to get Food and Nutrition Services benefits. We will only contact US Citizenship and Immigration Service (USCIS) to check the immigration status on the household members who give us their immigration documents. If an applicant does not provide this information, they will be ineligible for benefits. By signing this form, it states, under penalty of perjury I have given correct information on the citizenship/alien status of all individuals applied for. Household members must provide their financial information because it is needed to determine eligibility for individuals who are applying. Eligible household members who apply will be able to get benefits even though some people in the household are not applying for benefits. The amount of benefits will depend on the number of people requesting benefits.
A. List everyone who lives with you below. (Attach another sheet if needed)
Name |
Relation- |
Date of |
Age/ |
Applying |
*Optional |
*Optional |
*Optional |
**Optional |
Buy & |
***Lives in a |
|
Hispanic |
Homeless |
||||||||||
(First, Middle |
ship to You |
Birth |
Sex |
for |
Social |
U.S. |
Race |
Cook |
|||
or Latino |
Shelter |
||||||||||
Initial, |
|
|
|
Benefits? |
Security |
Citizen |
(see |
Together? |
|||
|
|
|
Yes/No |
or on the |
|||||||
& Last) |
|
|
|
Yes/No |
Number |
Yes/No |
below) |
Yes/No |
|||
|
|
|
(see |
Street |
|||||||
|
|
|
|
|
(see |
(see |
|
|
|||
|
|
|
|
|
below) |
|
|
(Yes/No) |
|||
|
|
|
|
|
below) |
below) |
|
|
|||
|
|
|
|
|
|
|
|
|
Self
*Social Security Numbers and Citizenship information are not needed for those not applying for benefits. *Giving your ethnicity and race information is voluntary and may be protected by the Privacy Act. Eligibility or level of benefits are not affected if ethnicity or race is not answered. When the information is not provided the agency will collect the information by observation during the interview. Giving this information will help ensure program benefits are distributed without regard to race, color, or national origin (this information is used for statistical purposes only).
**Race Choose one or more numbers that apply and enter above:
Page: 1 of 5 |
|
Economic and Family Services |
***These questions may assist in identifying
B. Tell us about your finances.
***1. Does anyone in your household work? Yes No If yes, complete below.
***2. Is anyone in your household getting ready to start a job? Yes No If yes, expected start date_________ and complete below.
Attach all income verification pay received during the month listed on Page 1. If you are paid monthly, attach income verification for the month listed on Page 1. If you are
If you do not have all your check stubs, you may have your employer complete the employer verification section below. (Attach another sheet if needed)
Name of Person Working: |
|
|
How Often Paid: (weekly/month, etc.) |
|
||
|
|
|
|
|
|
|
Employer Name: |
|
|
Employer Phone Number: |
|
||
|
|
|
|
|
|
|
Date Pay Received |
Number of |
Rate of |
Bonus or Vacation |
Gross Pay |
|
Tips |
(month & day) |
Hours |
Pay |
Pay |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer Signature: |
Employer Title: |
Date Signed: |
|
***3. Has anyone in your household stopped working within the last 6 months? Yes No If yes, who stopped working? __________ |
||
Reason? _________________Date last worked? _______ Date of last pay? ________ Total hours worked in last 30 days? ______
***4. Does anyone in your household get money other than from work? Yes No If yes, complete below and attach verification for month listed on page 1. Examples: Cash, Contributions, Work First, Child Support, Unemployment Benefits, Social Security, SSI, Worker’s Compensation, Veteran’s Benefits, etc. (attach another sheet if needed)
Name
Type of Income |
Person or Organization |
Phone Number and Address |
Amount of Income |
|
That Gives the Money |
of Person or Organization |
(before taxes) |
|
|
|
|
How
Often?
