Fill Out Your C 3 Form
The C-3 form is a crucial document for employees in New York seeking workers' compensation benefits due to injuries sustained at work. By completing this form, individuals can initiate their claims and provide essential information about their incidents. It requires detailed responses regarding the employee's personal details, employer information, and specifics about the job at the time of the injury. Claimants must fill out sections that describe the nature of their injury or illness, the circumstances surrounding it, and any medical treatment received. Additionally, the form asks if there are any witnesses to the injury and details about the return to work. There’s also an acknowledgment of the legal implications associated with providing accurate information, emphasizing the seriousness of the claim process. Importantly, the C-3 can be completed online, making it accessible for those who may need assistance navigating the complexities of workers' compensation. Understanding the C-3 form is vital for anyone looking to secure their rights and benefits under New York's workers' compensation law.
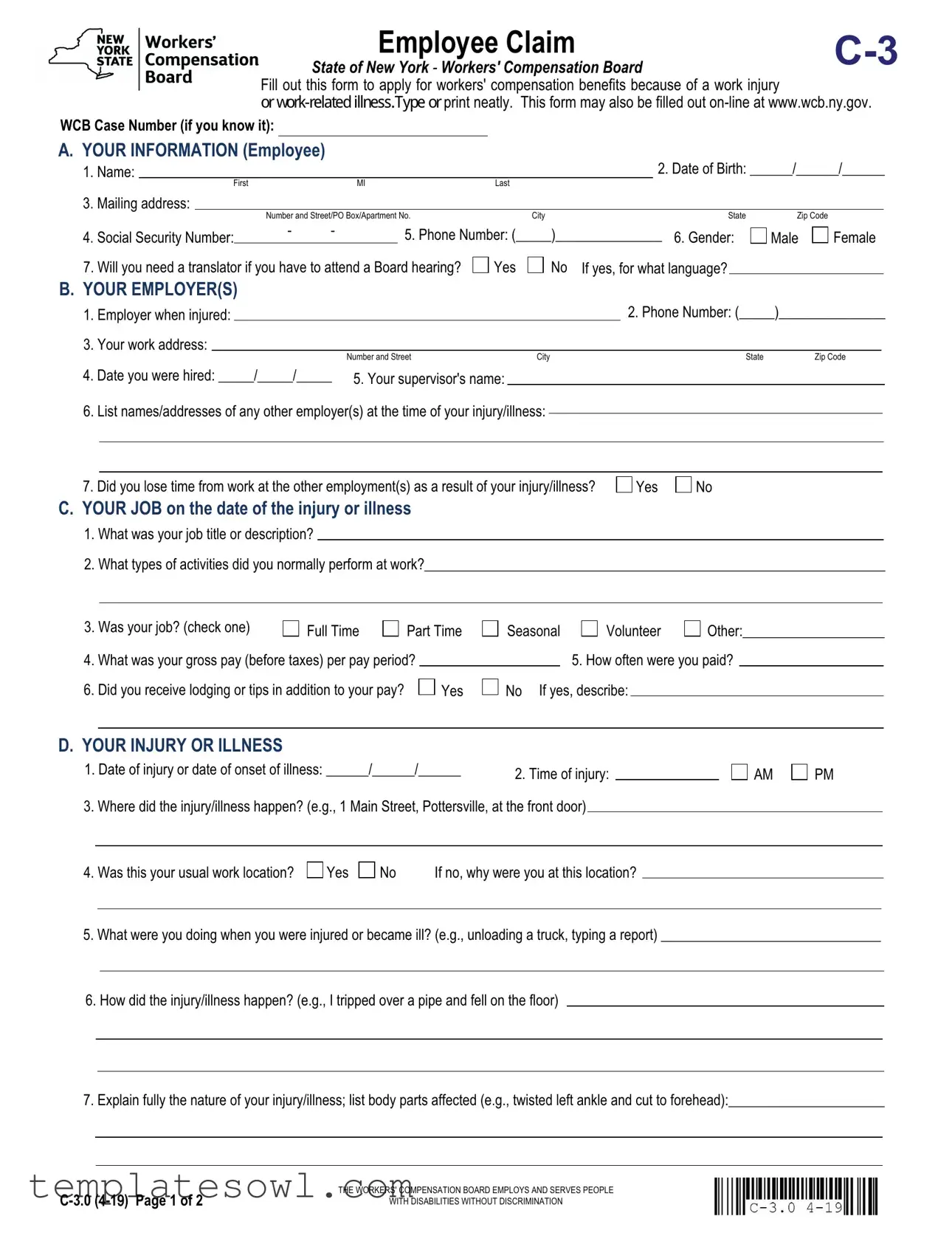
C 3 Example
Employee Claim |
|
State of New York - Workers' Compensation Board |
|
Fill out this form to apply for workers' compensation benefits because of a work injury
RUZRUNUHODWHG OOQHVV7\SHRUprint neatly. This form may also be filled out
WCB Case Number (if you know it):
A. YOUR INFORMATION (Employee)
1. |
Name: |
|
|
|
|
|
|
|
|
2. Date of Birth: ______/______/______ |
|||
|
|
|
First |
|
|
MI |
Last |
|
|
|
|
||
3. |
Mailing address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number and Street/PO Box/Apartment No. |
City |
State |
Zip Code |
|
||||
4. |
Social Security Number: |
|
- |
- |
|
5. Phone Number: (_____)_______________ |
6. Gender: |
Male |
Female |
||||
|
|
|
|
||||||||||
|
|
|
|
||||||||||
7. Will you need a translator if you have to attend a Board hearing? 
 Yes
Yes 
 No If yes, for what language?
