Fill Out Your Ar N Form
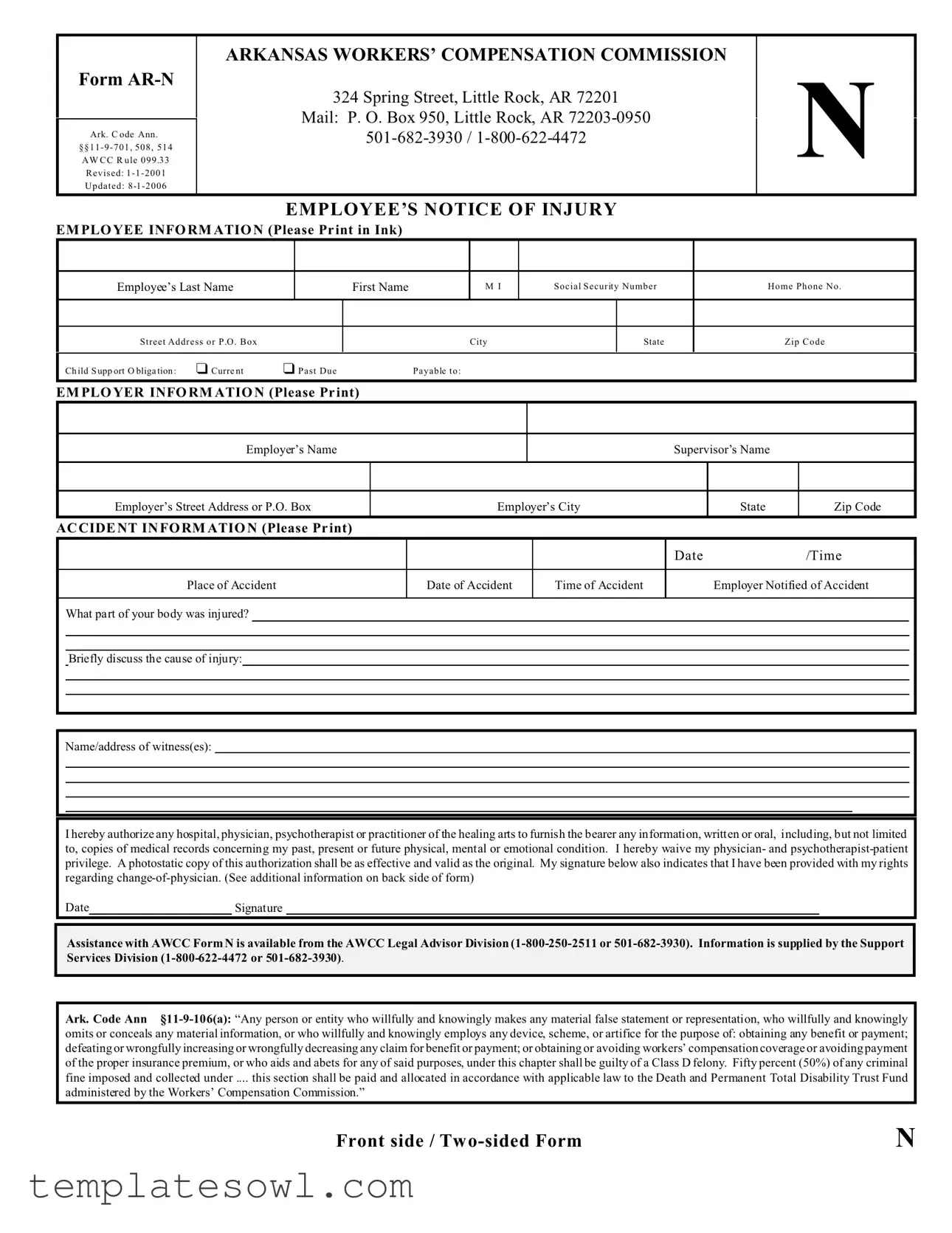
The Form AR-N is an essential document related to workers' compensation in Arkansas, designed to ensure that employees can effectively report injuries sustained on the job. It serves a crucial role in the process of documenting incidents that may lead to claims for medical benefits or compensation. This one-page form requires essential information about the employee, including their name, social security number, and contact details. It also necessitates pertinent information about the employer, such as the company name and address. The form captures vital accident details, including the date, time, and location of the incident, as well as a description of the injuries sustained and the cause of the accident. Employees can list any witnesses and sign an authorization that allows medical providers to share their medical history relevant to the injury. It is imperative that both employees and employers understand the reporting process outlined in the Arkansas Workers’ Compensation laws, which stipulate that injuries must be reported in a timely manner for benefits to be received. Failure to do so may result in complications or delays in claims processing. Additionally, the form addresses the employee’s rights regarding change-of-physician requests, ensuring that they have access to appropriate medical care. Thus, the Form AR-N is not only a legal requirement but also a pivotal tool for employees seeking to navigate the complexities of workers’ compensation in Arkansas.