***5. Does anyone work as a volunteer or participate in a work training program? Yes No If yes, complete below.
Name
Name of Volunteer Site or Work Training Program
Site Address and Phone Number
Start
Date
End
Date
Hours Per Week
6. Does anyone own or jointly own any assets including a
|
|
How Much or |
Where Do You Keep This Asset and What is |
Name (Who Owns it?) |
Type of Asset |
Value of Asset? |
the Account Number? |
|
Cash on Hand |
|
|
|
Checking Account |
|
|
|
Savings Account |
|
|
|
Lottery/Gambling Winnings |
|
|
|
Other (such as interest income) |
|
|
C. Tell us about your expenses.
Yes No |
Do you pay rent or mortgage where you live? If yes, how much do you pay out of your pocket each month? $______ |
|
|
Yes No |
Do you receive assistance paying your rent? If yes, check any you received HUD Section 8 Public Housing |
|
|
Yes No |
Do you pay any other expenses where you live? If yes, check the expense and enter the monthly amount: |
|
Lot Rent $____________ Property Taxes (if paid separately) $___________ Other (list type) $ ____________ |
|
Homeowner’s dues (if paid separately) $_________Homeowners Insurance (if paid separately) $ ____________ |
Yes No |
Are you responsible for paying any utility bills separate from your rent? If yes, check all that apply. |
|
Heat Kerosene Fuel Oil Electricity Coal Wood Natural Gas LP Gas |
|
Telephone/Cell Phone Water/Sewage Garbage/Trash Utility Excess (Public Housing) |
|
How do you heat your home? ____________________ |
|
How do you cool your home? ____________________ |
Page: 2 of 5 |
|
Economic and Family Services |
Yes No |
Does anyone help pay your bills? If yes, who helps? _________________________How much $ _____________ |
Yes No |
Did you get a |
|
that was more than $20, in the recent month or within the past 12 months? If yes, who _______________________ |
Yes No |
Is your household responsible for paying any childcare or disabled adult care? |
|
If yes, who receives care? ______________________________________________ |
|
Who pays? _______________________________________________amount per month $ _____________ |
|
Name and phone number of care provider? _____________________________________________ |
|
Child/adult care expenses? _________________________________________________________ |
Yes No |
Does anyone age 60 or over, or anyone receiving disability benefits, have |
|
monthly? This includes Medicare or Health Insurance and transportation cost for medical care. If yes, do you wish to |
|
claim a deduction for these expenses Yes No If yes, to get this deduction you must attach receipts or a |
|
computer printout of your expenses. |
Yes No |
Does your household pay court ordered child support for children outside your home (include court ordered health |
|
insurance payments)? |
|
If yes, who pays the child support? _____________________________________________ |
