Fill Out Your Cf Es 2282 Form
The CF-ES 2282 form serves as an essential tool for individuals seeking financial assistance through Medicaid and Medicare Buy-In programs. Filling it out accurately is crucial to ensure eligibility for benefits. The form includes sections for demographic information, where applicants must provide personal details such as names, Social Security numbers, and living addresses. It also inquires about marital status and asks for contact information for a support person. Additionally, the form covers technical details; applicants must disclose their date of birth, citizenship status, and whether they plan to remain in Florida. Importantly, the form delves into the applicant’s financial situation, requiring a detailed overview of assets and income, including employment details and any other insurance coverage. Understanding one’s rights and responsibilities is another vital aspect highlighted within the application. It ensures that applicants know their rights to assistance and what is expected of them to maintain eligibility. Failure to provide accurate information can lead to serious consequences, making it necessary for applicants to approach the form with care and attention.
Cf Es 2282 Example
|
Clear |
|
|
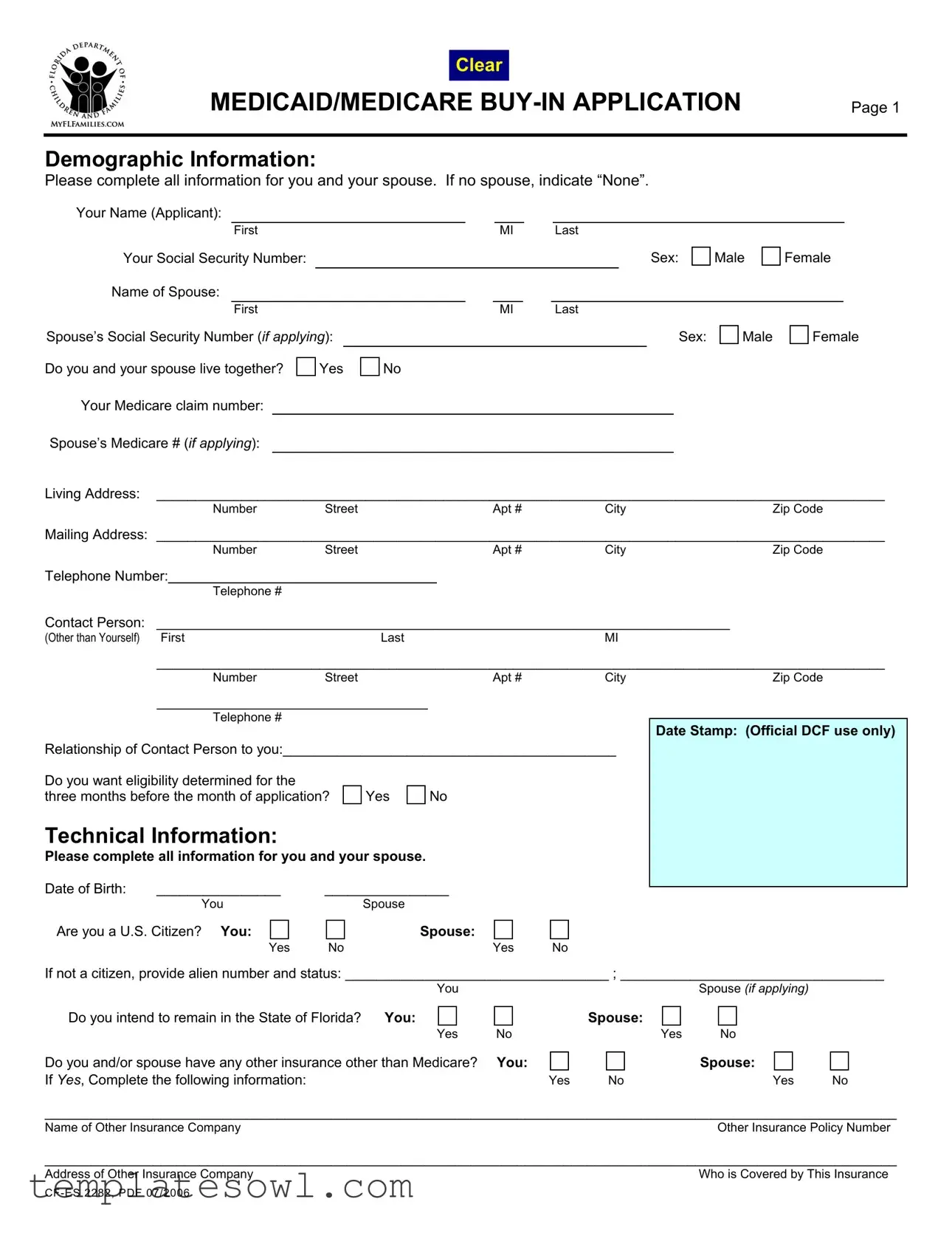
MEDICAID/MEDICARE |
Page 1 |
||
|
|
|
|
Demographic Information: |
|
||
Please complete all information for you and your spouse. If no spouse, indicate “None”. |
|
||
Your Name (Applicant):
First |
|
MI |
|
Last |
Your Social Security Number: |
|
Sex: |
Name of Spouse: |
|
|
Male
Female
|
First |
|
|
|
|
MI |
|
Last |
|
|
|
|||
Spouse’s Social Security Number (if applying): |
|
|
|
|
|
|
|
Sex: |
Male |
Female |
||||
Do you and your spouse live together? |
Yes |
No |
|
|
|
|
|
|
|
|||||
Your Medicare claim number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Spouse’s Medicare # (if applying): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Living Address: ______________________________________________________________________________________________
Number |
Street |
Apt # |
City |
Zip Code |
Mailing Address: ______________________________________________________________________________________________
NumberStreetApt #CityZip Code
Telephone Number:
Telephone #
Contact Person: |
