Fill Out Your 5021 Form
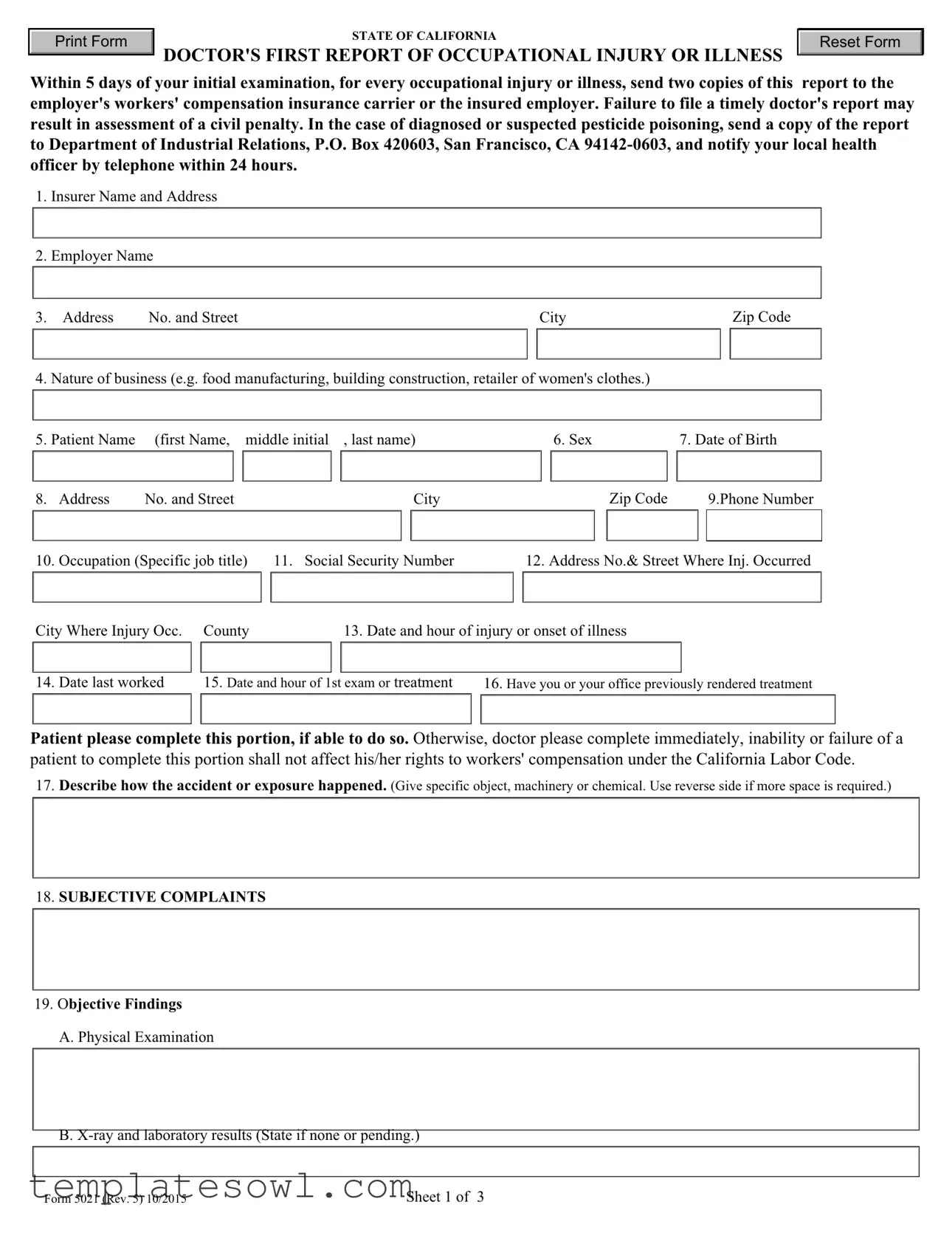
The California 5021 form, officially known as the Doctor's First Report of Occupational Injury or Illness, plays a vital role in the workers' compensation process for individuals who have experienced job-related injuries or illnesses. Within five days of a patient’s initial examination, healthcare providers must complete and file this report with the employer's workers' compensation insurance carrier. This is crucial not only for ensuring the patient receives timely care but also for confirming their eligibility for benefits. The form requires detailed information, including the patient's personal data, the nature of the business where the injury occurred, specifics about the incident itself, and the physician's findings and treatment plans. Should the injury be linked to pesticide exposure, additional reporting to health authorities is mandated. Failing to submit this report within the designated timeframe could lead to penalties, emphasizing the importance of timely compliance. Overall, this form is designed to facilitate an efficient response to workplace injuries, ensuring that all necessary parties are informed and can act accordingly to support the affected individual’s recovery process.