Ar N Example
Form
Ark. C ode Ann. §§11 - 9 - 701, 508, 514 AW CC R ule 099 .33
Revised: 1 - 1 - 2001
Updated: 8
ARKANSAS WORKERS’ COMPENSATION COMMISSION
324 Spring Street, Little Rock, AR 72201
Mail: P. O. Box 950, Little Rock, AR
N
EMPLOYEE’S NOTICE OF INJURY
EM PLO YEE INFO RM ATIO N (Please Pr int in Ink)
Employee’s Last Name |
|
|
First Name |
|
M I |
Social Security Number |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address or P .O . Box |
|
|
|
|
City |
|
State |
|
|
|
|
|
|
|
|
||
Ch ild S upp ort O bliga tion : |
“ Curre nt |
“ Past Due |
|
Payable to: |
|
|
||
|
|
|
|
|
|
|
|
|
Home Phone No .
Zip Code
EM PLO YER INFO RM ATIO N (Please Pr int)
Employer’s Name
Employer’s Street Address or P.O. Box
AC CIDE NT IN FO RM ATIO N (Please Pr int)
Supervisor’s Name
|
Employer’s City |
State |
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
Date/Time
Place of Accident
Date of Accident
Time of Accident
Employer Notified of Accident
What part of your body was injured?
Briefly discuss the cause of injury:
Name/address of witness(es):
I hereby authorize any hospital, physician, psychotherapist or practitioner of the healing arts to furnish the bearer any information, written or oral, including, but not limited to, copies of medical records concerning my past, present or future physical, mental or emotional condition. I hereby waive my physician- and
Date |
|
Signature |
Assistance with AWCC Form N is available from the AWCC Legal Advisor Division
Ark. Code Ann
omits or conceals any material information, or who willfully and knowingly employs any device, scheme, or artifice for the purpose of: obtaining any benefit or payment; defeating or wrongfully increasing or wrongfully decreasing any claim for benefit or payment; or obtaining or avoiding workers’ compensation coverage or avoiding payment of the proper insurance premium, or who aids and abets for any of said purposes, under this chapter shall be guilty of a Class D felony. Fifty percent (50%) of any criminal fine imposed and collected under .... this section shall be paid and allocated in accordance with applicable law to the Death and Permanent Total Disability Trust Fund
administered by the Workers’ Compensation Commission.”
Front side / Tw |
N |
Form
Ark. C ode Ann.
§§11 - 9 - 701, 508, 514 AW CC R ule 33
Revised: 1 - 1 - 2001
Updated: 8
ARKANSAS WORKERS’ COMPENSATION COMMISSION
324 Spring Street, Little Rock, AR 72201
Mail: P. O. Box 950, Little Rock, AR
N
EMPLOYER’S NOTICE TO EMPLOYEE
NOTICE TO EMPLOYEE - Fill out this form to give to your employer immediately. Employer: Be sure the employee receives a copy of this form [Ark. Code Ann. §
Ark. Code Ann. §
(a)(1) Unless an injury either renders the employee physically or mentally unable to do so, or is made known to the employer immediately after it occurs, the employee shall report the injury to the employer on a form prescribed or approved by the Workers’ Compensation Commission and to a person or at a place specified by the employer, and the employer shall not be responsible for disability, medical, or other benefits prior to receipt of the employee’s report of injury.
(2)All reporting procedures specified by the employer must be reasonable and shall afford each employee reasonable notice of the reporting requirements.
(3)The foregoing shall not apply when an employee requires emergency medical treatment outside the employer’s normal business hours; however, in that event, the employee shall cause a report of the injury to be made to the employer on the employer’s next regular business day.
(b)(1) Failure to give the notice shall not bar any claim:
(A)If the employer had knowledge of the injury or death;
(B)If the employee had no knowledge that the condition or disease arose out of and in the course of the employment; or
(C)If the commission excuses the failure on the grounds that for some satisfactory reason the notice could not be given.
(2)Objection to failure to give notice must be made at or before the first hearing on the claim.
CHOICE/CHANGE OF PHYSICIAN
Rights and responsibilities. Treatment or services furnished or prescribed by any physician other than the ones selected according to the provisions below, except emergency treatment, shall be at the claimant’s/employee’s expense.
