Fill Out Your Cms 671 Form
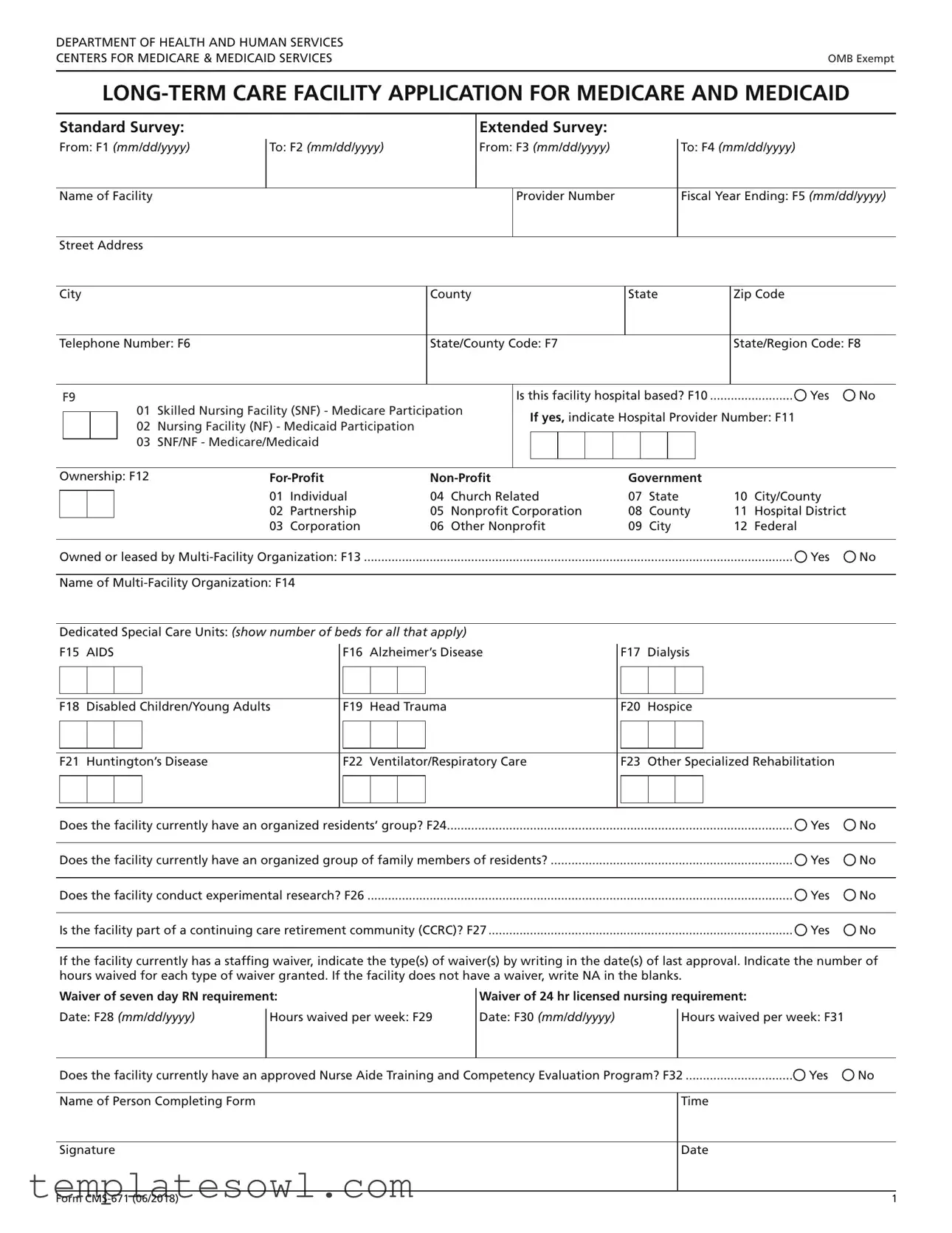
The CMS 671 form is a vital document for long-term care facilities seeking certification for Medicare and Medicaid services. It plays a significant role in the standard and extended survey processes, ensuring that facilities comply with the necessary regulations that govern their operation. This form captures essential information about the facility, including its name, location, and unique identifiers, such as the provider number. The form also addresses critical operational factors, such as ownership type—whether for-profit, non-profit, or government-run—and whether the facility is part of a larger multi-facility organization. Furthermore, it collects data on specialized care units that cater to specific health conditions and the presence of organized groups for residents and families. The CMS 671 form even considers staffing requirements and training programs, thereby facilitating a comprehensive assessment of the facility's capabilities and compliance status. Successfully completing this form is essential for any facility aiming to provide quality care while participating in federally funded programs.