5021 Example
Print Form |
STATE OF CALIFORNIA |
Reset Form |
|
DOCTOR'S FIRST REPORT OF OCCUPATIONAL INJURY OR ILLNESS |
|
|
|
Within 5 days of your initial examination, for every occupational injury or illness, send two copies of this report to the employer's workers' compensation insurance carrier or the insured employer. Failure to file a timely doctor's report may result in assessment of a civil penalty. In the case of diagnosed or suspected pesticide poisoning, send a copy of the report to Department of Industrial Relations, P.O. Box 420603, San Francisco, CA
1.Insurer Name and Address
2.Employer Name
3. |
Address |
No. and Street |
|
City |
|
Zip Code |
4. |
Nature of business (e.g. food manufacturing, building construction, retailer of women's clothes.) |
|
|
|||
5. |
Patient Name |
(first Name, middle initial |
, last name) |
6. Sex |
7. Date of Birth |
|
8. |
Address |
No. and Street |
City |
Zip Code |
|
9.Phone Number |
|
|
|
|
|
|
|
10. |
Occupation (Specific job title) |
11. Social Security Number |
12. Address No.& Street Where Inj. Occurred |
|
City Where Injury Occ. |
County |
13. Date and hour of injury or onset of illness |
||
14. |
Date last worked |
15. Date and hour of 1st exam or treatment |
16. Have you or your office previously rendered treatment |
|
Patient please complete this portion, if able to do so. Otherwise, doctor please complete immediately, inability or failure of a patient to complete this portion shall not affect his/her rights to workers' compensation under the California Labor Code.
