Fill Out Your Cdph 183 Form
The CDPH 183 form plays a crucial role in the certification process for Home Health Aides (HHA) in California. Designed by the California Department of Public Health, this form allows training programs to submit essential information about students who have successfully completed their HHA training. This includes both 40-hour and 120-hour programs. When schools or agencies submit this form, they must provide details such as the program start and end dates, along with the mailing address and identifying school code. A registered nurse, who oversees the training program, must sign the form to certify that the students meet the certification requirements. Personal information about the students, including their names, dates of birth, mailing addresses, and Social Security numbers, must also be accurately filled out. It is vital to remember that only this form should be sent to the Aide and Technician Certification Section; no additional forms are allowed. Understanding the importance of the CDPH 183 is essential for training programs aiming to help their students transition into licensed professionals in the healthcare field.
Cdph 183 Example
State of California- Health and Human Services Agency |
California Department of Public Health (CDPH) |
|
Licensing and Certification Program (L&C) |
|
Aide and Technician Certification Section (ATCS) |
|
MS 3301, P.O. Box 997416 |
|
Sacramento, CA |
|
PHONE: (916) |
|
Date sent: _________________ |
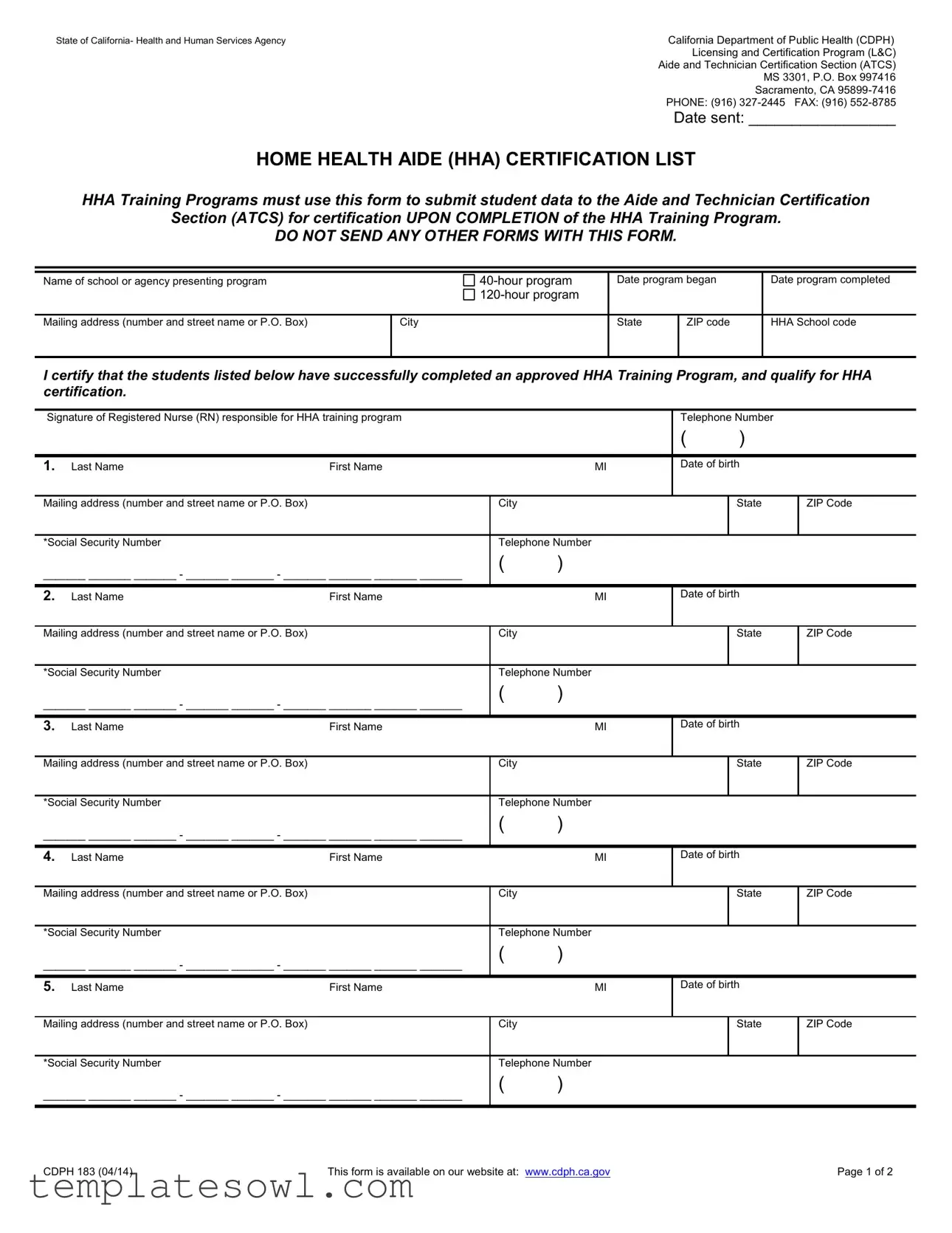
HOME HEALTH AIDE (HHA) CERTIFICATION LIST
HHA Training Programs must use this form to submit student data to the Aide and Technician Certification
Section (ATCS) for certification UPON COMPLETION of the HHA Training Program.