No If yes, for what language?
B.YOUR EMPLOYER(S)
1. |
Employer when injured: |
|
|
2. Phone Number: (_____)_______________ |
|||
3. |
Your work address: |
|
|
|
|
|
|
|
|
|
Number and Street |
City |
State |
Zip Code |
|
4.Date you were hired: _____/_____/_____ 5. Your supervisor's name:
6.List names/addresses of any other employer(s) at the time of your injury/illness:
7. Did you lose time from work at the other employment(s) as a result of your injury/illness? |
Yes |
No |
C.YOUR JOB on the date of the injury or illness
1.What was your job title or description?
2.What types of activities did you normally perform at work?_________________________________________________________________
3. Was your job? (check one) |
Full Time |
Part Time |
Seasonal |
Volunteer |
Other:____________________ |
|||||
4. |
What was your gross pay (before taxes) per pay period? |
|
|
|
5. How often were you paid? |
|
||||
6. |
Did you receive lodging or tips in addition to your pay? |
|
Yes |
No If yes, describe: |
|
|
|
|||
|
|
|
|
|||||||
D. YOUR INJURY OR ILLNESS
1. Date of injury or date of onset of illness: ______/______/______ |
2. Time of injury: |
|
3. Where did the injury/illness happen? (e.g., 1 Main Street, Pottersville, at the front door)
AM
PM
4. Was this your usual work location? |
Yes |
No |
If no, why were you at this location? |
5.What were you doing when you were injured or became ill? (e.g., unloading a truck, typing a report) _______________________________
6.How did the injury/illness happen? (e.g., I tripped over a pipe and fell on the floor)
7.Explain fully the nature of your injury/illness; list body parts affected (e.g., twisted left ankle and cut to forehead):______________________
THE WORKERS' COMPENSATION BOARD EMPLOYS AND SERVES PEOPLE
WITH DISABILITIES WITHOUT DISCRIMINATION
YOUR NAME:________________________________________________ |
DATE OF INJURY/ILLNESS: ______/______/______ |
||||||||||||||||||||
|
|
|
|
First |
|
MI |
|
|
Last |
|
|
|
|
|
|
|
|
|
|
|
|
D. YOUR INJURY OR ILLNESS continued |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
8. |
Was an object (e.g., forklift, hammer, acid) involved in the injury/illness? |
Yes |
No If yes, what? |
|
|
|
|
|
|||||||||||||
9. |
Was the injury the result of the use or operation of a licensed motor vehicle? |
Yes |
|
No |
|
|
|
|
|
|
|||||||||||
|
|
|
If yes, |
your vehicle |
employer's vehicle |
other vehicle |
License plate number (if known): |
|
|
|
|
||||||||||
|
|
|
|
|
|||||||||||||||||
|
|
|
If your vehicle was involved, give name and address of your motor vehicle insurance carrier: |
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
10. |
Have you given your employer (or supervisor) notice of injury/illness? |
Yes |
No |
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
If yes, notice was given to: ____________________________________ |
orally |
in writing |
Date notice given: _____/_____/_____ |
||||||||||||||||
11. Did anyone see your injury happen? |
Yes |
No |
Unknown If yes, list names:________________________________________ |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
E. RETURN TO WORK |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
1. Did you stop work because of your injury/illness? |
|
Yes, on what date? _____/_____/_____ |
No , skip to Section F. |
||||||||||||||||||
2. Have you returned to work? |
Yes |
No |
If yes, on what date? _____/_____/_____ |
regular duty |
limited duty |
||||||||||||||||
3. If you have returned to work, who are you working for now? |
Same employer |
New employer |
Self employed |
||||||||||||||||||
4. What is your gross pay (before taxes) per pay period? |
|
|
|
|
How often are you paid? |
|
|
|
|
||||||||||||
F. MEDICAL TREATMENT FOR THIS INJURY OR ILLNESS |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
1. |
What was the date of your first treatment? ______/______/______ |
None received (skip to question |
|
|
|
||||||||||||||||
2. |
Were you treated on site? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
3. |
Where did you receive your first off site medical treatment for your injury/illness? |
none received |
Emergency Room |
||||||||||||||||||
|
|
|
|
Doctor's office |
|
Clinic/Hospital/Urgent Care |
|
|
Hospital Stay over 24 hours |
|
|
|
|||||||||
|
|
|
Name and address where you were first treated: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone Number: (_____)_______________ |
||||||
4. |
Are you still being treated for this injury/illness? |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Give the name and address of the doctor(s) treating you for this injury/illness: |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone Number: (_____)_______________ |
||||||
5. |
Have you had another injury to the same body part, or a similar illness? |
|
|
Yes |
No |
|
|
|
|
||||||||||||
|
|
|
If yes, were you treated by a doctor? |
Yes |
No |
If yes, provide the names and addresses of the doctor(s) who treated |
|||||||||||||||
|
|
|
you and COMPLETE AND FILE FORM |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. Was the previous injury/illness work related? |
Yes |
No |
|
If yes, were you working for the same employer that you work for now? |
Yes |
||
No
I am hereby making a claim for benefits under the Workers' Compensation Law. My signature affirms that the information I am providing is true and accurate to the best of my knowledge and belief.