Cms 671 Example
DEPARTMENT OF HEALTH AND HUMAN SERVICES |
|
CENTERS FOR MEDICARE & MEDICAID SERVICES |
OMB Exempt |
Standard Survey:
From: F1 (mm/dd/yyyy)
To: F2 (mm/dd/yyyy)
Extended Survey:
From: F3 (mm/dd/yyyy)
To: F4 (mm/dd/yyyy)
Name of Facility
Provider Number
Fiscal Year Ending: F5 (mm/dd/yyyy)
Street Address
City |
|
|
County |
|
|
|
|
|
State |
Zip Code |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Telephone Number: F6 |
|
State/County Code: F7 |
|
|
|
|
|
State/Region Code: F8 |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
F9 |
|
|
|
|
Is this facility hospital based? F10 |
|
Yes |
No |
||||||||||||
|
|
|
|
01 |
Skilled Nursing Facility (SNF) - Medicare Participation |
|
If yes, indicate Hospital Provider Number: F11 |
|
|||||||||||||
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
02 |
Nursing Facility (NF) - Medicaid Participation |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
03 |
SNF/NF - Medicare/Medicaid |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ownership: F12 |
|
|
|
|
|
Government |
|
|
|
||||||||||||
|
|
|
|
|
01 |
Individual |
04 |
Church Related |
07 |
State |
10 |
City/County |
|
||||||||
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
02 |
Partnership |
05 |
Nonprofit Corporation |
08 |
County |
11 |
Hospital District |
|
||||||||
|
|
|
|
|
03 |
Corporation |
06 |
Other Nonprofit |
09 |
City |
12 |
Federal |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Owned or leased by |
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Name of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Dedicated Special Care Units: (show number of beds for all that apply)
F15 AIDS
F16 Alzheimer’s Disease
F17 Dialysis
F18 Disabled Children/Young Adults
F19 Head Trauma
F20 Hospice
F21 Huntington’s Disease
F22 Ventilator/Respiratory Care
F23 Other Specialized Rehabilitation
Does the facility currently have an organized residents’ group? F24 |
Yes |
No |
|
|
|
Does the facility currently have an organized group of family members of residents? |
Yes |
No |
|
|
|
Does the facility conduct experimental research? F26 |
Yes |
No |
|
|
|
Is the facility part of a continuing care retirement community (CCRC)? F27 |
Yes |
No |
If the facility currently has a staffing waiver, indicate the type(s) of waiver(s) by writing in the date(s) of last approval. Indicate the number of hours waived for each type of waiver granted. If the facility does not have a waiver, write NA in the blanks.
Waiver of seven day RN requirement:
Date: F28 (mm/dd/yyyy) |
Hours waived per week: F29 |
|
|
Waiver of 24 hr licensed nursing requirement:
Date: F30 (mm/dd/yyyy) |
Hours waived per week: F31 |
|
|
Does the facility currently have an approved Nurse Aide Training and Competency Evaluation Program? F32 |
Yes |
No |
Name of Person Completing Form
Time
Signature
Date
Form |
1 |

DEPARTMENT OF HEALTH AND HUMAN SERVICES
CENTERS FOR MEDICARE & MEDICAID SERVICES |
OMB Exempt |
|
GENERAL INSTRUCTIONS AND DEFINITIONS
(use with
This form is to be completed by the Facility. For the purpose of this form “the facility” equals certified beds (i.e., Medicare and/or Medicaid certified beds).