__________________________________________________________________________ |
|
|||
(Other than Yourself) |
First |
Last |
|
MI |
|
|
______________________________________________________________________________________________ |
||||
|
Number |
Street |
Apt # |
City |
Zip Code |
___________________________________
Telephone #
Relationship of Contact Person to you:___________________________________________
Do you want eligibility determined for the |
|
|
three months before the month of application? |
Yes |
No |
Technical Information:
Please complete all information for you and your spouse.
Date of Birth: |
________________ |
________________ |
|
|
|
You |
Spouse |
|
|
Are you a U.S. Citizen? You: |
Spouse: |
|
|
|
|
Yes |
No |
Yes |
No |
Date Stamp: (Official DCF use only)
If not a citizen, provide alien number and status: __________________________________ ; __________________________________
You |
Spouse (if applying) |
Do you intend to remain in the State of Florida? You:
Yes
Do you and/or spouse have any other insurance other than Medicare? If Yes, Complete the following information:
Spouse:
NoYes No
You: |
|
Spouse: |
|
Yes |
No |
Yes |
No |
______________________________________________________________________________________________________________
Name of Other Insurance CompanyOther Insurance Policy Number
______________________________________________________________________________________________________________
Address of Other Insurance Company |
Who is Covered by This Insurance |
|

|
|
|
|
|
Page 2 |
Asset Information: Please list all assets owned by you and/or spouse (even if your spouse is not applying). |
|||||
TYPE |
NAME OF BANK/ |
ADDRESS |
ACCOUNT NUMBER |
VALUE OF |
IN WHOSE NAME |
|
FINANCIAL INSTITUTION |
|
|
ASSET |
IS IT HELD |
CASH |
|
|
|
|
|
|
|
|
|
|
|
SAVINGS ACCOUNT |
|
|
|
|
|
|
|
|
|
|
|
CHECKING ACCOUNT |
|
|
|
|
|
|
|
|
|
|
|
CAR |
|
|
|
|
|
Make/Model/Year: |
|
|
|
|
|
|
|
|
|
|
|
HOMESTEAD |
|
|
|
|
|
|
|
|
|
|
|
OTHER PROPERTY |
|
|
|
|
|
|
|
|
|
|
|
TRUST FUND |
|
|
|
|
|
|
|
|
|
|
|
STOCKS/BONDS |
|
|
|
|
|
|
|
|
|
|
|
TAX SHELTERED |
|
|
|
|
|
ACCOUNTS |
|
|
|
|
|
LIFE INSURANCE |
|
|
|
|
|
|
|
|
|
|
|
KEOGH PLAN |
|
|
|
|
|
|
|
|
|
|
|
Other: Please Specify |
|
|
|
|
|
|
|
|
|
|
|
Income Information: Please complete all information for you and your spouse (even if spouse is not applying).