17.Describe how the accident or exposure happened. (Give specific object, machinery or chemical. Use reverse side if more space is required.)
18.SUBJECTIVE COMPLAINTS
19.Objective Findings
A.Physical Examination
B.
Form 5021 (Rev. 5) 10/2015
Sheet 1 of 3
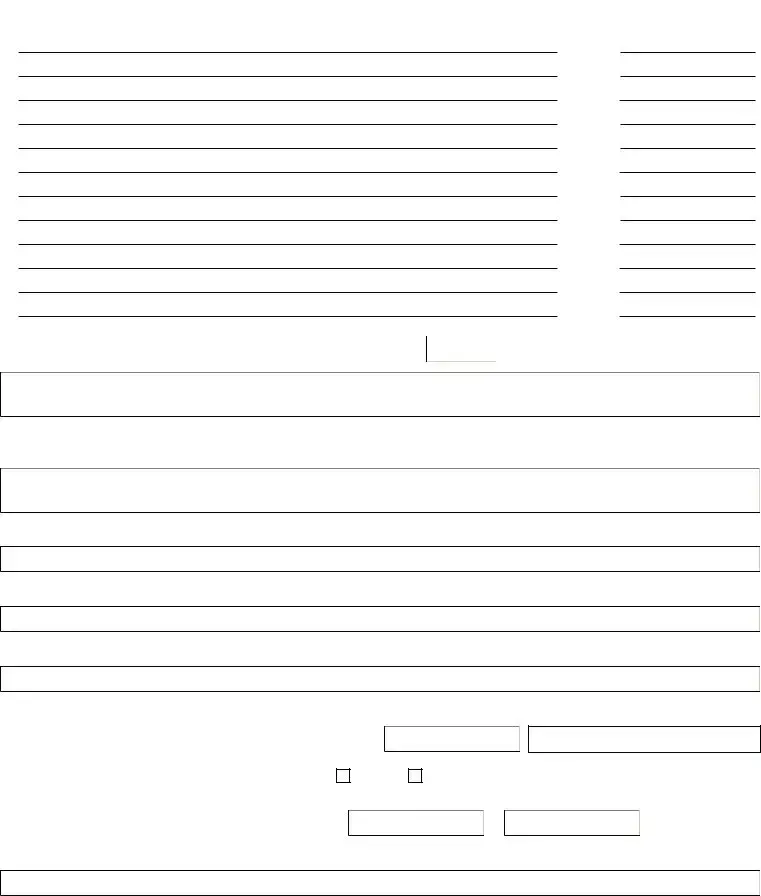
STATE OF CALIFORNIA DOCTOR'S FIRST REPORT OF OCCUPATIONAL INJURY OR ILLNESS
20. DIAGNOSES(if occupational illness specify etiologic agent and duration of exposure.) Chemical or toxic compounds involved? 
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
21. Are your findings and diagnosis consistent with patient's account of injury or onset of illness?
22. Is there any other current condition that will impede or delay patient's recovery?
23.TREATMENT RENDERED (Use reverse side if more space is required.)
24.If further treatment required, specify treatment plan/estimated duration.
25.If hospitalized as inpatient, give hospital name and location
Date admitted
If "no," please explain below:
If "yes," please explain below:
Estimated length of stay
26.WORK STATUS - Is patient able to perform usual work? If "no", date when patient can return to
Yes |
No |
Regular work |
Modified work |
Specify restrictions
Form 5021 (Rev. 5) 10/2015
Sheet 2 of 3
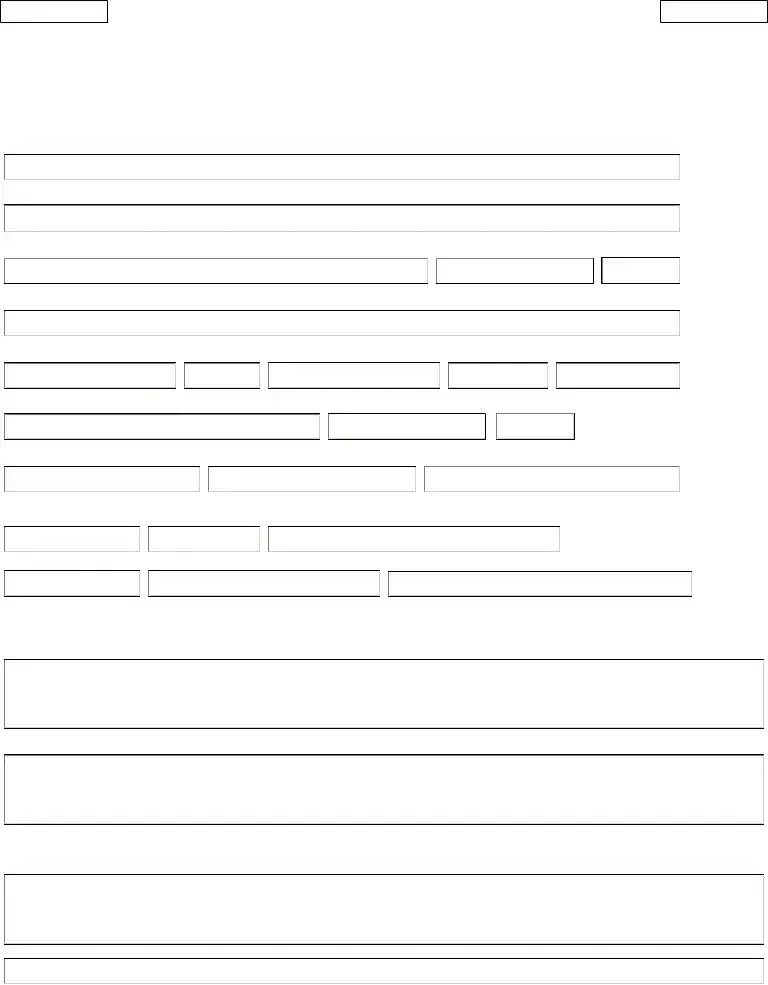
STATE OF CALIFORNIA
DOCTOR'S FIRST REPORT OF OCCUPATIONAL INJURY OR ILLNESS
Physician Signature: (original signature, do not stamp)
I declare under penalty of perjury that this report is true and correct to the best of my knowledge and that I have not violated Labor Code section 139.3.