Standard Survey: LEAVE BLANK – Survey team will complete.
Extended Survey: LEAVE BLANK – Survey team will complete.
INSTRUCTIONS AND DEFINITIONS
Name of Facility: Use the official name of the facility for business and mailing purposes. This includes components or units of a larger institution.
Provider Number: Leave blank on initial certifications. On all recertifications, insert the facility’s assigned six- digit provider code.
Street Address: Street name and number refers to physical location, not mailing address, if two addresses differ.
City: Rural addresses should include the city of the nearest post office.
County: County refers to parish name in Louisiana and township name where appropriate in the New England States.
State: For U.S. possessions and trust territories, name is included in lieu of the State.
Zip Code: Zip Code refers to the
Telephone Number: Include the area code.
State/County Code: LEAVE BLANK. State Survey Office will complete.
State/Region Code: LEAVE BLANK. State Survey Office will complete.
Block F9: Enter either 01 (SNF), 02 (NF), or 03 (SNF/NF).
Block F10: If the facility is under administrative control of a hospital, check “yes,” otherwise check “no.”
Block F11: The hospital provider number is the hospital’s assigned
Block F12: Identify the type of organization that controls and operates the facility. Enter the code as identified for that organization (e.g., for a for profit facility owned by an individual, enter 01 in the F12 block; a facility owned by a city government would be entered as 09 in the F12 block).
Definitions to determine ownership are:
Government: If operated by a governmental entity, indicate whether State, City, Hospital District, County, City/County, or Federal Government.
Block F13: Check “yes” if the facility is owned or leased by a
A
Block F14: If applicable, enter the name of the multi- facility organization. Use the name of the corporate ownership of the
Block F15 – F23: Enter the number of beds in the facility’s Dedicated Special Care Units. These are units with a specific number of beds, identified and dedicated by the facility for residents with specific needs/diagnoses. They need not be certified or recognized by regulatory authorities. For example, a SNF admits a large number of residents with head injuries. They have set aside 8 beds on the north wing, staffed with specifically trained personnel. Show “8” in F19.
Block F24: Check “yes” if the facility currently has an organized residents’ group, i.e., a group(s) that meets regularly to discuss and offer suggestions about facility policies and procedures affecting residents’ care, treatment, and quality of life; to sup- port each other; to plan resident and family activities; to participate
in educational activities or for any other purposes; otherwise check “no.”
Form |
1 |

Block F25: Check “yes” if the facility currently has an organized group of family members of residents, i.e., a group(s) that meets regularly to discuss and offer suggestions about facility policies and procedures affecting residents’ care, treatment, and quality of life; to support each other, to plan resident and family activities; to participate in educational activities or for any other purpose; otherwise check “no.”
Block F26: Check “yes” if the facility conducts experimental research; otherwise check “no.” Experimental research means using residents to develop and test clinical treatments, such as a new drug or therapy, that involves treatment and control groups. For example, a clinical trial of a new drug would be experimental research.
Block F27: Check “yes” if the facility is part of a continuing care retirement community (CCRC); otherwise check “no.” A CCRC is any facility which operates under State regulation as a continuing care retirement community.
Blocks F28 – F31: If the facility has been granted a nurse staffing waiver by CMS or the State Agency in accordance with the provisions at 42CFR 483.35(e) or (f), enter the last approval date of the waiver(s) and report the number of hours being waived for each type of waiver approval.
Block F32: Check “yes” if the facility has a State approved Nurse Aide Training and Competency Evaluation Program; otherwise check “no.”