|
Who is it paid to? ___________________________________________________________ |
|
Child’s name? _____________________________________________________________ |
|
Amount you pay? $____________ How often? _____________ |
D. Tell us about the people in your home.
Yes No |
Is anyone in your household age 16 or older attending school at least half time now or have they in the last 6 months? |
|
If yes, list the person’s name and school they attend: __________________________________________ |
|
|
|
Does anyone in your household have a felony drug conviction or controlled substance after August 22, 1996? If yes tell |
Yes No |
us his/her name, date, type, and place of conviction: _____________________________________________ |
|
_____________________________________________ |
|
|
|
Is anyone in your household in violation of probation or parole or running from the law to avoid felony prosecution? If |
Yes No |
yes tell us his/her name, date, type, and place of conviction: ________________________________________ |
|
_____________________________________________ |
|
|
|
Have you or any member of your household been convicted as an adult of aggravated sexual abuse, murder, sexual |
Yes No |
exploitation and other abuse of children, a Federal or State offense involving sexual assault, or an offense under State |
|
law determined by the Attorney General to be substantially similar to such an offense, after February 7, 2014? If yes tell |
|
us his/her name, date, type, and place of conviction: ___________________________________________ |
|
|
|
Have you or any member of your household been convicted of trading benefits for drugs after August 22, 1996? |
Yes No |
If yes tell us his/her name, date, type, and place of conviction:___________________________________________ |
|
_____________________________________________ |
|
|
|
Have you or any member of your household been convicted of buying or selling benefits $500 or more after August 22, |
Yes No |
1996? If yes tell us his/her name, date, type, and place of conviction___________________________________ |
|
_____________________________________________ |
|
|
|
Have you or any member of your household been convicted of fraudulently receiving duplicate benefits in any State |
Yes No |
after August 22, 1996? If yes tell us his/her name, date, type, and place of conviction: _______________________ |
|
_____________________________________________ |
|
|
|
Have you or any member of your household been convicted of trading benefits for guns, ammunitions, or explosives |
Yes No |
after August 22, 1996? If yes tell us his/her name, date, type, and place of conviction: _______________________ |
|
_____________________________________________ |
|
|
Yes No |
Is anyone in your household physically or mentally unfit for employment? If yes, who and what months? |
_____________________________________________ |
|
|
|
|
Does anyone operate a Home School at least 30 hours a week? If yes, who and what months? |
Yes No |
_____________________________________________ |
|
|
|
Does anyone care for an incapacitated person (does not have to live in the home)? If yes, who and what months? |
Yes No |
_____________________________________________ |
|
|
|
Does anyone participate in an official Refugee Employment Program? If yes, who and what months? |
Yes No |
_____________________________________________ |
|
|
|
Is anyone in the household unable to work due to alcohol and/or drug addiction? If yes, who and what months? |
Yes No |
_____________________________________________ |
|
|
|
Is anyone in a drug or alcohol treatment program? If yes, who and what months? |
Yes No |
_____________________________________________ |
|
|
Yes No |
Is anyone in the household pregnant? If yes, who? __________________________________________ |
|
Page: 3 of 5 |
|
Economic and Family Services |

Authorized Representative
Do you need someone to help you get and/or use your Food and Nutrition Services benefits? Yes No If yes,
please list that person’s name. If you checked Yes above, we will
give or mail you a form. You and the person you want to help can complete the form and return it to our office. This person will receive an EBT card and will have access to your Food and Nutrition Services Benefits. If you already have an authorized representative, do you want them to continue?
Yes No Authorized Representative Name:
How to Get a Fair Hearing
You have the right to ask for a hearing in person, by telephone or in writing, if you think your case is wrong. You have 90 calendar days to ask for a hearing. Unless you ask for a hearing by then, you cannot have one. A household member or someone else such as a lawyer, friend, or relative can represent you at a fair hearing. Free legal advice may be available. Contact Legal Aid of North Carolina office at
Voter Registration
“If you are not registered to vote where you live now, would you like to apply to register to vote here today?
Yes No
IF YOU DO NOT CHECK EITHER BOX, YOU WILL BE CONSIDERED TO HAVE DECIDED NOT TO REGISTER TO VOTE AT THIS TIME. Register to vote in North Carolina. If you want to register to vote or to update your registration, you can complete a voter registration form at www.ncsbe.gov/nvra/01, ask your caseworker or contact your local DSS for a voter registration form. Applying to register or declining to register to vote will not affect the amount of assistance that you will be provided by this agency. If you would like help in filling out the voter registration application form, we will help you. The decision whether to seek or accept help is yours. You may fill out the application form in private. If you believe that someone has interfered with your right to register or to decline to register to vote, your right to privacy in deciding whether to register or in applying to register to vote, or your right to choose your own political party or other political preference, you may file a complaint with the North Carolina State Board of Elections, PO Box 27255, Raleigh NC
You Will Not Be Discriminated Against
In accordance with Federal civil rights law and U.S. Department of Agriculture (USDA) civil rights regulations and policies, the USDA, its agencies, offices, and employees, and institutions participating in or administering USDA programs are prohibited from discriminating based on race, color, national origin, sex, religious creed, disability, age, political beliefs, or reprisal or retaliation for prior civil rights activity in any program or activity conducted or funded by USDA.