Physician signature |
|
|
Cal. License Number: |
|
|||||||
Executed at: |
|
|
|
Date (mm/dd/yyyy): |
|
||||||
Physician Name |
|
|
|
Specialty: |
|
|
|||||
Physician address: |
|
|
|
Phone Number |
|
|
|||||
Any person who makes or causes to be made any knowingly fraudulent material statement or material representation for the
purpose of obtaining or denying workers' compensation benefits or payments is guilty of a felony.
PRIVACY NOTICE: The Administrative Director is authorized to maintain the records of the Division of Workers' Compensation (DWC). (Cal. Lab. Code
§126.) The Information Practices Act of 1977 and the Federal Privacy Act require the Administrative Director to provide this notice to individuals who submit information to the DWC pertaining to a workers' compensation claim. (Cal. Civ. Code § 1798.17; Public Law
The principal purpose for requesting information from injured workers, dependents, lien claimants, physician, employers or their representatives is to administer the California workers' compensation system. Each form shows which fields are required to be completed for DWC to process the form. If a required field in a form is incomplete or unreadable, the DWC may return the form to the individual for correction or may reject the form. Providing a social security number is required on this form pursuant to Labor Code § 6409. If you do not provide your security number, the DWC may return the form to you for correction or reject the form. If you do not have a social security number, indicate this in the space provided for the injured worker's social security number. As permitted by law, social security numbers are used to help properly identify injured workers and to conduct statistical research as allowed under the Labor Code.
As authorized by law, information furnished on this form may be given to: you, upon request; the public, pursuant to the Public Records Act; a governmental entity, when required by state or federal law; to any person, pursuant to a subpoena or court order pursuant to any other exception in Civil Code § 1798.24.
An individual has a right of access to records containing his/her personal information that are maintained by the Administrative Director. An individual may also amend, correct, or dispute information in such personal records. (Cal. Civ. Code §§
Form 5021 (Rev. 5) 10/2015 |
Sheet 3 of 3 |
Form Characteristics
| Fact Name | Details |
|---|---|
| Name of Form | Doctor's First Report of Occupational Injury or Illness |
| Form Number | 5021 |
| Filing Deadline | Must be filed within 5 days of the initial examination. |
| Recipient | Send two copies to the employer's workers' compensation insurance carrier or the insured employer. |
| Pesticide Poisoning Protocol | Report to the Department of Industrial Relations and notify local health officer within 24 hours if applicable. |
| Applicable Law | California Labor Code, Sections 6409 and 139.3. |
| Required Information | Includes patient personal information, nature of injury, diagnosis, treatment rendered, and work status. |
| Consequences of Non-Compliance | Failure to file timely may result in a civil penalty. |
| Privacy Notice | Information is maintained under the California Information Practices Act of 1977 and the Federal Privacy Act. |
Guidelines on Utilizing 5021
The next steps involve ensuring all necessary information is accurately provided on the 5021 form. Timely completion and submission of this form are vital to avoid potential penalties. Follow the steps below to fill out the form effectively.
- Insurer Name and Address: Write the full name and address of the insurance carrier.
- Employer Name: Fill in the name of the employer.
- Address: Enter the employer's address, including number and street, city, and zip code.