DO NOT SEND ANY OTHER FORMS WITH THIS FORM.
Name of school or agency presenting program
Date program began
Date program completed
Mailing address (number and street name or P.O. Box)
City
State
ZIP code
HHA School code
I certify that the students listed below have successfully completed an approved HHA Training Program, and qualify for HHA certification.
Signature of Registered Nurse (RN) responsible for HHA training program |
|
|
Telephone Number |
|
|||
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
1. |
Last Name |
First Name |
|
MI |
Date of birth |
|
|
|
|
|
|
|
|
|
|
Mailing address (number and street name or P.O. Box) |
|
City |
|
|
State |
ZIP Code |
|
|
|
|
|
|
|
||
*Social Security Number |
|
Telephone Number |
|
|
|
||
_______ _______ _______ - _______ _______ - _______ _______ _______ _______ |
( |
) |
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
2. |
Last Name |
First Name |
|
MI |
Date of birth |
|
|
|
|
|
|
|
|
|
|
Mailing address (number and street name or P.O. Box) |
|
City |
|
|
State |
ZIP Code |
|
|
|
|
|
|
|
||
*Social Security Number |
|
Telephone Number |
|
|
|
||
_______ _______ _______ - _______ _______ - _______ _______ _______ _______ |
( |
) |
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
3. |
Last Name |
First Name |
|
MI |
Date of birth |
|
|
|
|
|
|
|
|
|
|
Mailing address (number and street name or P.O. Box) |
|
City |
|
|
State |
ZIP Code |
|
|
|
|
|
|
|
||
*Social Security Number |
|
Telephone Number |
|
|
|
||
_______ _______ _______ - _______ _______ - _______ _______ _______ _______ |
( |
) |
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
4. |
Last Name |
First Name |
|
MI |
Date of birth |
|
|
|
|
|
|
|
|
|
|
Mailing address (number and street name or P.O. Box) |
|
City |
|
|
State |
ZIP Code |
|
|
|
|
|
|
|
||
*Social Security Number |
|
Telephone Number |
|
|
|
||
_______ _______ _______ - _______ _______ - _______ _______ _______ _______ |
( |
) |
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
5. |
Last Name |
First Name |
|
MI |
Date of birth |
|
|
|
|
|
|
|
|
|
|
Mailing address (number and street name or P.O. Box) |
|
City |
|
|
State |
ZIP Code |
|
|
|
|
|
|
|
||
*Social Security Number |
|
Telephone Number |
|
|
|
||
_______ _______ _______ - _______ _______ - _______ _______ _______ _______ |
( |
) |
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
CDPH 183 (04/14) |
This form is available on our website at: www.cdph.ca.gov |
Page 1 of 2 |
6. Last Name |
First Name |
MI |
Date of birth
Mailing address (number and street name or P.O. Box) |
|
City |
|
|
State |
ZIP Code |
|
|
|
|
|
|
|
||
*Social Security Number |
|
Telephone Number |
|
|
|
||
_______ _______ _______ - _______ _______ - _______ _______ _______ _______ |
( |
) |
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
7. |
Last Name |
First Name |
|
MI |
Date of birth |
|
|
|
|
|
|
|
|
|
|
Mailing address (number and street name or P.O. Box) |
|
City |
|
|
State |
ZIP Code |
|
|
|
|
|
|
|
||
*Social Security Number |
|
Telephone Number |
|
|
|
||
_______ _______ _______ - _______ _______ - _______ _______ _______ _______ |
( |
) |
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
8. |
Last Name |
First Name |
|
MI |
Date of birth |
|
|
|
|
|
|
|
|
|
|
Mailing address (number and street name or P.O. Box) |
|
City |
|
|
State |
ZIP Code |
|
|
|
|
|
|
|
||
*Social Security Number |
|
Telephone Number |
|
|
|
||
_______ _______ _______ - _______ _______ - _______ _______ _______ _______ |
( |
) |
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
9. |
Last Name |
First Name |
|
MI |
Date of birth |
|
|
|
|
|
|
|
|
|
|
Mailing address (number and street name or P.O. Box) |
|
City |
|
|
State |
ZIP Code |
|
|
|
|
|
|
|
||
*Social Security Number |
|
Telephone Number |
|
|
|
||
_______ _______ _______ - _______ _______ - _______ _______ _______ _______ |
( |
) |
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
10. |
Last Name |
First Name |
|
MI |
Date of birth |
|
|
|
|
|
|
|
|
|
|
Mailing address (number and street name or P.O. Box) |
|
City |
|
|
State |
ZIP Code |
|
|
|
|
|
|
|
||
*Social Security Number |
|
Telephone Number |
|
|
|
||
_______ _______ _______ - _______ _______ - _______ _______ _______ _______ |
( |
) |
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
11. |
Last Name |
First Name |