Persons with disabilities who require alternative means of communication for program information (e.g. Braille, large print, audiotape, American Sign Language, etc.), should contact the Agency (State or local) where they applied for benefits. Individuals who are deaf, hard of hearing or have speech disabilities may contact USDA through the Federal Relay Service at (800)
To file a program complaint of discrimination, complete the USDA Program Discrimination Complaint Form, (AD- 3027) found online at: https://
mail: U.S. Department of Agriculture
Office of the Assistant Secretary for Civil Rights 1400 Independence Avenue, SW Washington, D.C.
fax: (202)
email: program.intake@usda.gov.
This institution is an equal opportunity provider.
Page: 4 of 5 |
|
Economic and Family Services |

Getting Help with Your Telephone Bill
If you receive Supplemental Security Income (SSI), Food and Nutrition Services, Medicaid, Federal Public Housing (Sec. 8 Housing Assistance), or Veterans Pension and Survivors Benefit you may be eligible for a local telephone service discount. Lifeline provides recipients a discount on monthly telephone service purchased from participating providers. Recipients can also purchase discounted broadband from participating providers. Discounts will apply to
Your Signature and Statement of Understanding
I understand that my signature authorizes federal, state, and local officials to contact other persons or organizations to verify the information I have provided. Do not lie or hide information to get benefits that your household should not get. I have given correct information on the citizenship/immigration status of all individuals applied for. If a law enforcement officer requests the address, social security numbers, or photographs in your file to assist in locating fugitive felons or probation/parole violators, the agency must provide this information. I will report lottery and/or gambling winnings in the amount of $3,750 or more. I am aware all household members will lose eligibility to receive Food and Nutrition Services.
Any member who intentionally breaks any of the rules, may not be able to get Food and Nutrition Services for one year for the first violation, two years for second the violation, and permanently for third the violation. If a court of law finds you guilty of using or receiving benefits in a transaction involving the sale of a controlled substance, you will not be eligible for benefits for two years for the first violation, and permanently for the second violation. You may also be fined up to $250,000 and/or jailed up to 20 years. If court ordered, you may also be ineligible from the Food and Nutrition Services program for an additional 18 months. If a court finds you guilty of having trafficked benefits for $500 or more, or trading benefits for firearms, ammunition or explosives you will be permanently ineligible for Food and Nutrition Services. If you use your food assistance benefits to buy nonfood items, trade, or sell your benefits, pay on credit accounts, take someone’s EBT card without authorization or let someone use yours, you will lose your benefits. If you give false information about your identity or residence in order to get Food and Nutrition Services in more than one place, you will not get Food and Nutrition Services for 10 years. If you have a Food and Nutrition Services claim arise against you, we will give your answers and Social Security Numbers to federal and state agencies, as well as private claims collection agencies, to collect the overpayment. All eligibility procedures are strictly supported by the Food and Nutrition Services policies. The other programs time limits or requirements do not affect your Food and Nutrition Services benefits. Your household may not be denied food assistance because your household has been denied benefits from other programs.