- Nature of Business: Describe the type of business, such as food manufacturing or retail.
- Patient Name: Provide the patient's first name, middle initial, and last name.
- Sex: Specify the patient's gender.
- Date of Birth: Enter the patient's birth date.
- Patient Address: Fill in the patient’s full address, including number and street, city, and zip code.
- Phone Number: Write the patient’s phone number.
- Occupation: State the patient’s specific job title.
- Social Security Number: Include the patient’s social security number.
- Address Where Injury Occurred: Specify the location of the injury, including number and street, city, and county.
- Date and Hour of Injury: Provide the date and time of the injury or illness onset.
- Date Last Worked: Fill in the last date the patient worked.
- Date and Hour of First Exam: Enter the date and time of the first examination or treatment.
- Previous Treatment: Indicate if prior treatment has been rendered. If yes or no, provide explanations as required.
- Description of Accident or Exposure: Provide details on how the accident or exposure occurred, mentioning specific objects or machinery. Use the reverse side if more space is needed.
- Subjective Complaints: Document the patient’s subjective complaints.
- Objective Findings: Summarize the findings from the physical examination and any relevant x-rays or laboratory results.
- Diagnoses: Specify the diagnoses, including occupational illness and any chemical compounds involved.
- Consistency with Patient's Account: Confirm whether the findings and diagnosis align with the patient’s statements.
- Current Conditions: Note any current conditions that may impact recovery.
- Treatment Rendered: Describe the treatment provided. Additional details can be added on the reverse side if necessary.
- Further Treatment Required: Outline any needed further treatment, including a treatment plan and estimated duration.
- Hospital Information: If hospitalization was required, provide the hospital name, location, and date admitted.
- ICD-10 Codes: List relevant ICD-10 codes as required.
- Work Status: Indicate if the patient can perform their regular or modified work, and specify any restrictions.
- Physician Signature: Sign the form with the original signature and declare the report's accuracy. Fill in the physician's name, specialty, address, and phone number.
What You Should Know About This Form
What is the purpose of the 5021 form?
The 5021 form, also known as the Doctor's First Report of Occupational Injury or Illness, serves as an essential document in the California workers' compensation system. It must be completed by a medical professional to report details about an employee's occupational injury or illness. This report is crucial for the employer's workers' compensation insurance carrier, as it provides necessary information for processing claims and ensuring the injured worker receives appropriate benefits.
Who is responsible for submitting the 5021 form?
The responsibility for submitting the 5021 form primarily lies with the medical provider who examines the injured worker. They are required to send two copies of the completed form to the employer’s workers' compensation insurance carrier within five days of the initial examination. Timely submission is essential, as delays can lead to penalties.
What happens if the 5021 form is not submitted on time?
If the 5021 form is not submitted within the required timeframe, there may be serious consequences. Specifically, the California Labor Code may impose civil penalties for late submissions. Therefore, it is vital for healthcare providers to prioritize the timely completion and submission of this report to avoid any potential penalties.
What information needs to be included on the 5021 form?
The form requires comprehensive information about the injury or illness. Key details include the patient's identity, description of the accident or exposure, nature of the business, and specifics on the injury's occurrence. Medical findings, treatment given, and the physician's diagnosis must also be included. This information assists in establishing a clear medical history related to the worker's compensation claim.
Is the patient's personal information kept confidential?
Yes, the 5021 form includes a privacy notice emphasizing the confidentiality of personal information. The information collected is used to administer the workers' compensation system and can only be shared under specific legal circumstances. Individuals do have the right to access and amend their personal information maintained by the Administrative Director.
What should be done in case of pesticide poisoning?
In the event of diagnosed or suspected pesticide poisoning, there are additional steps to be taken alongside submitting the 5021 form. A copy of the report must be sent to the Department of Industrial Relations, and the local health officer should be notified by telephone within 24 hours. This prompt action ensures proper tracking and response to such serious health concerns.