Form |
2 |
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose | The CMS 671 form is used for long-term care facilities to apply for participation in Medicare and Medicaid programs. |
| Owner Types | Facilities can be operated as for-profit, non-profit, or government-owned organizations. |
| Required Information | Facilities must provide details like provider number, address, contact information, and ownership type on the form. |
| State-Specific Laws | Each state may have unique regulations governing how facilities operate and apply for Medicare and Medicaid, which can affect the use of the CMS 671 form. |
Guidelines on Utilizing Cms 671
Completing the CMS 671 form is a crucial step for long-term care facilities seeking participation in Medicare and Medicaid programs. Following these steps carefully ensures that accurate information is submitted promptly, facilitating the review process by the relevant authorities.
- Begin by filling in the Standard Survey and Extended Survey date fields (From and To) as F1, F2, F3, and F4, but leave them blank; the survey team will complete these later.
- Provide the Name of Facility, which should be the official name used for business and mailing purposes.
- Leave the Provider Number blank if this is the initial certification. For recertifications, enter the assigned six-digit provider code.
- Enter the Street Address reflecting the physical location of the facility.
- Fill in the City field. If the facility is in a rural area, use the city of the nearest post office.
- Provide the County name.
- Select the State where the facility is located. U.S. possessions and trust territories should also be named accordingly.
- Complete the Zip Code including the “Zip-plus-four” code if available.
- Input the Telephone Number with the area code.
- Leave State/County Code and State/Region Code blank; these will be filled out by the State Survey Office.
- Indicate the type of facility by selecting 01 (SNF), 02 (NF), or 03 (SNF/NF) in block F9.
- Answer F10 by checking “Yes” if the facility is hospital-based, and if so, provide the Hospital Provider Number in block F11.
- In block F12, identify the facility's ownership: For-Profit, Non-Profit, or Government. Use the provided codes to indicate the ownership type.
- In block F13, select “Yes” or “No” to indicate if the facility is owned or leased by a multi-facility organization.
- In block F14, enter the name of the multi-facility organization, if applicable.
- For the Dedicated Special Care Units (F15-F23), enter the number of beds for each specified need (such as AIDS, Alzheimer’s, etc.).
- Indicate whether there is an organized residents’ group by answering F24 with “Yes” or “No”.
- Check F25 for the existence of an organized group of family members of residents.
- Respond to F26 by indicating if experimental research is conducted in the facility.
- In block F27, state whether the facility is part of a continuing care retirement community (CCRC).
- For staffing waivers, fill in blocks F28-F31 with the date and hours waived, or write “NA” if no waiver exists.
- In block F32, indicate if the facility currently has an approved Nurse Aide Training and Competency Evaluation Program.
- Finally, provide the Name of Person Completing Form, the Time, and sign it with the Date.
What You Should Know About This Form
What is the purpose of the CMS 671 form?
The CMS 671 form is designed for long-term care facilities to apply for participation in Medicare and Medicaid programs. It collects essential information about the facility, its services, and its operational structure, which helps ensure compliance with federal regulations. The form assists regulatory bodies in evaluating facilities for certification and re-certification based on the care they provide to residents.
Who is responsible for completing the CMS 671 form?
The facility itself is responsible for completing the CMS 671 form. This means that a representative from the facility must provide accurate information regarding its operations, ownership, and care services. It is essential that the person filling out the form understands the facility’s structure and meets the reporting requirements set forth by Medicare and Medicaid.
What specific types of information are required on the form?
The CMS 671 form requires several key pieces of information. This includes the facility’s official name, provider number, location, contact details, and the types of care offered. It also asks about the ownership structure of the facility, the presence of organized resident and family groups, and any special care units dedicated to specific medical needs. Completing these sections accurately is crucial for proper evaluation and potential certification by Medicare or Medicaid.
What are Dedicated Special Care Units, and how should they be reported on the form?