Any person who knowingly and with INTENT TO DEFRAUD presents, causes to be presented, or prepares with knowledge or belief that it will be presented to, or by an insurer, or
Employee's Signature: |
|
Print Name: |
|
Date: _____/_____/_____ |
|
On behalf of Employee: |
|
Print Name: |
|
Date: _____/_____/_____ |
|
An individual may sign on behalf of the employee only if he or she is legally authorized to do so and the employee is a minor, mentally incompetent or incapacitated.
I certify to the best of my knowledge, information and belief, formed after an inquiry reasonable under the circumstances, that the allegations and other factual matters asserted above have evidentiary support, or are likely to have evidentiary support after a reasonable opportunity for further investigations or discovery.
Signature of Attorney/Representative (if any): |
|
|
|
|
|
|
Date: _______/_______/_______ |
||
|
|
Title: |
|
|
|||||
Print Name: |
|
|
|
|
|
|
|
||
ID No., if any: R |
|
|
If Licensed Representative, License No.: |
|
|
Expiration Date: _______/_______/_______ |
|||
|
|
|
|
||||||
Limited Release of Health Information |
|
(HIPAA) |
State of New York - Workers' Compensation Board
WCB Case No. (if you know it):___________________________
To Claimant: If you received treatment for a previous injury to the same body part or for an illness similar to the one described in your current Claim, fill out this form. This form allows the health care providers you list below to release health care information about your previous injury/ illness to your employer's workers' compensation insurer. The federal HIPAA law (Health Insurance Portability and Accountability Act of 1996) says you have a right to get a copy of this form. If you do not understand this form, talk to your legal representative. If you do not have a legal representative, the Advocate for Injured Workers at the Workers' Compensation Board can help you. Call:
To Health Care Provider: A copy of this
HIPAA.
This release is:
 Voluntary. Your health care provider(s) must give you the same care, payment terms, and benefits, whether you sign this form or not.
Voluntary. Your health care provider(s) must give you the same care, payment terms, and benefits, whether you sign this form or not.
 Limited. It gives your health care provider(s) permission to release only those health records that are related to the previous illness/condition you
Limited. It gives your health care provider(s) permission to release only those health records that are related to the previous illness/condition you
describe below.
 Temporary. It ends when your current claim for compensation is established or disallowed and all appeals are exhausted.
Temporary. It ends when your current claim for compensation is established or disallowed and all appeals are exhausted.
 Revocable. You can cancel this release at any time. To cancel, send a letter to the health care provider(s) listed on this form. Also, send a copy of your
Revocable. You can cancel this release at any time. To cancel, send a letter to the health care provider(s) listed on this form. Also, send a copy of your
letter to your employer's workers' compensation insurer and the Workers'
Compensation Board. Note: You may not cancel this release with respect to medical records already provided.
 For records only. It gives your health care provider(s) listed on this form permission to send copies of your health care records to your employer's
For records only. It gives your health care provider(s) listed on this form permission to send copies of your health care records to your employer's
workers' compensation insurer.
This form does NOT allow your health care provider(s) to release the following types of information:

 Psychotherapy notes
Psychotherapy notes
 Alcohol/Drug treatment
Alcohol/Drug treatment
 Mental Health treatment (unless you check below)
Mental Health treatment (unless you check below)
 Verbal information (your health care providers may not discuss your health care information with anyone)
Verbal information (your health care providers may not discuss your health care information with anyone)
Any medical records released will become part of your workers' compensation file and are confidential under the Workers' Compensation Law.
A.YOUR INFORMATION (Claimant)
1. Name:__________________________________________________________________ 2. Social Security
3. |
Mailing Address: _________________________________________________________________________________________________ |
4. |
Date of Birth: ______/______/______ 5. Date of the current injury/illness: ______/_______/_______ |
6.Current injury/illness, including all body parts injured:_____________________________________________________________________
______________________________________________________________________________________________________________
7.Your legal representative's name and address (if any):___________________________________________________________________
______________________________________________________________________________________________________________
Check here if you allow your health care provider(s) to release mental health care information.
B.YOUR HEALTH CARE PROVIDER(S) (List all health care providers who treated you for a previous injury to the same body part or similar illness. If more than 2 providers attach their contact information to this form.)
1.Provider:__________________________________________________________________ 2. Phone Number: (______)_______________
3.Mailing Address: _________________________________________________________________________________________________
4.Other provider (if any):_______________________________________________________ 5. Phone Number: (______)_______________
6.Mailing Address:_________________________________________________________________________________________________
C.READ AND SIGN BELOW. I hereby request that the health care provider(s) listed above give my employer's workers' compensation insurer copies of all health records related to any previous injury/illness, to all body parts, described above.