Common mistakes
When filling out the 5021 form, many make simple mistakes that can lead to delays or complications in the workers' compensation process. One common error is missing required fields. The form contains several mandatory sections that must be completed for the submission to be accepted. Omitting details like patient name, date of injury, or social security number is a common oversight that can prevent timely processing.
Another frequent mistake occurs in the description of the incident. It's important to provide a clear and specific account of how the injury or illness occurred. Vague descriptions can lead to confusion and may result in the form being returned for additional clarification. Always include relevant objects, machinery, or chemicals involved.
Many people also struggle with providing accurate treatment details. It's essential to document all treatments rendered, along with any follow-up plans. Leaving sections incomplete or misreporting treatment can undermine the validity of the report and affect the injured worker’s claim.
Inaccuracies in the work status section can create unnecessary complications. The physician must indicate whether the patient is able to return to regular or modified work. Providing unclear or conflicting information might delay the patient’s ability to receive benefits while recovering.
Another mistake includes failing to submit the form on time. The law requires that this report be filed within five days of the initial examination. Delays in filing may lead to penalties and affect the benefits the patient can receive. Make sure to meet deadlines to avoid these issues.
Lastly, some individuals forget to sign and date the form properly. An original signature is required; a stamped signature will not suffice. An unsigned form can be considered invalid, which is a preventable issue that can cause unnecessary frustration for everyone involved in the process.
Documents used along the form
The 5021 form, known as the Doctor's First Report of Occupational Injury or Illness, is a key document in the workers' compensation process in California. When filing this report, there are several other forms and documents that may often be required or beneficial to include. Each form serves a specific purpose in documenting the injury and facilitating the claims process.
- Workers' Compensation Claim Form (DWC 1): This form is filled out by the employee to initiate a claim for workers' compensation benefits. It provides basic information about the employee, the injury, and the details surrounding the incident.
- Medical Treatment Authorization (MTA): This document authorizes medical treatment for the injured worker and outlines the approved healthcare providers and treatment types. It helps ensure that the necessary treatments are covered under the workers' compensation policy.
- Notice of Injury or Illness (DWC Form 5020): This form is used to notify the employer of a work-related injury or illness. It includes essential details about the incident, which is crucial for the employer’s records and their timely response to the claim.
- Employer's Report of Occupational Injury or Illness: This document is completed by the employer to report the injury or illness to their workers' compensation insurance carrier. It describes how the incident occurred from the employer's perspective.
- Subsequent Report of Occupational Injury or Illness: Used for updates on the injured worker's condition or changes in treatment, this report should be submitted after the initial report if the worker's status changes.
- Physician's Progress Report: This report provides ongoing updates from the healthcare provider regarding the patient's recovery, treatment plans, and work capabilities. It is crucial for tracking the worker's progress.
- Return to Work Form: After treatment, this document outlines the worker's ability to return to their job, including any restrictions or need for modified duties. It is important for both the employee and employer to establish a safe reintegration into the workplace.
- Legal Representation Authorization Form: If the injured worker chooses to have legal representation, this form grants the attorney access to pertinent records and communication regarding the case.
Each of these forms plays a vital role in the workers' compensation process, helping to ensure that all parties involved have the necessary information for effective communication and proper management of the claim. The completion and timely submission of these documents can greatly influence the efficiency of the claims process and the provision of benefits to the injured worker.
Similar forms
- Worker's Compensation Claim Form: Similar to the 5021 form, this document initiates the process for workers' compensation claims. It collects essential information about the injury and the injured worker, including medical history and circumstances surrounding the incident.
- Doctor's Progress Report: This report details ongoing treatment and recovery information for the injured worker. Like the 5021 form, it ensures that all relevant medical findings are documented to facilitate appropriate claims processing.
- Notice of Injury: Employers often require a formal notification of an injury sustained by an employee. This document shares many of the same necessary details about the employee, injury, and initial response, ensuring that all parties are informed.
- First Report of Injury (FROI): This form is filed by employers with their insurance carrier following an employee's injury. It captures details similar to the 5021 form, including the employee's information, nature of business, and circumstances of the injury.