I acknowledge that I have received an explanation of my right to an income deduction for Food and Nutrition Services benefits for any of the following items: Child/adult care expenses, medical expenses, shelter expenses, utility expenses, and operational expenses for
*YOU MUST SIGN AND FILL OUT THE INFORMATION BELOW BEFORE RETURNING*
Your Signature or Authorized Representative ____________________________Date Signed ____________
Witness Signature (if signature is an X) _________________________________Date Signed ____________
First Name _________________________Middle Initial________ Last Name____________________________
Residence Address (House/Apt. #, Street)
_________________________________________City__________________ State_____ Zip Code _________
Mailing Address (if different from Residence Address)
_________________________________________ City__________________ State_____ Zip Code _________
Home Phone ______________________Cell Phone _______________________ Message Number___________________
Telephone Company Provider _______________________________ Language you speak __________________________
For information regarding the Teen Pregnancy Prevention Initiative contact your local Health Department or call the DHHS Customer Service Center at
**AGENCY USE ONLY **
Caseworker Signature________________________________ Date of Interview_____________ |
|
Telephone |
Office Visit
Page: 5 of 5 |
|
Economic and Family Services |
Form Characteristics
| Fact Name | Details |
|---|---|
| Governing Law | The Food Stamp Program in North Carolina is governed by the Food and Nutrition Act of 2008 and state regulations that administer food assistance in compliance with federal guidelines. |
| Form Purpose | This form allows individuals to recertify their eligibility and continue receiving Food and Nutrition Services (FNS) benefits. |
| Submission Deadline | To avoid a lapse in benefits, the completed form must be returned by the due date specified in the form. |
| Language Assistance | Free language assistance is available for applicants who do not speak English, as well as communication aids for those with disabilities. |
| Verification Requirements | Applicants are responsible for providing necessary verification of income, household composition, and expenses. |
| Social Security Number Requirement | Applicants must provide Social Security Numbers for everyone included in the application, as this is mandated by federal law. |
| Penalties for Fraud | Providing false information or misusing benefits can lead to disqualification, fines, and imprisonment. |
| Authorized Representatives | Individuals may designate someone to help them navigate the application process and manage their benefits. |
| Voter Registration Option | The form provides a chance for applicants to register to vote or update their voter registration as part of the application process. |
Guidelines on Utilizing Food Stamp Nc
Once you have the Food Stamp NC form, you'll need to fill it out carefully to ensure that all your information is correct. Completing the form accurately will help avoid delays in processing your recertification. Here are the steps to fill out the form:
- Locate the Form: Ensure you have the latest version of the Food Stamp NC form in front of you.
- Fill in Your Information: Write your name, mailing address, and case identifier in the appropriate sections.
- Complete the Household Listing: List everyone who lives with you, including their relationship to you, age, and if they are applying for benefits.
- Provide Financial Details: Answer the questions about income and assets for each household member. Attach any necessary income verification.
- Document Your Expenses: Include details about your rent or mortgage payments and any utility expenses.
- Fill Out the Personal Background: Answer questions about school attendance, felony convictions, and other relevant household information.
- Complete the Authorized Representative Section: If someone is helping you with your benefits, provide their name and relationship.
- Sign and Date: Sign the form and date it at the end, confirming that all information is accurate.
- Attach Required Documentation: Include any additional documents or verifications needed for your application.
- Submit the Form: Return the completed form to the appropriate DSS mailing address or in person, ensuring it arrives by the due date.
Make sure all sections are completed before you submit the form. If you need assistance at any step, don’t hesitate to reach out to your local DSS office for help. They can answer questions and guide you through the process smoothly.
What You Should Know About This Form
What is the purpose of the Food Stamp NC form?
The Food Stamp NC form is used to apply for and recertify benefits under the Food and Nutrition Services program in North Carolina. It collects essential information about your household, income, and expenses to determine your eligibility for food assistance.
How do I submit the Food Stamp NC form?
You can submit the completed form by bringing it to your local DSS office, mailing it to the provided DSS mailing address, faxing it, or submitting an application online at https://epass.nc.gov/CitizenPortal/application.do. Ensure that your submission is sent during the specified time frame to avoid delays.
What happens if I do not submit the form by the due date?
If you do not return the form by the specified due date, your FNS benefits will stop on the expiration date indicated on the form. You may lose your eligibility for continued assistance, so it's crucial to meet the deadlines.
Who can help me fill out the Food Stamp NC form?
If you need assistance completing the form due to a disability or language barrier, call 1-866-719-0141. Local DSS offices can also provide assistance. Additionally, you can designate an authorized representative to help with your application.