____________________________________________________________________________________________________________
Claimant's signature (ink only |
Date |
If the claimant is unable to sign, the person signing on his/her behalf must fill out and sign below:
______________________________________________________________________________________________________________
Your name |
Relationship to Claimant |
Signature (ink only |
Date |
Versión en español al reverso de la forma. |
www.wcb.ny.gov |
||
Divulgación limitada de información sobre la salud |
|
(HIPAA) |
Estado de NuevaYork - Junta de Compensación Obrera (WCB)
WCB Case No. (if you know it) (Número de caso WCB [si lo sabe])
Al reclamante: Si usted recibió tratamiento por una lesión anterior en la misma parte del cuerpo o por una enfermedad similar a la que motiva ahora su reclamación, complete este formulario. Este formulario les permite a los proveedores de salud que usted señala a continuación divulgar a la compañía de seguros de compensación obrera de su empleador la información sobre su salud relacionada con su lesión/enfermedad anterior. La Ley federal HIPAA (Ley de portabilidad y responsabilidad del seguro de salud de 1996) establece que usted tiene derecho a recibir una copia de este formulario. Si no comprende este formulario, hable con su representante legal. Si no tiene un representante legal, el
Representante de los obreros lesionados de la Junta de Compensación Obrera puede ayudarlo. Llame al
Al proveedor de salud: Una copia de esta divulgación, redactada según lo que establece la ley HIPAA, le permite divulgar información sobre la salud. Si envía los registros al asegurador de compensación obrera del empleador en respuesta a la presente divulgación, también debe enviar por correo copias al representante legal del reclamante. (Si a continuación no se especifica un representante legal, envíe las copias al reclamante). Los proveedores de salud que divulgan los registros deben cumplir con las leyes del estado de Nueva York y la HIPAA.
Esta divulgación es:
 Voluntaria. Su(s) proveedor(es) de salud deben otorgarle la misma atención, condiciones de pago y beneficios, independientemente de que usted firme este formulario o no.
Voluntaria. Su(s) proveedor(es) de salud deben otorgarle la misma atención, condiciones de pago y beneficios, independientemente de que usted firme este formulario o no.
 Limitada. Le otorga a su(s) proveedor(es) de salud permiso para divulgar únicamente los registros médicos que se relacionen con la enfermedad/ afección anterior que usted describe a continuación.
Limitada. Le otorga a su(s) proveedor(es) de salud permiso para divulgar únicamente los registros médicos que se relacionen con la enfermedad/ afección anterior que usted describe a continuación.
 Temporal. Termina cuando se otorgue o desestime su actual reclamación de compensación y se hayan agotado todas las apelaciones.
Temporal. Termina cuando se otorgue o desestime su actual reclamación de compensación y se hayan agotado todas las apelaciones.
 Revocable. Usted puede cancelar esta divulgación en cualquier momento. Para hacerlo, envíe una carta al (a los) proveedor(es) de salud que se indican en este formulario. Además, envíe una copia de su carta a la compañía de seguros de compensación obrera de su empleador y a la Junta
Revocable. Usted puede cancelar esta divulgación en cualquier momento. Para hacerlo, envíe una carta al (a los) proveedor(es) de salud que se indican en este formulario. Además, envíe una copia de su carta a la compañía de seguros de compensación obrera de su empleador y a la Junta
de Compensación Obrera. Nota: No podrá cancelar esta divulgación en lo que se refiere a registros médicos que ya se hayan provisto.
 Solamente para registros. Le otorga a su(s) proveedor(es) de salud que se indica(n) en este formulario permiso para enviar copias de sus registros de salud a la compañía de seguros de compensación obrera de su empleador.
Solamente para registros. Le otorga a su(s) proveedor(es) de salud que se indica(n) en este formulario permiso para enviar copias de sus registros de salud a la compañía de seguros de compensación obrera de su empleador.
Este formulario NO autoriza a su(s) proveedor(es) de salud a divulgar los siguientes tipos de información:
 Información relacionada con el VIH
Información relacionada con el VIH
 Notas de terapia psicológica
Notas de terapia psicológica
 Tratamientos por abuso de alcohol o drogas
Tratamientos por abuso de alcohol o drogas
 Tratamiento de salud mental (a menos que usted lo
Tratamiento de salud mental (a menos que usted lo
indique a continuación)
 Información verbal (sus doctores no pueden hablar
Información verbal (sus doctores no pueden hablar
con nadie sobre su información de salud)
Los registros médicos divulgados se incorporarán a su expediente de compensación obrera y son confidenciales conforme a la Ley de compensación obrera.
CONTESTA LAS SIGUIENTES PREGUNTAS, EN INGLÉS SI ES POSIBLE, EN LOS ESPACIOS PROVISTOS Y FIRMA AL FRENTE DE LA FORMA.
A. YOUR INFORMATION (Claimant) INFORMACIÓN PERSONAL (Reclamante)
1. Name (Nombre) |
2. Social Security Number (Número de seguro social) |
|
3. |
Mailing Address (Dirección postal) |
|
4. |
Date of Birth (Fecha de nacimiento) |
5. Date of the current injury/illness (Fecha de la lesión/enfermedad actual) |
6.Current injury/illness, including all body parts injured (Descripción de la lesión/enfermedad actual, incluyendo todas las partes del cuerpo lesionadas)
7.Your legal representative's name and address (if any) (Nombre y dirección de su representante legal [si corresponde])
Check here if you allow your health provider(s) to release mental health care information. (Marque aquí si autoriza a su(s) proveedor(es) de
salud a divulgar información sobre tratamientos de salud mental.)