Dedicated Special Care Units refer to specific areas within a facility that cater to residents with particular needs, like Alzheimer’s care or dialysis. When completing the CMS 671 form, facilities must indicate the number of beds allocated for each type of care. This information helps regulatory agencies understand the capacity of the facility to address specialized medical needs, which is important for both assessment and planning purposes.
How does the staffing waiver process work in relation to the CMS 671 form?
The CMS 671 form includes sections for reporting staffing waivers. If a facility has received approval for a nurse staffing waiver, it must provide details such as the type of waiver, the date of last approval, and the number of hours waived each week. This allows the facility to operate under certain adjusted staffing requirements while still adhering to care regulations. If a waiver is not applicable, the facility should indicate "NA" in the appropriate sections.
Common mistakes
Completing the CMS 671 form requires attention to detail. One common mistake is failing to use the official name of the facility. The name must match the business and mailing purposes exactly. Inconsistencies can lead to delays in processing and potential issues with Medicare and Medicaid certification.
Another mistake is neglecting to leave certain fields blank as instructed. Specifically, the Standard Survey and Extended Survey fields should be left blank. It's important to follow these guidelines precisely; doing otherwise complicates matters for both the facility and the survey team.
Incorrectly entering the provider number is also a frequent error. On initial certifications, leave this field blank. However, during recertifications, the facility's six-digit provider code must be included. Failing to do so can result in the form being rejected.
One of the more significant errors involves the ownership classification. Facilities often misunderstand the definitions of For-Profit, Non-Profit, and Government categories. Misclassifying the facility can lead to improper treatment under regulations and possible penalties.
Not providing necessary details about staffing waivers is another oversight. If the facility has a staffing waiver, the individual must specify the number of hours waived and the date of the last approval. Conversely, if there is no waiver, it’s crucial to write "NA" in the provided spaces.
Finally, many people fail to sign and date the form correctly. The individual completing the form must include their name, time, signature, and the date. This oversight may render the entire submission invalid, leading to further complications.
Documents used along the form
The CMS-671 form is an important document for facilities seeking Medicare and Medicaid certification. Alongside this form, other documents may be required to ensure a smooth application process. Below is a list of ten additional forms and documents that are commonly used with the CMS-671. Each of these plays a critical role in providing the necessary information for regulatory approval and care standards.
- CMS-855A: This is the application for Medicare enrollment for institutional providers, including skilled nursing facilities. It gathers detailed information about the provider and the services they offer.
- CMS-2567: This survey and certification report documents findings from the inspections of long-term care facilities. It lists any deficiencies and is crucial for compliance monitoring.
- State Licensure Application: A form required by state health departments that certifies that the facility meets state-specific regulations for operation.
- Annual Financial Report: This report provides a detailed overview of the facility's financial health and sustainability, which is assessed by both Medicare and Medicaid.
- NPI Application (CMS-10114): This application is necessary for obtaining a National Provider Identifier, which is essential for billing and claims processing.
- Staffing Waiver Request: This document is submitted if the facility is requesting a waiver for nurse staffing requirements, outlining the reasons and supporting data.
- Quality Assessment and Performance Improvement Plan: This plan outlines how the facility monitors and improves the quality of care provided to residents and must be submitted for evaluation.
- Background Check Documentation: Proof that criminal background checks have been performed on all staff members, ensuring a safe environment for residents.
- Plan of Correction: After deficiencies are found, a plan detailing how the facility will address the issues and improve care quality is required to demonstrate compliance.
- Clinical Policies and Procedures: Documentation showing framework guidelines on care practices, safety measures, and quality assurance protocols followed by the facility.
These additional forms and documents assist in painting a complete picture of the facility's operations, compliance, and quality of care. Completing these accurately and thoroughly is essential for securing necessary certifications and maintaining high standards in healthcare delivery.
Similar forms
-
CMS-672: This form is similar to the CMS-671 as it also pertains to long-term care facilities. It gathers information needed for Medicare and Medicaid participation and focuses on compliance with specific federal regulations. Like the CMS-671, it requires details about the organization's structure, services offered, and staff qualifications.