- Medical Authorization Form: Often required by insurers, this document allows insurance companies access to the medical records of the injured worker. It ensures that relevant medical information is shared, paralleling the intention of the 5021 form in documenting injury responses.
- Return to Work (RTW) Form: This document provides information about the injured worker's ability to resume work. It includes insights from the medical professional similar to those found in the 5021 form, confirming physical capabilities and any restrictions.
Dos and Don'ts
When filling out the 5021 form, there are important guidelines to follow to ensure accurate and timely submission. Below is a list of dos and don'ts.
- Do complete the form within five days of the initial examination.
- Do send two copies to the employer's workers' compensation insurance carrier or the employer.
- Do include the patient’s Social Security number as required.
- Do provide a detailed description of how the accident or exposure occurred.
- Do ensure that all required fields are filled out completely and legibly.
- Don't delay the submission of the form, as this may result in penalties.
- Don't use a stamped signature; the physician must sign the form personally.
- Don't leave any relevant information incomplete, as this can cause delays in processing.
- Don't forget to notify the local health officer within 24 hours in cases of suspected pesticide poisoning.
Misconceptions
Misconceptions about the 5021 form can lead to confusion and delays in the workers' compensation process. Here are some common myths and the truths behind them:
- The 5021 form is optional. This form is mandatory for reporting occupational injuries or illnesses within five days of the examination.
- Only doctors can fill out the 5021 form. While the doctor must complete it, injured patients can help by providing information if they are able.
- Submitting the form late has no consequences. A late submission may lead to civil penalties, which can affect both the doctor and the patient.
- All forms can be submitted electronically. Not all insurance carriers accept electronic submissions. It's important to check with the specific carrier.
- Providing a social security number is not necessary. The form requires a social security number, and failing to provide it may lead to the form being rejected or returned.
- The form is only relevant for workers with serious injuries. The 5021 form applies to all occupational injuries and illnesses, regardless of severity.
- The information on the form remains completely confidential. While there are privacy protections, some information may be shared under legal requirements or public records laws.
- The 5021 form covers all aspects of a workers' compensation claim. This form serves as a doctor's report. Additional forms and information may still be necessary for a complete claim.
Key takeaways
Understanding the nuances of filling out the 5021 form is essential for ensuring compliance and facilitating workers’ compensation claims. Below are key takeaways to consider.
- Timeliness is Crucial: Submit two copies of the report within five days of the initial examination to the employer's workers' compensation insurance carrier.
- Pesticide Poisoning Protocol: If exposure to pesticides is suspected, notify both the Department of Industrial Relations and the local health officer within 24 hours.
- Accurate Data is Essential: Fields such as patient information, employer details, and specifics of the injury or illness must be accurately completed.
- Document Specifics: When describing how the accident or exposure occurred, be detailed and specific about the machinery, chemicals, or objects involved.
- Compliance and Accuracy: Incomplete or unreadable forms may be returned or rejected by the Division of Workers' Compensation, delaying processing.
- Signature Requirement: The form must be signed by the physician, and signatures should not be stamped.
- Social Security Number Requirement: Providing a social security number is mandatory for identification purposes; if unavailable, indicate accordingly in the designated area.
- Review of Privacy Rights: Be aware of the rights regarding personal information as outlined in the privacy notice, including the right to access and amend personal records.
Each of these points underscores the importance of diligence when completing the 5021 form. Establish clear communication between all parties involved to streamline the process and uphold compliance.
Browse Other Templates
Employee Performance Assessment Form,Civilian Performance Counseling Record,Base System Counseling Checklist,Organizational Performance Review Document,Civilian Staff Evaluation Guide,Performance Feedback and Counseling Record,Professional Developmen - Written input from the Ratee can offer insights that enhance the counseling process.
Telephone Tree - Reliability is critical; ensure everyone knows how to use the phone tree.
Autocad Exam Questions - Strategic study guided by the objectives will enhance overall performance on the exam.