Ark. Code Ann. §
“(e). . . [T]he injured employee shall have direct access to any optometric or ophthalmologic medical service provider who agrees to provide services under the rules, terms, and conditions regarding services performed by the managed care entity initially chosen by the employer for the treatment and management of eye injuries or conditions.”
1.Your employer shall have the right to select the initial primary care physician from among those associated with certified MCOs.
2.You may request a
3.If your request for change of physician is denied you may send a petition to the Clerk of the Arkansas Workers’ Compensation Commission for a one
(1)time only
4.If your employer has contracted with a certified MCO, you shall be allowed to change physicians by petitioning the commission one (1) time only for a
5.If your employer does not have a contract with a certified MCO, you shall be allowed to change physicians by petitioning the commission one
(1)time only for a
Back side /
N
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Identification | This is Form AR-N, specifically used for reporting workplace injuries in Arkansas. |
| Governing Laws | The form is governed by Ark. Code Ann. §§11 - 9 - 701, 508, 514 and AWCC Rule 099.33. |
| Revisions | The form was last revised on January 1, 2001, and updated on August 1, 2006. |
| Filing Location | Forms should be submitted to the Arkansas Workers’ Compensation Commission located at 324 Spring Street, Little Rock, AR 72201. |
| Contact Information | The commission can be reached at 501-682-3930 or 1-800-622-4472. |
| Employee’s Responsibilities | Employees must report injuries immediately according to the protocols established by their employer. |
| Employer’s Obligations | Employers are required to provide employees with knowledge of reporting procedures and forms. |
| Change-of-Physician | Employees have the right to request a change of physician under certain conditions as specified in the law. |
| Witness Information | Employees must provide names and addresses of any witnesses to the incident when completing the form. |
| Legal Consequences | Willful misstatements on the form can result in criminal charges, classified as a Class D felony under Ark. Code Ann. § 11-9-106. |
Guidelines on Utilizing Ar N
Completing the AR N form is essential to ensure that your workers' compensation claim is handled promptly and correctly. Follow these steps to fill out the form accurately and provide the necessary information regarding your workplace injury.
- Start with the Employee Information section. Print your last name, first name, and middle initial clearly in the designated spaces.
- Enter your Social Security Number.
- Provide your street address or P.O. Box, including city, state, and zip code.
- Indicate your home phone number.
- If applicable, check the box next to Child Support Obligation to indicate if you have current or past due obligations, and specify who it is payable to.
- Fill in the Employer Information section with your employer’s name and their complete address.
- Next, go to the Accident Information section. Fill in the name of your supervisor.
- Document the date and time of the accident, as well as the place where it occurred.
- Specify if and when the employer was notified of the accident.
- Describe the part of your body that was injured.
- Briefly explain the cause of your injury.
- List the names and addresses of any witnesses.
- Sign the authorization statement allowing medical records to be shared and acknowledging your rights concerning a change of physician.
- Date your signature.
Ensure you review the completed form for accuracy before submission. Once filled out, submit the form to your employer to comply with reporting requirements. Keep a copy for your records.
What You Should Know About This Form
What is Form AR-N?
Form AR-N is the Employee’s Notice of Injury used in Arkansas to report a work-related injury. This form is essential for employees who wish to notify their employer and the Arkansas Workers’ Compensation Commission about an incident that caused injury. The completion of this form helps initiate the workers' compensation claims process.
When should I fill out Form AR-N?
Employees should fill out Form AR-N as soon as possible after the injury has occurred. It is important to report the injury immediately, or as soon as the employee is physically able to do so. Timely completion of this form ensures that the employer is notified and can begin the process of addressing the injury claim.
What information is required on Form AR-N?
The form requires personal information such as the employee's name, Social Security number, and contact information. Additionally, details of the injury must be provided, including the date, time, and place of the accident, what part of the body was injured, and a brief account of how the injury occurred. It is also advisable to list any witnesses to the incident.
What happens if I do not fill out Form AR-N?
If an employee fails to notify their employer about a work-related injury using Form AR-N, this may affect their ability to receive workers’ compensation benefits. However, as per Arkansas law, failure to give notice may not bar a claim if the employer already had knowledge of the injury or if the employee had a valid reason for not reporting it.
Can I change my physician after filing Form AR-N?
Yes, employees have the right to request a change of physician after filing Form AR-N. Initially, a request for a change should be directed to the employer or insurance carrier. If the request is denied, employees may petition the Arkansas Workers’ Compensation Commission for one change of physician. It is important to follow the specific procedures outlined in the form and associated regulations.
How can I get assistance with Form AR-N?