Are you or your spouse
Applicant
Yes |
No |
Gross Amount |
|
|
Earned Monthly |
Spouse
Yes |
No |
Gross Amount |
|
|
Earned Monthly |
Do you or your spouse work for someone else?
Applicant
Yes |
No |
Gross Amount |
|
|
Earned Monthly |
Spouse
Yes |
No |
Gross Amount |
|
|
Earned Monthly |
Do you or your spouse receive income from any of the following? |
|
|
|
Gross Amount Received Each Month |
|||
|
|
(Before Any Deductions) |
|
Type |
Benefit No. |
Applicant |
Spouse |
Veterans Benefits |
|
|
|
Pension |
|
|
|
Interest/Dividends |
|
|
|
Civil Service Annuity |
|
|
|
Income from another person |
|
|
|
Black Lung |
|
|
|
Social Security |
|
|
|
Other (e.g. SSI, Annuities): (specify) |
|
|
|
|
|
|
|
Page 3
YOUR RIGHTS AND RESPONSIBILITIES: Read this sheet before you sign your name.
YOU HAVE THE RIGHT TO:
•Apply for assistance and have a determination of your eligibility made without regard to race, color, sex, age, handicap, religion, national origin, marital status or political belief.
•Have a representative help you fill out the eligibility forms.
•Have action taken on your application promptly and be notified of such action.
•Be informed of other available services of the Department of Children and Families.
•Request a fair hearing when you disagree with a decision of the Department of Children and Families.
•Have the information about you and/or your spouse that is collected by the department treated confidentially in accordance with federal and state laws.
YOU HAVE THE RESPONSIBILITY TO (things you must do):
•Assist in determining your eligibility by giving complete and correct information and provide written proof of information, as requested, within the time limits given.
•Declare the citizenship or alien status for you and your spouse by signing the Medicaid/Medicare
•File for any payments or benefits from other sources if this application, or other information, indicates that you or your spouse may be eligible for such payments or benefits.
•Assign your rights to third party benefits and cooperate in reporting any insurance or other health plan that covers medical costs for you (and/or your spouse, if applying) unless good cause can be shown not to do so.
•Report changes in your situation (e.g., income, assets) within 10 days of the change.
•Report your (and your spouse’s, if applying) Social Security numbers. Without accurate numbers, we will be unable to provide Medicaid/Medicare
IMPORTANT INFORMATION ABOUT MEDICAID:
Any person (including the designated representative) who knowingly withholds information or knowingly misrepresents the truth may be punished under federal or state law or both. If you get medical assistance for which you do not qualify, you may have to repay the cash value of that assistance.
Certification of Citizenship/Alien Status: I certify, under the penalty of perjury, by signing my name on this application, that I and my spouse (if applicable) are U.S. citizens or nationals of the United States or qualified aliens.
Certification: In signing this application, I swear and affirm, under penalty of perjury, that the information I have given on this application is correct and complete to the best of my knowledge. I have read and understand the above rights and responsibilities and important information about Medicaid.