B.YOUR HEALTH CARE PROVIDERS (List all health care providers who treated you for a previous injury to the same body part or similar illness. If more than 2 providers, attach their contact information to this form.
SU(S) PROVEEDOR(ES) DE SALUD (Enumere todos los proveedores de salud que le han tratado por lesiones previas a las mismas areas del cuerpo ó por enfermedades semejantes.Si son más de 2 proveedores, adjunte su información de contacto a este formulario.)
1. |
Provider (Proveedor de salud) |
2. Phone Number (No de teléfono) |
3. |
Mailing Address (Dirección postal) |
|
4.Other provider (if any) (Otro proveedor [si corresponde])
6.Mailing Adress (Dirección postal)
5. Phone Number (No de teléfono)
C. READ AND SIGN BELOW I hereby request that the health care provider(s) listed above give my employer's workers' compensation insurer copies of all health records related to any previous injury/illness, to all body parts, described above. LEA Y FIRME A CONTINUACIÓN. Por la presente solicito que los proveedores de salud aquí enumerados le provean al asegurador de compensación obrera de mi patrono copias de todos los records médicos relacionados a cualquier lesión/enfermedad aquí enumeradas.
If the claimant is unable to sign, the person signing on his/her behalf must fill out and sign below: (Si el reclamante no puede firmar, la persona que firme el formulario en su nombre y representación debe llenar y firmar a continuación)
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
Claimant's signature (Firma del reclamante ) use solo tinta - preferiblemente azulDate (Fecha)
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
Your name (Su nombre) |
Relationship to Claimant (Relación con el reclamante) |
Signature(Firma) |
Date(Fecha) |
www.wcb.ny.gov |
Instructions for Completing Employee Claim (Form
Please complete this form and send it to the Workers' Compensation Board centralized mailing address listed at the end of these instructions. If you need additional help completing this form, contact the Workers' Compensation Board at
Section A - Your Information (Employee):
In Section A, enter your name, address and other requested information.
Note on Item 7: Board hearings are conducted in English. If you need a translator, select Yes and indicate the language needed.
Notification Pursuant to the New York Personal Privacy Protection Law
(Public Officers Law Article
The Workers' Compensation Board's (Board’s) authority to request that claimants provide personal information, including their social security number, is derived from the Board’s investigatory authority under Workers' Compensation Law (WCL) § 20, and its administrative authority under WCL § 142. This information is collected to assist the Board in investigating and administering claims in the most expedient manner possible and to help it maintain accurate claim records. Providing your social security number to the Board is voluntary. There is no penalty for failure to provide your social security number on this form; it will not result in a denial of your claim or a reduction in benefits. The Board will protect the confidentiality of all personal information in its possession, disclosing it only in furtherance of its official duties and in accordance with applicable state and federal law.
Section B - Your Employer(s):
In Section B, enter the name, address, phone number and other information of the employer you were working for at the time of the injury/illness.
Note: Your employer is the company or agency that issues your paycheck. If you are a contractor at a work site or office, the staffing agency or vendor who hired you is your employer, not the work site or office where you report to work.
Section C - Your Job on the Date of the Injury or Illness:
In Section C, enter your job title, work activities and pay information.
Section D - Your Injury or Illness:
In Section D, enter your injury or illness information.
Item 1: Enter the date you were injured or the first date you noticed you became ill.
If this is an illness or occupational disease, skip item 2. The date you were injured must be in month/day/year format. The year should be written as four digits, e.g., 2015.
Item 2: Enter the time when the injury occurred. Check whether it was AM or PM.
Item 3: Indicate the location where the injury/illness occurred, including the address of the building and the physical location in the building where the injury/illness happened.
Item 4: Check whether this was your normal work location. If it was not, explain why you were at this location.
Item 5: Describe in detail what you were doing at the time of the injury/illness (e.g., unloading boxes from a truck by hand). This explains the events leading up to the injury.
Item 6: Describe in detail how the injury/illness occurred (e.g., I was lifting a heavy box off a truck). This should include all people and events involved in the injury/illness.
Item 7: Indicate fully the nature and extent of your injury/illness, including all body parts injured. Be as specific as possible (e.g., I strained my back trying to lift a heavy box. It hurts to bend over or hold even lighter objects now).
Item 8: Indicate if some object was involved in the accident other than a licensed motor vehicle. Other objects may include a tool (e.g., hammer), a chemical (e.g., acid), machinery (e.g., forklift or drill press), etc.
Item 9: Indicate if a licensed motor vehicle was involved in the accident. If so, check if the motor vehicle involved was yours, your employer's, or a third party's. Include the license plate number (if known). If your vehicle was involved, fill out the name and address of your automobile liability insurance carrier.
Item 10: Check if you gave your employer or supervisor notice of your injury or illness. If so, indicate who you gave notice to as well as if it was orally or in writing. Include the date you gave notice.
Item 11: Check if anyone else saw the injury happen. If anyone did see it, include their name(s).
Section E - Return to Work:
Item 1: If you stopped working as a result of your
Item 2: If you have since returned to work, check Yes. Also indicate on what date you started working again, as well as if you have returned to your Normal Duties or if you are on Limited or Restricted Duty. (If you have not returned to your full
Item 3: If you have returned to work, indicate who you are working for now.