Assistance with Form AR-N is available through the Arkansas Workers’ Compensation Commission. Employees can reach out to the Legal Advisor Division or the Support Services Division by calling 1-800-250-2511 or 501-682-3930 for help in completing the form or understanding their rights and responsibilities related to their injury.
Common mistakes
Filling out the AR-N form incorrectly can lead to delays or complications in processing a workers' compensation claim. Here are some common mistakes that many people make when completing this form.
One common error is not providing complete information. When filling out the employee section, it’s crucial to include all relevant details such as the full name, social security number, and current address. Incomplete or inaccurate information can cause significant delays in processing claims.
Another mistake involves failing to report the accident promptly. The form requires details about when and where the accident occurred. If this information is missing or incorrect, it can create confusion for employers and insurance companies, complicating the claims process.
Not documenting the injury properly is also a frequent mistake. Employees should specify the exact part of the body that was injured and give a clear description of how the injury happened. If these sections are vague or unclear, it can weaken the claim.
Some individuals forget to include witness information. If there were witnesses to the accident, providing their names and contact details can support a claim significantly. Missing this information can hinder verification of the incident.
A misunderstanding of medical authorization is another issue. When signing the authorization for medical information, individuals need to understand what they are agreeing to. Some may fail to realize the implications of waiving their medical privacy rights by signing the form.
Another key mistake is not keeping a copy of the completed form. It is essential to retain a copy for personal records. Without this record, employees may find it challenging to follow up on their claim or address any issues that arise later.
Additionally, many people overlook the importance of submitting the form on time. The Arkansas Workers’ Compensation Commission has specific timelines for reporting injuries. Delays in submission can result in denial of benefits even if the claim is otherwise valid.
Some employees fail to ask for help when needed. Navigating the claims process and filling out forms can be confusing. Resources are available for those who need assistance, and ignoring these can lead to errors.
Finally, misunderstanding the choice and change of physician process can pose challenges. Employees should be clear about their rights to change physicians and the proper procedures for doing so. This understanding is crucial for receiving appropriate medical care and ensuring their claims are not negatively affected.
By being aware of these common mistakes, employees can improve their chances of a smooth claims process and ensure they receive the benefits they deserve.
Documents used along the form
When filing an injury claim under the Arkansas Workers’ Compensation system, the AR N form is essential. However, several other forms and documents often accompany it in this process. Each document serves a specific purpose, ensuring that the claim is processed efficiently and that both the employee and employer are aware of their rights and responsibilities.
- Employee’s Notice of Injury: This form allows employees to officially report their injury to their employer. It captures details such as the nature of the injury, the circumstances surrounding it, and witness information.
- Employer’s Notice to Employee: This document serves as a notification to the employee regarding their rights and how to report an injury. It is crucial that the employer provides a copy to the employee immediately to ensure they are informed of the necessary steps.
- Notice of Claim: Employees may need to submit this document to formally begin the claims process. It outlines the details of the injury and the requested benefits, ensuring the Workers’ Compensation Commission is aware of the claim.
- Request for Change of Physician: If an employee wishes to switch their medical provider, this form must be completed. It outlines the process for requesting changes and states the conditions under which a change can occur.
- Medical Authorization Release: This document allows medical providers to share information about the employee's injury with the employer or the Workers’ Compensation Commission. It helps streamline communication between all parties involved.
- Final Settlement Agreement: If a settlement is reached between the employee and the employer’s insurance, this form is signed to finalize the terms. It includes details about compensation and any ongoing medical coverage.
Utilizing these forms properly contributes significantly to the management of workers’ compensation claims in Arkansas. Understanding their roles can help ensure that both employees and employers navigate the complexities of the system more effectively.
Similar forms
The AR-N form relates to workers' compensation and injury reporting, similar to other key documents used in related contexts. Here’s a comparative list of documents that share similarities with the AR-N form:
- Workers’ Compensation Claim Form: This document initiates a claim for workers' compensation benefits, requiring details about the injury, treatment, and employer notification, much like the AR-N form.
- Employer's First Report of Injury: This form captures initial injury details as reported by the employer, ensuring compliance with notification requirements, paralleling the data collected in the AR-N.
- Employee Medical Release Form: This authorization allows healthcare providers to share medical information related to an employee's injury. Similar to the AR-N's authorization section, which permits disclosure of medical records.
- Incident Report Form: Used within organizations to document workplace accidents, this form collects information about the event, including witnesses and descriptions, which is also a focus of the AR-N.
- Physician's Certificate of Injury: This document confirms the nature and extent of an employee's injury, much like the medical information section in the AR-N that reviews treatment and condition.