Applicant |
Go Back To Page 1 |
|
|||||
|
|
|
|
||||
Signature: |
|
|
Date: |
|
|||
Spouse |
|
|
|
|
|
||
Signature: |
|
|
Date: |
|
|||
|
|
|
|
|
|
|
|
Designated |
|
|
|
|
|||
Representative Signature: |
|
|
Date: |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
HELPING PERSON: (Official use only) |
|
|
|
|
|||
|
|
|
|
|
Date: |
|
|
|
|
|
|
|
|
|
|
Signature of Individual Who Assisted Applicant in Completing
In accordance with Federal law and our policy, the Department of Children and Families is prohibited from discriminating on the basis of race, color, national origin, sex, age, disability, religion, political belief, or marital status.
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose | The CF-ES 2282 form is a Medicaid and Medicare Buy-In Application designed to determine eligibility for assistance in paying Medicare premiums. |
| Eligibility | Eligibility is determined based on the applicant’s income, assets, and residency status. Both spouses must provide information even if only one is applying. |
| Personal Information | The form collects essential personal details such as name, Social Security numbers, birthdays, and citizenship status for both the applicant and spouse. |
| Assets Disclosure | Applicants must list all assets they and/or their spouse own, including bank accounts, properties, and other financial holdings. |
| Rights and Responsibilities | Applicants have rights, including receiving assistance without discrimination, and responsibilities, such as providing accurate information and reporting changes. |
| Governing Law | This form is governed under Florida Medicaid law, particularly as it relates to insurance and healthcare assistance programs. |
Guidelines on Utilizing Cf Es 2282
Filling out the CF-ES 2282 form is an important step in the process of applying for Medicaid/Medicare Buy-In. Once the form is completed, it will be submitted to the appropriate agency for review. It’s crucial to ensure all sections are filled out accurately to avoid delays in processing.
- State your personal information clearly, starting with your name, Social Security number, sex, and the name and details of your spouse if applicable.
- Indicate whether you and your spouse live together, and provide your Medicare claim number and your spouse’s Medicare number if applicable.
- Fill in your living and mailing addresses precisely, along with your telephone number and contact person’s information.
- Decide if you want eligibility to be determined for the three months prior to the application month and mark your choice.
- Provide demographic information, including dates of birth and U.S. citizenship status for yourself and your spouse.
- List any other insurance coverage, and provide the name and address of the insurance company, along with the policy number and who is covered.
- Detail all assets owned by you and your spouse, including account types, financial institution names, account numbers, and their values.
- Document income information for you and your spouse by indicating self-employment status and any other sources of income, including the gross amounts received monthly.
- Read through your rights and responsibilities carefully to understand what is expected of you during this process.
- Affirm the correctness of the provided information by signing the application. Include the dates of your signatures and those of your spouse if applicable.
- If needed, have the designated representative sign to confirm their assistance in completing the application.
What You Should Know About This Form
What is the CF-ES 2282 form used for?
The CF-ES 2282 form is utilized as the Medicaid and Medicare Buy-In Application. Individuals seeking financial assistance for medical costs may use this form to apply for eligibility under Medicaid or Medicare programs. By completing this application, you express your interest in receiving benefits that help cover medical expenses, while also providing essential demographic, asset, and income information required for assessment.
Who needs to complete this form?
This form must be filled out by anyone applying for Medicaid or Medicare Buy-In benefits. If you have a spouse, both your information and your spouse’s details should be included in the application. If you are single, simply indicate “None” where asked about your spouse. Accurate information is crucial, as it determines your eligibility for the programs.
Are there any important responsibilities I should be aware of when completing this application?
Yes, applicants have specific responsibilities. You must provide complete and accurate information about your financial status and living situation. If there are changes in your income or assets, you are required to report these within 10 days. Additionally, you must declare your citizenship status and may need to cooperate by assigning rights to any third-party benefits that could assist with your medical costs. Remember, withholding information may result in penalties.
What rights do I have while filling out this application?