-
CMS-855A: The CMS-855A is used for enrolling providers in Medicare. It shares similarities with the CMS-671 by collecting vital information about the organization’s ownership, services, and compliance history. Both forms help ensure that providers meet necessary requirements to participate in Medicare and Medicaid programs.
-
CMS-1500: This form is primarily used for billing Medicare for medical and healthcare services. Although the focus is different, both forms require accurate details about the facility in order to maintain eligibility for federal healthcare programs. The CMS-1500 has information on diagnosis and services, while CMS-671 centers on facility compliance and structure.
-
State Licensure Application: Like the CMS-671, this application is required for long-term care facilities to operate legally within a state. Both documents ensure that facilities adhere to state and federal regulations and collect similar information regarding ownership, services, and compliance.
Dos and Don'ts
When completing the CMS 671 form, attention to detail is crucial. Here are some important dos and don'ts to consider:
- Do use the official name of the facility for all sections requiring identification. This ensures clarity and avoids confusion.
- Do leave the Provider Number and State/County Code sections blank on your initial certification. These will be filled in during the review process.
- Do accurately specify the type of organization controlling the facility in Block F12. This information is essential for proper classification.
- Do answer all questions honestly. For example, indicate whether the facility operates under a multi-facility organization and specify any dedicated special care units.
- Don't skip any blocks that require information. Each section is designed to gather specific data critical for evaluation.
- Don't guess at answers if you're unsure. It's better to check the appropriate "yes" or "no" than to provide potentially misleading information.
Misconceptions
Understanding the CMS 671 form is essential for long-term care facilities applying for Medicare and Medicaid. However, several misconceptions can lead to confusion. Here are six common misconceptions:
- It is only for skilled nursing facilities. Many believe the CMS 671 form applies exclusively to skilled nursing facilities (SNFs). In reality, it is also for nursing facilities eligible for Medicaid, and both kinds of facilities must complete this form.
- The form is optional for facilities seeking certification. Some think they can choose whether or not to submit this form. However, submission of the CMS 671 is mandatory to participate in Medicare and Medicaid programs.
- All sections must be filled out completely. It is a misconception that every field must be completed on the form. Certain blocks are designated to be left blank, as they will be filled in by the survey team.
- The form only gets submitted once. Some may think the CMS 671 is a one-time submission. Facilities must regularly submit this form during recertifications or if there are significant changes in their operations.
- Ownership information is not necessary. There is a belief that providing details about facility ownership is unimportant. The CMS 671 requires specific codes indicating whether a facility is for-profit, non-profit, or government-operated.
- Only the facility administrator can fill out the form. Many assume that only the administrator can complete the CMS 671. In fact, any knowledgeable person can fill it out, as long as they provide accurate information.
Clarifying these misconceptions can help ensure accurate completion of the CMS 671 form. Proper understanding fosters compliance with Medicare and Medicaid requirements.
Key takeaways
The CMS-671 form is crucial for facilities seeking Medicare and Medicaid certification, specifically for long-term care providers. Properly filling out this form ensures compliance with federal standards.
Ensure you accurately list the official name and physical address of the facility. This is essential for business and mailing communications.
Pay close attention to the ownership category in Block F12. Select the correct classification, such as For-Profit, Non-Profit, or Government, as this impacts regulatory oversight and funding.
Blocks related to organized groups (like residents and family members) should reflect accurate information. This data is significant for understanding community engagement and support within the facility.
If applicable, indicate any staffing waivers in Blocks F28 to F31. This needs to show the approval dates and hours waived, which are essential for regulatory compliance.
Browse Other Templates
Example of Plot - Story leaves room for speculation about future possibilities.
Choices Opwdd - The IMS-01 form is the User ID and System Access Request Form for external users of OPWDD.
Patient Intake Form Template - Patient safety considerations, such as the presence of seatbelts, contribute to risk management.