- Change of Physician Request Form: This allows an employee to formally request a change in their treating physician, echoing similar provisions found in the AR-N form regarding physician choice and change.
- Return to Work Form: After an injury, this document indicates an employee's readiness to resume work. It may share a connection with the AR-N in terms of ensuring proper communication between the employee, employer, and medical providers.
- Independent Medical Examination (IME) Report: This report assesses an employee's injury from an impartial viewpoint, which works alongside the AR-N's inquiry into injuries and conditions for the claims process.
- Subrogation Claim Form: This form may be used when a third party is liable for an injury, linking directly to the employee's injury details and potential compensation outlined in the AR-N.
- Notice of Denial of Benefits: This document communicates to an employee the denial of their benefits claim, similar to the notification requirements in the AR-N regarding reporting injuries.
Dos and Don'ts
Filling out the AR N form correctly is crucial for ensuring that your injury is reported properly and that you receive the benefits you deserve. Here are nine important do's and don'ts to keep in mind:
- Do print clearly in ink to avoid any misunderstandings.
- Don't leave any sections blank. Ensure every required field is filled out.
- Do provide accurate and detailed information about the injury, including the cause and witnesses.
- Don't exaggerate or understate your injuries. Honesty is essential.
- Do sign and date the form to validate your statements and authorize medical information release.
- Don't forget to keep a copy of the completed form for your records.
- Do notify your employer immediately after the accident to ensure timely reporting.
- Don't assume your employer knows about your injury; provide a formal report as required.
- Do reach out to an AWCC legal advisor if you have questions about the process.
Taking these steps can help facilitate a smoother claims process and ensure that your rights are protected.
Misconceptions
- Misconception 1: The Ar N form is only for severe injuries.
- Misconception 2: The employer is responsible for filing the form.
- Misconception 3: Submitting the form guarantees benefits.
- Misconception 4: I cannot change my physician after filing.
- Misconception 5: Verbal notifications are sufficient for reporting injuries.
- Misconception 6: I have unlimited time to submit the form.
This perception often leads individuals to believe that only serious injuries warrant the completion of this form. In reality, any injury sustained at work, regardless of severity, should be reported using the Ar N form to ensure proper documentation and coverage under workers’ compensation.
Many employees assume that their employer will automatically handle the filing of the Ar N form. However, it is primarily the employee’s responsibility to report the injury promptly using the required form. Failure to do so can result in delays or denials of benefits.
Some individuals believe that submitting the Ar N form guarantees compensation for medical costs or lost wages. While filing the form is a necessary step, benefits are contingent upon meeting specific eligibility criteria, and approval is not guaranteed.
This misconception suggests that once the form is submitted, employees have no choice in their medical care. In fact, employees can request a change of physician under certain circumstances, according to the stipulations provided in the workers’ compensation guidelines.
Many people think that simply informing a supervisor verbally is adequate to report an injury. However, Arkansas law requires that a formal notification via the Ar N form be completed and submitted to ensure that the injury is documented and eligible for compensation.
Some employees may believe that they can take their time before submitting the Ar N form. However, timely reporting is crucial. Though the law allows for some exceptions, delays can jeopardize the claim and result in loss of benefits.
Key takeaways
When filling out the AR-N form, it's helpful to keep some key points in mind to ensure the process goes smoothly. Here are some important takeaways:
- Make sure to print clearly and use ink when filling out your personal information. This includes your name, social security number, and address.
- Details about your injury should be reported as soon as possible. The form must be submitted to your employer to notify them of the incident.
- Include the date and time of the accident in the appropriate fields. This information is crucial for your claim.
- Document everyone involved. List witnesses to the incident, as they can provide support to your claim.
- Be aware that any medical professional you authorize can share your relevant medical information. Your signature on the form grants permission for this.
- If you wish to change your physician, note the proper process. Following the correct steps is essential to ensure your treatment continues smoothly.
- Always keep a copy of the completed form. This could be useful for future references and tracking your claim.
- If you're unsure about any part of the process, assistance is available from the Arkansas Workers’ Compensation Commission.
- Remember, failing to notify your employer immediately can complicate your claim. Stay informed about your reporting requirements to avoid unnecessary issues.
By following these tips, you're setting yourself up for a clearer path during a challenging time. Filling out the AR-N form accurately can make a significant difference in the handling of your workers' compensation claim.
Browse Other Templates
Tax Exempt Office Depot - All details must match the information on your tax-exemption certificate for approval.
Uhc Global Claims Address - This form plays a vital role in tracking the details and treatment of vision care services provided.
Initial Return - The form is designed to assist in understanding both medical and employment considerations.