As an applicant, you have several rights. You have the right to apply without discrimination based on factors such as race or religion. You can seek assistance in completing the forms and expect prompt action on your application. If you disagree with any decisions made regarding your eligibility, you are entitled to request a fair hearing. Furthermore, your personal information is protected under confidentiality laws, ensuring your data is treated with care throughout the application process.
Common mistakes
When filling out the CF ES 2282 form, individuals often make mistakes that can delay the application process. One common error is not completing all demographic information. This includes the applicant's name, address, and social security number. Incomplete sections can lead to misunderstandings and delays in processing the application.
Another frequent mistake is not providing accurate information regarding spouse details. Applicants sometimes forget to indicate “None” when they do not have a spouse. This oversight can cause confusion about eligibility and affect the assessment of the application.
A significant number of people also forget to indicate whether they and their spouse live together. This question is essential for determining eligibility. Without a clear answer, the application cannot be assessed correctly.
Failing to provide information about other insurance can be problematic as well. Many applicants neglect to mention any additional insurance policies they or their spouse may have. This information is crucial because it can impact coverage decisions and benefits.
Some applicants mistakenly skip the asset information section. Listing all assets, regardless of whether the spouse is applying, is mandatory. Incomplete information here can lead to further questioning or request for additional documentation.
Improperly reporting income is another critical error. Individuals must accurately state their monthly earnings and any benefits received. Misreporting could result in penalties or denial of benefits.
Additionally, applicants often overlook the requirement to report their Social Security numbers. Providing incorrect or missing Social Security numbers may prevent benefits from being granted, so accuracy is vital.
Another mistake is not signing the application or delaying the submission. All parties must read the rights and responsibilities section and sign it. Failing to sign can render the application invalid.
Lastly, misunderstanding the changes in circumstances can lead to errors. Applicants should report any changes in income or assets within ten days. Not doing so might result in complications or a loss of benefits.
Documents used along the form
The CF ES 2282 form, designed for the Medicaid and Medicare Buy-In application process, typically requires several supporting documents to provide a complete picture of an applicant's situation. Below is a list of commonly used documents alongside the CF ES 2282 form, each serving an important role in the application process.
- Proof of Citizenship or Alien Status: This document verifies the citizenship or immigration status of the applicant and any spouse applying. Acceptable forms include a birth certificate, passport, or immigration documents.
- Social Security Administration Records: These records can confirm eligibility and payment history regarding Social Security benefits for the applicant and spouse.
- Income Verification Documents: Required to establish financial eligibility, these can include pay stubs, tax returns, and bank statements detailing income from all sources.
- Asset Documentation: Applicants must provide information regarding assets, such as property deeds, bank account statements, and investment records, to assess their financial situation accurately.
- Health Insurance Information: This includes policy numbers, names of insurance companies, and coverage details for any existing health insurance besides Medicare, relevant to determining eligibility for the Buy-In program.
- Power of Attorney or Designation of Representative: If a representative assists the applicant in the application process, a legal document indicating authority to act on behalf of the applicant may be required.
Each of these documents plays a crucial role in assessing eligibility for Medicaid and Medicare Buy-In benefits. Ensuring all necessary paperwork is accurately completed and submitted can streamline the application process, reducing delays in receiving benefits.
Similar forms
- CF-ES 2035: Application for Public Assistance - This form initiates the process for individuals seeking various types of public assistance, similar to the CF ES 2282 by collecting demographic, income, and asset information from applicants.
- CF-ES 2330: Application for Food Assistance - This document, like the CF ES 2282, gathers personal and financial details to determine eligibility for food assistance benefits, ensuring a comprehensive review of the applicant's situation.
- Medicaid Application for Financial Assistance - This application also requests detailed information about income and assets, akin to the CF ES 2282, to assess eligibility for Medicaid services.
- CF-ES 2070: Request for Services - Individuals seeking services must provide information regarding their needs and circumstances, similar to the CF ES 2282, to help service providers understand the applicant's situation.