Item 4: Enter your gross pay (before tax pay) per pay period for the job you are working at now. Indicate how often you are receiving a paycheck (weekly,
C‐3.0 (4‐19)
Section F - Medical Treatment for This Injury or Illness:
Item 1: If you did not receive medical treatment for this injury/illness, check None Received and skip to item 5. Otherwise, enter the date you first received treatment for this injury/illness and complete the rest of this section.
Item 2: Check if you were first treated on the job for this injury or illness.
Item 3: Check the location where you first received off site medical treatment for your injury or illness. Include the name and address of the facility as well as the phone number (including area code).
Item 4: If you are still receiving ongoing treatment for the same injury or illness, check Yes and indicate the name and address of the doctor(s) providing treatment as well as the phone number (including area code); otherwise, check No.
Item 5: If you already had an injury to the same body part or a similar illness, check Yes and indicate if you were treated by a doctor for this injury or illness. If you were treated by a doctor, indicate the name(s) and address(es) of the doctor(s) whom provided care and complete and file Form
Item 6: If you had a previous injury or illness, check if your previous injury or illness was
Sign Form
bottom of page 2.
What Every Worker Should Do in Case of
1.Immediately tell your employer or supervisor when, where and how you were injured.
2.Secure medical care immediately.
3.Tell your doctor to file medical reports with the Board and with your employer or its insurance carrier.
4.Make out this claim for compensation and send it to the nearest Workers' Compensation Board Office. (See below.) Failure to file within two years after the date of injury may result in your claim being denied. If you need help in completing this form, telephone or visit the nearest Workers' Compensation Board Office listed below.
5.Go to all hearings when notified to appear.
6.Go back to work as soon as you are able; compensation is never as high as your wage.
Your Rights:
1.Generally, you are entitled to be treated by a doctor of your choice, provided he/she is authorized by the Board. If your employer is involved in a preferred provider organization (PPO) arrangement, you must obtain initial treatment from the preferred provider organization which has been designated to provide health care services for workers' compensation injuries.
2.DO NOT pay your doctor or hospital. Their bills will be paid by the insurance carrier if your case is not disputed. If your case is disputed, the doctor or hospital must wait for payment until the Board decides your case. In the event you fail to prosecute your case or the Board decides against you, you will have to pay the doctor or hospital.
3.You are also entitled to be reimbursed for drugs, crutches, or any apparatus properly prescribed by your doctor and for carfares or other necessary expenses going to and from your doctor's office or the hospital. (Get receipts for such expenses.)
4.You are entitled to compensation if your injury keeps you from work for more than seven days, compels you to work at lower wages, or results in permanent disability to any part of your body.
5.Compensation is payable directly and without waiting for an award, except when the claim is disputed.
6.Injured workers or dependents of deceased workers may represent themselves in matters before the Board or may retain an attorney or licensed representative to represent them. If an attorney or licensed representative is retained, his/her fee for legal services will be reviewed by the Board and if approved will be paid by the employer or insurance company out of any compensation benefits due. Injured workers or dependents of deceased workers should not directly pay anything to the attorney or licensed representative representing them in a compensation case.
7.If you need help returning to work, or with family or financial problems because of your injury, contact the Workers' Compensation Board office nearest you and ask for a rehabilitation counselor or social worker.
This form should be filed by sending directly to the address listed below:
New York State Workers' Compensation Board
Centralized Mailing
PO Box 5205
Binghamton, NY
Customer Service
C‐3.0 (4‐19)
Form Characteristics
| Fact Name | Description |
|---|---|
| Form Purpose | This form is used to apply for workers' compensation benefits after a work-related injury or illness. |
| Governing Law | The C-3 form is governed by the New York Workers' Compensation Law. |
| Employee Information | Employees must fill out personal details, including name, mailing address, and date of birth. |
| Employer Details | It requires information about the employer at the time of injury, including contact details. |
| Injury Details | The form asks for specifics about the injury, including the date, time, and nature of the incident. |
| Medical Treatment | Claimants should provide details about their medical treatment, including the first treatment date and provider information. |
| Return to Work | It includes questions about whether the employee stopped working due to the injury or illness and if they have returned. |
Guidelines on Utilizing C 3
Completing the C-3 form is an essential step in applying for workers' compensation benefits in New York. This form requires specific information about your injury or illness, employment details, and medical treatment. After filling out the form, submit it to the Workers' Compensation Board mailing address provided in the instructions.
- Start by providing your name, date of birth, mailing address, social security number, and phone number in Section A.
- Indicate your gender and whether you will need a translator for any hearings.
- Proceed to Section B and enter the name and contact details of your employer when the injury occurred, including their phone number and address.
- Document your date of hire and your supervisor's name in this section. If applicable, list other employers at the time of your injury.
- In Section C, specify your job title and describe your job activities.
- Answer whether your job was full-time, part-time, seasonal, or another designation. Specify your gross pay before taxes and the frequency of your pay schedule.
- Move to Section D to provide details about your injury or illness, including the date and time it occurred, and explain how it happened.
- Indicate where the injury took place and confirm if it was your regular work location.
- Describe the nature of your injury and list any body parts affected.
- If applicable, mention whether an object was involved in the injury, and check if a licensed vehicle was involved, providing relevant details.