What is required regarding Social Security Numbers and citizenship?
You must provide Social Security Numbers and information about citizenship or immigration status for all individuals applying for benefits. If you do not wish to provide this information, you may choose not to apply, as these details are necessary for eligibility determination.
What information must I provide about my household finances?
Your household must disclose all sources of income, including wages, pensions, and government assistance. Attach any required verification, such as pay stubs or tax forms, to complete your application. This information is critical to assess overall eligibility and benefit levels.
What are the consequences of providing false information?
Providing false information can lead to serious consequences, including disqualification from receiving benefits for a specified period, fines, and even criminal charges. Complete honesty is essential when filling out the form to avoid these outcomes.
Can I apply if I only have Supplemental Security Income (SSI)?
If your household only consists of individuals receiving SSI, you can apply for recertification at your Social Security office instead of using the Food Stamp NC form. This streamlines the process specifically for SSI recipients.
What if I require a fair hearing regarding my application?
You have the right to request a fair hearing if you believe there has been an error in your case. You must do this within 90 calendar days of receiving your determination. You can represent yourself or have someone assist you in this process.
Common mistakes
Filling out the Food Stamp NC form can be a bit overwhelming, and it’s easy to make mistakes along the way. One common error is not providing complete financial information. Every household member’s financial data is crucial for assessing eligibility. Forgetting to mention other sources of income, like child support or unemployment benefits, can lead to delays or denials. Make sure to list all sources of income carefully and accurately.
Another mistake people often make is skipping required signatures. It may seem minor, but a form without a signature is incomplete. This step is critical to confirming that all the information provided is accurate. Ensure that you, or your authorized representative, sign the form completely before sending it off. Double-check that the signature aligns with the printed name to avoid any confusion.
Failing to attach necessary documentation is another frequent issue. Verifications for the specified month are essential. If you’re asked to provide proof of income, residency, or expenses, be sure those documents are included. The more thorough your submission, the less likely you’ll need to go back and forth with your worker, which can slow down the process.
Lastly, people sometimes return the form too early. Remember, you should not submit this form before the designated start date. Adhering to the timeline is important to avoid issues with your benefits. Check the dates carefully and ensure that you’re following the guidelines about when to send your application.
Documents used along the form
When applying for or renewing benefits through the Food Stamp NC form, several supporting documents may be required to help verify your eligibility. Below are some of the forms and documents that are often used alongside the Food Stamp NC form:
- Verification of Income Form: This document provides proof of any employment income received. It includes details such as employer information and pay stubs, essential for determining eligibility for benefits.
- Identity Verification Document: This is used to confirm an applicant's identity. Acceptable forms of identification may include a driver's license, state ID, or passport.
- Social Security Number Verification: This document must list the Social Security numbers for all household members applying for benefits. It is required to validate claims for assistance and to comply with federal regulations.
- Residency Verification Form: Applicants must prove they reside in the area where they are applying for benefits. This may include utility bills, rental agreements, or other official documents showing the applicant's address.
- Household Expenses Documentation: This includes receipts or statements outlining monthly expenses such as rent, utility costs, and childcare, which can influence the benefit amount a household may receive.
Providing these documents can streamline the application and approval process for Food Stamp benefits. It's important to prepare each form carefully to ensure that the application is processed smoothly.
Similar forms
- SNAP Application Form: Similar to the Food Stamp NC form, this application is used to apply for federal food assistance. Both forms require detailed household income and expense information to determine eligibility.
- WIC Program Application: The Women, Infants, and Children (WIC) program requires a similar application process to assess eligibility based on family size, income, and nutritional needs. Both forms focus on providing assistance to low-income families.
- Medicaid Application: This form is essential for applying for medical assistance. Much like the Food Stamp NC form, it asks for personal, financial, and household information to assess eligibility for benefits.
- Temporary Assistance for Needy Families (TANF) Application: This document serves to request financial assistance to support families in need. It also collects similar verification and income details as the Food Stamp NC form.