- CF-ES 2056: Child Care Assistance Application - This form, focused on child care assistance, similarly collects crucial financial and demographic data, mirroring the approach taken by the CF ES 2282 for assessing eligibility.
- Medicare Part D Extra Help Application - This application assesses eligibility for assistance with Medicare prescription drug costs, requiring similar personal and financial details as the CF ES 2282 to determine qualification for benefits.
Dos and Don'ts
When filling out the CF-ES 2282 form, it is essential to follow some guidelines to ensure the process goes smoothly. Below is a list of things you should and shouldn't do.
- Do complete all sections fully, including details for both the applicant and spouse if applicable.
- Do provide accurate Social Security numbers for yourself and your spouse.
- Do report any changes in income or assets within 10 days of the change.
- Do declare your citizenship or alien status clearly on the form.
- Don't leave any sections blank unless specified; incomplete information can delay processing.
- Don't sign the application without reviewing all the information for accuracy first.
Misconceptions
There are several misconceptions surrounding the CF-ES 2282 form, which is crucial for individuals applying for Medicaid or Medicare buy-in. Understanding these misconceptions can provide clarity and help applicants successfully navigate the process.
- Misconception 1: Only individuals currently receiving Medicare can apply.
- Misconception 2: The information required is excessive and not necessary.
- Misconception 3: Assistance will automatically be granted once the form is submitted.
- Misconception 4: I can skip questions if I think they are irrelevant.
- Misconception 5: It is not possible to have a representative assist in the application process.
Many believe that only those already enrolled in Medicare can fill out the CF-ES 2282 form. In reality, this form is specifically designed for those seeking assistance with their Medicare premiums and potentially eligible for Medicaid, regardless of their current enrollment status in Medicare.
Some applicants feel overwhelmed by the amount of information requested. However, each piece of information serves a purpose in assessing eligibility. Precise details about assets and income ensure that the application is processed accurately and efficiently. Providing accurate information can lead to timely assistance.
Many applicants think that submitting the CF-ES 2282 guarantees that they will receive assistance. However, eligibility is determined based on the information provided, and a decision will be communicated following a thorough review.
Some individuals believe it is acceptable to omit questions they deem unnecessary. Completing every section of the form is essential. Missing information can delay processing or even lead to denial of benefits, as all aspects of an applicant's financial situation are essential for eligibility determination.
There is a common belief that applicants must complete the form independently. However, applicants are allowed to have representatives assist them in filling out the application. This support can be invaluable, particularly for those who may find the process confusing or challenging.
Being informed about these misconceptions may ease concerns and enhance the overall application experience for those seeking assistance through the CF-ES 2282 form.
Key takeaways
When filling out the CF-ES 2282 form, keep these key takeaways in mind:
- Begin by providing complete demographic information for both you and your spouse, if applicable.
- Make sure to include Social Security numbers, as they are essential for processing your application.
- Clearly indicate whether you and your spouse currently live together.
- Consider whether you want eligibility decided for the three months prior to your application date.
- Report all assets accurately, as this information will help determine your eligibility for benefits.
- List any income sources, including self-employment and benefits, and provide gross amounts received each month.
- Understand and acknowledge your rights and responsibilities as outlined in the application.
- Provide accurate citizenship or alien status information for you and your spouse to avoid issues later.
- Any changes in income or assets must be reported within 10 days to maintain eligibility.
- Sign the application, confirming the information supplied is correct and complete to the best of your knowledge.
Completing the form thoughtfully and accurately will help in processing your Medicaid or Medicare buy-in benefits smoothly.
Browse Other Templates
Hunting Access Agreement,Landowner Hunting Authorization,Hunting Consent Form,Property Access Hunting Release,Hunting Authorization Document,Landowner's Hunting Permit,Hunter Access Permission Slip,Hunting Land Use Agreement,Permission to Hunt Form,H - This agreement fosters a respectful relationship between landowners and hunters.
Renew Handicap Parking Permit Florida Online - Properly completed applications expedite the process of obtaining permits.