|
MI |
Date of birth |
|
|
|
|
|
|
|
|
|
|
Mailing address (number and street name or P.O. Box) |
|
City |
|
|
State |
ZIP Code |
|
|
|
|
|
|
|
||
*Social Security Number |
|
Telephone Number |
|
|
|
||
_______ _______ _______ - _______ _______ - _______ _______ _______ _______ |
( |
) |
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
12. |
Last Name |
First Name |
|
MI |
Date of birth |
|
|
|
|
|
|
|
|
|
|
Mailing address (number and street name or P.O. Box) |
|
City |
|
|
State |
ZIP Code |
|
|
|
|
|
|
|
||
*Social Security Number |
|
Telephone Number |
|
|
|
||
_______ _______ _______ - _______ _______ - _______ _______ _______ _______ |
( |
) |
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
(ATTACH ADDITIONAL SHEETS IF NECESSARY)
INFORMATION COLLECTION AND
*Social Security Number Disclosure: Pursuant to Section 666(a)(13) of Title 42 of the United States Code and California Family Code, Section 17520, subdivision (d), the California Department of Public Health (CDPH), is required to collect social security numbers from all applicants for nursing assistant certificates, home health aide certificates, hemodialysis technician certificates or nursing home administrator licenses. Disclosure of your social security number is mandatory for purposes of establishing, modifying, or enforcing child support orders upon request by the Health Integrity and Protection Date Bank as required by 45, CFR §61.1 et seq. Failure to provide your social security number
will result in the return of your application. Your social security number will be used by CDPH for internal identification, and may be used to verify information on your application, to verify certification with another state’s certification authority, for examination identification, for identification purposes in national disciplinary databases or as the basis of a
disciplinary action against you.
CDPH 183 (04/14) |
This form is available on our website at: www.cdph.ca.gov |
Page 2 of 2 |
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose | The CDPH 183 form is used by Home Health Aide (HHA) training programs to submit student data to the Aide and Technician Certification Section for certification upon completion of the training program. |
| Governing Law | This form is governed by California Health and Safety Code as well as federal regulations pertaining to healthcare certification. |
| Mandatory Information | The form requires specific information, including the name of the training program, dates of attendance, student names, Social Security numbers, and a signature from an RN responsible for the training. |
| Non-Submission of Other Forms | Users must not send any other forms along with the CDPH 183 form to ensure compliance and facilitate processing. |
| Privacy Statement | Disclosure of Social Security numbers is mandatory, per federal and state laws, to facilitate child support enforcement and for identification purposes. |
| Contact Information | For questions or additional information, users can contact the California Department of Public Health by phone at (916) 327-2445 or by fax at (916) 552-8785. |
Guidelines on Utilizing Cdph 183
Once you have gathered the necessary information, you will be ready to fill out the CDPH 183 form. It is important to complete this form accurately to ensure that the student data is submitted correctly for certification. Follow these steps closely for a successful submission.
- Enter the date you are sending the form.
- Write the name of the school or agency presenting the HHA program.
- Indicate whether the program is a 40-hour or 120-hour program by checking the appropriate box.
- Fill in the date the program began and the date it was completed.
- Provide the complete mailing address of the school or agency, including the city, state, and ZIP code.
- Input the HHA School code.
- Have the responsible Registered Nurse (RN) sign the form, certifying the students' completion.
- Fill in the RN’s telephone number.
- For each student being submitted, enter the following details:
- Last Name
- First Name
- Middle Initial (MI)
- Date of Birth
- Mailing Address (number and street name or P.O. Box)
- City
- State
- ZIP Code
- *Social Security Number
- Telephone Number
- After entering the details for each student, check that all information is accurate.