- Note if you've informed your employer or supervisor about the injury and include the date and method of notification.
- In Section E, state whether you stopped working due to the injury and provide dates for your return to work.
- Lastly, sign the form affirming that the information is accurate and true to the best of your knowledge.
What You Should Know About This Form
What is the purpose of the C-3 form?
The C-3 form is used to apply for workers' compensation benefits in New York State when an employee suffers a work-related injury or illness. By completing this form, you are formally notifying the Workers' Compensation Board of your claim and initiating the process to receive benefits for medical care and lost wages resulting from your injury or illness.
Who needs to fill out the C-3 form?
Any employee in New York who has been injured or become ill due to their work activities should complete the C-3 form. This includes full-time, part-time, and seasonal workers. It is essential for individuals who wish to obtain workers' compensation benefits to provide accurate and complete information on this form.
What information do I need to gather before completing the C-3 form?
Before filling out the C-3 form, gather the following information: your personal details (name, address, date of birth, Social Security number), employer details (company name, address, phone number), specifics about your job (title, duties, pay information), and detailed information about your injury or illness (date, time, location, description). Additionally, any previous injuries or ailments that might relate to your current claim should be documented.
How do I submit the C-3 form?
You can submit the C-3 form by mailing it to the Workers' Compensation Board. It is also possible to complete and submit the form online at www.wcb.ny.gov. Ensure that you keep a copy for your records. If you have questions while completing the form, consider reaching out to the Workers' Compensation Board at their help number: 1-877-632-4996.
What happens after I submit the C-3 form?
Once your C-3 form is submitted, the Workers' Compensation Board will review your claim. They may contact you for additional information or clarification if needed. You will receive a notice regarding the status of your claim, including whether it has been accepted or denied. If your claim is denied, you have the right to appeal their decision.
Can someone help me fill out the C-3 form?
Yes, you can seek assistance from a friend, family member, or a legal representative if you find the C-3 form challenging to complete on your own. The Workers' Compensation Board also offers resources and support for individuals who may have questions or need guidance. Additionally, the Advocate for Injured Workers can help; you can reach them at 800-580-6665.
What if I notice an error on my submitted C-3 form?
If you discover an error after submitting your C-3 form, you should contact the Workers' Compensation Board as soon as possible. They can guide you on how to correct the information. Timely updates will help ensure that your claim is handled accurately and without unnecessary delays.
Common mistakes
When filling out the C-3 form for workers' compensation claims in New York, avoiding mistakes is essential for a smooth process. Here are nine common missteps individuals often make that can delay their claim or create complications.
One frequent error is providing incomplete personal information. It's vital to ensure your name, address, phone number, and other details are accurate and fully filled out. Omissions can lead to delays or misunderstandings about your identity, potentially slowing down the processing of your claim.
Incorrectly identifying the employer at the time of the injury is another common issue. Applicants sometimes mistakenly indicate the wrong company, especially if they have worked for multiple employers. It’s critical to list the employer that issued your paycheck at the time of the injury to ensure proper processing.
Many claimants also neglect to document their injury details adequately. The section asking for the nature and cause of your injury needs comprehensive and specific descriptions. A vague explanation may leave room for interpretation and could hinder your claim. Ensure you detail what you were doing during the incident and the exact nature of your injuries.
Another common mistake is failing to provide the date and time of the injury accurately. These details are pivotal for establishing a timeline and context for your claim. If an applicant fails to enter this correctly, it can create significant complications during the review process.
Skipping sections or not answering all questions can also be problematic. Some individuals tend to overlook questions they think are not relevant to their case. However, every question serves a purpose in assessing your claim. Take the time to answer every question thoroughly, even if some seem less relevant.
Inconsistency between the information provided in different parts of the form can create confusion. For instance, if you indicate returning to work but state elsewhere that you still require medical treatment, this inconsistency could lead to questions about your eligibility. It's essential to ensure that all sections of the form correlate logically.
Many people also make the mistake of not indicating if any witnesses saw their injury occur. If you do not document this, your claim may lack additional support. Providing witness details can strengthen your case significantly.
Furthermore, individuals might forget to check if they require a translator for board hearings. If language barriers exist and this need is not communicated, it can pose challenges during hearings. Properly indicating this requirement is imperative for clear communication.
Finally, failing to sign and date the form is an all-too-common oversight. Without your signature, the Workers' Compensation Board cannot process your claim. Double-check that you have signed at the end of the form and that all dates are filled out correctly.
By being aware of these common mistakes and taking extra care while completing your C-3 form, you can help facilitate a smoother claims process and increase the chances of a favorable outcome.
Documents used along the form
The C-3 form is primarily used for applying for workers' compensation benefits in the State of New York. When completing this process, various additional forms and documents may also be required. Below is a list of other commonly used documents that are often submitted alongside the C-3 form to support your claim.
- Limited Release of Health Information (C-3.3): This form allows healthcare providers to disclose medical information related to previous injuries or illnesses to the employer’s workers' compensation insurer.
- Verification of Employee's Wage (C-5): This document verifies the employee’s earnings before the injury, helping to determine compensation amounts.
- Employer’s Report of Work-Related Injury (C-2): This document must be filed by the employer when an employee reports a work-related injury. It includes details about the incident.