- Supplemental Security Income (SSI) Application: Individuals applying for SSI must provide financial information and household status, paralleling the requirements of the Food Stamp NC form in assessing economic eligibility.
- Housing Assistance Application: This application form is for those seeking help with housing costs. Like the Food Stamp NC form, it requires income details and household size to determine aid eligibility.
- Unemployment Benefits Application: When applying for unemployment assistance, applicants must provide financial details and work history, similar to the information requested on the Food Stamp NC form.
Dos and Don'ts
- Do ensure all sections are completed. Fill out every part of the form accurately.
- Do attach necessary documentation. Provide any verification required for the application.
- Do read the instructions carefully. Familiarize yourself with all requirements and deadlines.
- Do keep a copy for your records. Always have a personal copy of the completed application.
- Don't submit the form before the designated date. Wait until the official submission period begins.
- Don't provide false information. Be honest about your financial situation and household details.
Misconceptions
Here are ten common misconceptions about the Food Stamp NC form, often referred to as the DSS Food and Nutrition Services application. Understanding these misconceptions can help individuals navigate the process more effectively.
- Misconception 1: Individuals must fill out the entire application.
- Misconception 2: Only the head of the household can apply.
- Misconception 3: Social Security Numbers are optional for all applicants.
- Misconception 4: Recertification is not necessary if you have ongoing benefits.
- Misconception 5: You can return the application anytime.
- Misconception 6: You need to provide financial information for all household members.
- Misconception 7: You cannot receive assistance if you have a felony conviction.
- Misconception 8: The application process is too complicated to understand.
- Misconception 9: If denied, you cannot appeal the decision.
- Misconception 10: Your benefits will never change once awarded.
It's important to know that if you cannot complete the form, it's sufficient to provide just your signature, name, and address for processing your request.
Any member of the household or an authorized representative can complete and submit the application on behalf of the group.
In fact, providing a Social Security Number is mandatory for anyone applying for benefits. This helps verify eligibility through state and federal databases.
It is essential to recertify before your benefits expire. If you fail to do so, your benefits will stop.
You should not return the form before the specified date provided in the instructions. Doing so could delay processing.
Only the individuals applying for benefits are required to provide their financial details. Others in the household can remain confidential if they are not applying.
This is not always the case. While certain felony convictions may affect eligibility, individuals can still apply for benefits under specific conditions.
The form is designed to be accessible, and assistance is available for those who need help completing it. Resources are accessible for non-English speakers and individuals with disabilities.
You have the right to request a hearing if you believe your case was handled incorrectly. This must be done within 90 days of the denial.
Your benefits may change based on household income, size, and other factors. Regular updates and verifications are crucial to maintaining accurate support.
Key takeaways
- Complete the Form Fully: Ensure that you fill out every section of the Food Stamp NC form. Missing information may lead to delays or complications with your benefits.
- Sign and Date: Don’t forget to sign and date the form at the bottom. An unsigned form may prevent your application from being processed.
- Verification Documents: Attach any necessary verification documents as specified on the form. This may include income proof, housing costs, and identification.
- Submission Deadline: Return the completed form before the specified due date to avoid interruption in your benefits.
- Language Assistance: If you need help because English is not your first language, free interpreter services are available. Contact your local DSS office for assistance.
- Household Members: List everyone in your household who is applying for benefits. Make sure to include their personal information as required.
- Financial Information: Provide detailed financial information for everyone applying. This will help determine your eligibility and benefit amount.
- Discrimination Rights: Remember that you have the right to be treated fairly. If you feel you have been discriminated against, you can file a complaint with the appropriate authorities.
Browse Other Templates
America First Credit Union External Transfer Limit - Use the correct beneficiary account name to ensure funds are received.
What Is a Dwc 1 Form - It is crucial for employees to keep a copy of the signed form for their records.