- If more than 12 students were part of the training program, attach additional sheets as necessary.
- Finally, send the completed form to the California Department of Public Health, Aide and Technician Certification Section, at the provided mailing address.
Completing this form accurately is crucial for your students' certification process. Ensure all the information is filled out correctly and submitted promptly to avoid delays.
What You Should Know About This Form
What is the Cdph 183 form used for?
The Cdph 183 form is used to submit student data for Home Health Aide (HHA) certification. HHA training programs must complete this form when their students finish the training program. The form helps the California Department of Public Health (CDPH) confirm that students have successfully completed an approved program and are eligible for certification.
Who is required to sign the Cdph 183 form?
A Registered Nurse (RN) who is responsible for the HHA training program must sign the Cdph 183 form. Their signature verifies that all the students listed on the form have completed the necessary training. This is an important step for maintaining the integrity of the certification process.
What information is needed on the Cdph 183 form?
The form requires specific information such as the name of the training school or agency, program duration (40-hour or 120-hour), start and completion dates, and mailing address. Additionally, each student’s name, date of birth, mailing address, Social Security number, and telephone number must be included. This detailed information helps the CDPH accurately track and verify student certifications.
Where can I find the Cdph 183 form?
The Cdph 183 form can be accessed on the California Department of Public Health's website. It's essential to ensure you are using the most current version of the form. Following your access, you should complete it carefully and submit it as required to avoid any processing delays.
Common mistakes
Completing the CDPH 183 form can feel overwhelming, but avoiding common mistakes can streamline the process. One frequent error occurs with the Social Security Number. Incomplete or incorrect entries can lead to application delays or rejections. Ensure that each number is clearly written and formatted correctly. Double-checking this crucial piece of information before submission is vital.
Another common oversight involves the date fields. Filling out the dates incorrectly can complicate verification efforts later on. Make sure to include the exact start and completion dates of the Home Health Aide Training Program. A simple mistake, like transposing numbers, can result in significant issues down the line.
Inaccurate contact information can also lead to issues. Applicants often neglect to verify the mailing address and phone number details. This can hinder communication from the California Department of Public Health regarding the certification status. It’s best to confirm that every entry is accurate to prevent unnecessary delays.
Some applicants forget to include the signature of the Registered Nurse responsible for the training program. This signature acts as a certification that the student has successfully completed the program, and its absence may cause the application to be deemed incomplete. Ensure this critical element is not overlooked.
Another oversight commonly seen is the failure to provide sufficient student data. In some cases, applicants miss providing information for all students listed on the form. Each spot should be filled out completely, even if there are blank fields for students who didn’t attend the program.
Applicants tend to confuse the correct HHA School Code as well. This detail is essential for proper identification of the training program. Incorrect or missing codes can create confusion and delays in processing the application.
Misplacing or failing to attach additional sheets can also be problematic. If the space allocated for student information is insufficient, applicants must ensure that extensions are attached as needed. Not doing so could result in missing information and hinder final approval.
One crucial area that sometimes gets overlooked is ensuring that all fields are complete for each student. Omissions can not only delay the processing of the application but can also raise questions regarding compliance. Full transparency in filling out every section is necessary.
Lastly, some individuals submit forms alongside other documents, which is explicitly discouraged. Always remember, to adhere to the instruction of submitting only the CDPH 183 form, without any additional documentation. This oversight can lead to issues during the review process.
By staying vigilant and carefully reviewing each detail of the CDPH 183 form, applicants can avoid common pitfalls. A thorough approach allows for a smoother certification process, helping students move forward in their Home Health Aide careers without unnecessary delays.
Documents used along the form
The Cdph 183 form is essential for home health aide certification in California. Alongside this form, several other documents are commonly used to ensure a smooth certification process. Each document has a specific purpose and helps maintain standards in training and certification.
- CDPH 402 Form: This form is used to apply for certification as a Nursing Assistant. It collects information about the applicant’s training and qualifications, similar to the Cdph 183 form but for nursing assistants specifically.
- CDPH 507 Form: The purpose of this form is to report and verify training program completion for various health care certifications. It details information about student performance, similar to the data required in the Cdph 183.
- CDPH 800 Form: This form is designed for applicants seeking a background check. It is crucial for ensuring the safety and integrity of care provided by health professionals. All applicants must complete this before certification.
- Verification of Training Completion: This document confirms that a student has finished the required training hours. It is typically signed by the RN responsible for the training program and ensures that students meet all necessary educational criteria before applying for certification.