- Claimant's Authorization for Release of Information (C-3.1): This form gives permission to the Workers' Compensation Board and insurance companies to obtain necessary information regarding the claim.
- Medical Report (C-4): A healthcare provider fills out this report. It documents the nature of the injury or illness and the treatment received.
- Follow-Up Medical Treatment Report (C-4.1): This form is used to document any additional or ongoing medical treatments related to the employee's injury.
- Notice of Indemnity (C-60): Used to inform the employee about compensation benefits and medical treatment under the Workers' Compensation Law.
- First Report of Injury (C-2.1): This document is submitted by employers and outlines the details of an injury from the employer’s perspective, including how and when it occurred.
- Hearing Request Form (C-6): This form can be used to request a hearing regarding disputes related to workers’ compensation claims.
Each document plays a role in the workers' compensation claims process. Completing and submitting them accurately can help ensure a smoother experience when seeking benefits.
Similar forms
- Form C-4: This form is used for a physician's report of an employee's injury. Like the C-3 form, it collects detailed information about the injury but from a medical perspective, outlining diagnosis, treatment, and prognosis.
- Form C-7: This document notifies the Workers' Compensation Board that an employee has returned to work. Similar to the C-3, it confirms the employee's work status and details regarding their job responsibilities post-injury.
- Form C-3.2: This form is a continuation of the C-3 process, seeking further information related to the injury. It is structured similarly but focuses on additional details that may arise after the initial claim.
- Form C-3.4: A notice of claim for repeat injuries. It operates similarly to the C-3 in that it gathers essential information about new or repeated injuries affecting the same body part as a prior claim.
- Form C-2: This form serves as a notice of accident report. It is similar in that it collects detailed specifics about the accident leading to a claim, providing context that may aid in the claims process.
- Form WCB-996: This document is used to release medical records related to the claim. It parallels the C-3 in the sense that it facilitates communication between medical providers and parties involved in the compensation process.
- Form WCB-5: This form serves to document the employee’s statement regarding the accident. It complements the C-3 by obtaining the employee's narrative of the incident, which helps clarify circumstances surrounding the claim.
- Form C-3.1: This is an extra informational request form, utilized if the Workers’ Compensation Board needs further explanations regarding the initial claim, similar to the C-3 in structure but requiring more specific answers.
- Form C-8A: A form used by employers to contest a claim. It mirrors the C-3 in its need for thoroughness and clarity but represents the employer's perspective in the process.
- Form C-7.1: This is issued when there is a need to assist injured workers who may require vocational rehabilitation services. It is similar in that it deals with the follow-up care after an injury, much like the C-3 which addresses immediate reporting of an injury.
Dos and Don'ts
- Do: Print neatly when filling out the C-3 form to ensure all information is legible.
- Do: Clearly describe the nature of your injury or illness with specific details about what happened.
- Don't: Leave any sections blank. If a particular question does not apply to you, indicate that by writing “N/A” or “Not applicable.”
- Don't: Provide false information or omit crucial details. Accuracy is vital for your claim to be processed properly.
By following these guidelines, you can help ensure that your application for workers' compensation goes smoothly. Remember, taking the time to do it right can make a significant difference.
Misconceptions
Misconception 1: The C-3 form is only for immediate injuries.
Many people believe that the C-3 form can only be used for accidents that happen on the job instantly. However, this form also accommodates claims for illnesses or injuries that develop over time due to workplace conditions. If you have ongoing health issues related to your job, don’t hesitate to file a claim with this form.
Misconception 2: Filling out the C-3 form is optional.
Some employees think that completing the C-3 form is merely a suggestion. On the contrary, if you've sustained an injury at work or have a work-related illness, it’s essential to fill out this form to ensure you receive the benefits you deserve. Delaying or skipping this step can jeopardize your claim.
Misconception 3: You can only submit the C-3 form through mail.
While mailing the C-3 form to the Workers' Compensation Board is one option, it's not the only one. You can also fill it out online at their website. This method can save time and ensure that your claim is filed promptly.
Misconception 4: Once submitted, the C-3 form can't be changed.
Another common belief is that once you submit the C-3 form, it's set in stone. But that’s not true. If you need to provide additional information or make corrections, you can update your claim later. Just make sure to keep the Board informed to avoid any complications.
Key takeaways
Here are some key takeaways about filling out and using the C-3 form:
- Provide Accurate Information: Ensure all personal details, such as your name and injury date, are correct. This prevents delays in processing your claim.
- Detailed Injury Description: Clearly describe your injury or illness. Include specifics about how and where it happened. The more detail, the better.
- Notify Your Employer: Inform your employer about your injury as soon as possible. This is crucial for eligibility and can impact your benefits.
- Understand Your Rights: You have the right to receive assistance in filling out the form. The Workers' Compensation Board is available to help if needed.
- Online Options: Consider filling out the C-3 form online at www.wcb.ny.gov for convenience. This can save time and ensure your information is legible.
Browse Other Templates
Satisfaction of Debt Letter - It's beneficial for a borrower to obtain this form after payment.
Utah State Tax Form for Employees - Part 2 is specifically for mineral production withholding reporting.
Small Business Workers Compensation Insurance Companies - Businesses must keep the U-26.3 updated in case of policy changes or renewals.