Utilizing these documents along with the Cdph 183 form can streamline the certification process for home health aides. Having all necessary paperwork ready will facilitate a smoother transition into the workforce and enhance compliance with state requirements.
Similar forms
The CDPH 183 form, used for certifying home health aides, shares similarities with several other documents related to healthcare training and certification. Here’s a brief overview of those comparisons:
- Nursing Assistant Certification Form: Like the CDPH 183, this form collects essential data about students who have completed a nursing assistant training program, ensuring their eligibility for certification.
- Certified Medication Aide Application: This document requires schools to verify that students have completed a specific training curriculum, similar to how the CDPH 183 certifies completion of home health aide programs.
- Dialysis Technician Certification Application: Just as the CDPH 183 gathers student information for home health aides, this application requests details about trainees who have finished their dialysis technician program, fostering quality care in healthcare settings.
- Physical Therapy Aide Certification Form: This form serves to verify successful completion of a physical therapy aide program. It parallels the CDPH 183 by requiring responsibly sourced student data for certification purposes.
- Direct Support Professional Certification Form: Much like the CDPH 183, this form is used to confirm that applicants have fulfilled training requirements to work effectively in support roles in healthcare.
- Home Care Aide Registry Application: Similar to the CDPH 183, this application facilitates the registration of individuals who have completed a training program, ensuring that all home care aides meet state standards.
Dos and Don'ts
When filling out the CDPH 183 form, it is important to follow specific guidelines to ensure the form is completed correctly. Below is a list of things to do and avoid during the process.
- Do use the official CDPH 183 form provided by the California Department of Public Health.
- Do ensure that all required fields are filled out completely, including names, addresses, and Social Security numbers.
- Do obtain a signature from the Registered Nurse responsible for the HHA training program.
- Do double-check that the social security numbers are entered accurately, as errors may delay processing.
- Do keep a copy of the completed form for your records.
- Don’t submit any other forms along with the CDPH 183 form, as this can lead to processing issues.
- Don’t leave any mandatory fields blank; incomplete forms may be returned.
- Don’t forget to verify the dates for the training program, as they must align with the program completion.
- Don’t use ink that is faded or difficult to read; clarity is essential.
- Don’t submit the form without a valid mailing address, as this can cause delivery issues.
Misconceptions
- Misconception 1: The CDPH 183 form can be sent with other forms.
- Misconception 2: Social Security numbers are optional on the form.
- Misconception 3: The form is just a simple certification request.
- Misconception 4: Only the training program can fill out and submit the form.
Many people mistakenly think that they can submit the CDPH 183 form along with other documents. In reality, the instructions clearly state that no other forms should be sent with it. This is to ensure that the submission is processed efficiently and without confusion.
Some individuals believe that providing Social Security numbers is not necessary. However, the CDPH mandates that disclosure of Social Security numbers is mandatory for processing applications. Without it, the application will be returned.
While it might look straightforward, the CDPH 183 form is a crucial document that requires precise information. Each section must be filled out accurately to qualify for HHA certification, as any errors can delay the process.
Many assume that only authorized personnel from the training program can complete the form. However, anyone with the necessary information can assist in filling it out, but it must be signed by a Registered Nurse responsible for the training program to be valid.
Key takeaways
When filling out and using the CDPH 183 form for Home Health Aide (HHA) certification, it is crucial to adhere to several key guidelines to ensure proper submission and compliance with regulations.
- Use the correct form. Ensure you are using the CDPH 183 form specifically designed for HHA certification. Do not send any other forms with this submission.
- Accurate student information. Enter accurate information for each student, including their full name, date of birth, mailing address, Social Security number, and telephone number.
- Ensure program completion. The form must only be submitted after students have successfully completed the approved HHA training program. Verification from a Registered Nurse is required.
- Signature requirement. A Registered Nurse responsible for the training program must sign the form. This signature confirms that the student data is correct and they qualify for certification.
- Submit to the correct address. Mail the completed form to the Aide and Technician Certification Section (ATCS) at the designated address in Sacramento, California. Ensure timely delivery to avoid processing delays.
Understanding and adhering to these guidelines can facilitate a smooth certification process for prospective home health aides.
Browse Other Templates
How to Write Summary of a Project - Note the school’s name to ensure proper record-keeping.
Real Property Transfer Document,Property Transfer Declaration,Deed Transfer Report,Real Estate Transfer Form,Property Sale Statement,Transfer of Ownership Form,Deed Transaction Report,Property Transfer Notice,Ownership Change Certificate,Real Estate - Buyers can provide comments on the condition of the property as needed.
Kaiser Fmla - Ensure your email address is accurate for any follow-up communications.