Fill Out Your De 1378N Form
The DE 1378N form serves as a crucial document for employers seeking elective coverage under the California State Disability Insurance (SDI) program. Specifically designed for employing units with eligible employees, governmental entities, and Indian tribes, this application enables them to secure disability insurance for their workforce under specified sections of the California Unemployment Insurance Code (CUIC). Importantly, the DE 1378N does not apply to employers seeking unemployment insurance benefits, thus preventing confusion regarding its purpose. When approved, the elective coverage agreement will detail the obligations that come with this insurance, requiring employers to comply with particular conditions. The application must be filed with necessary supporting documents, such as negotiated agreements or governing body resolutions, and must include information about employees to be covered along with their governing structure. Employers must also be aware of the timeline for coverage commencement, as it cannot retroactively apply but rather begins in line with the calendar quarters outlined in the form. Understanding the requirements and implications of the DE 1378N form is essential for employers wishing to provide this critical coverage to their employees.
De 1378N Example
Taxpayer Assistance Center, Attention: Specialized Coverage Desk, P.O. Box 2068, Rancho Cordova, CA
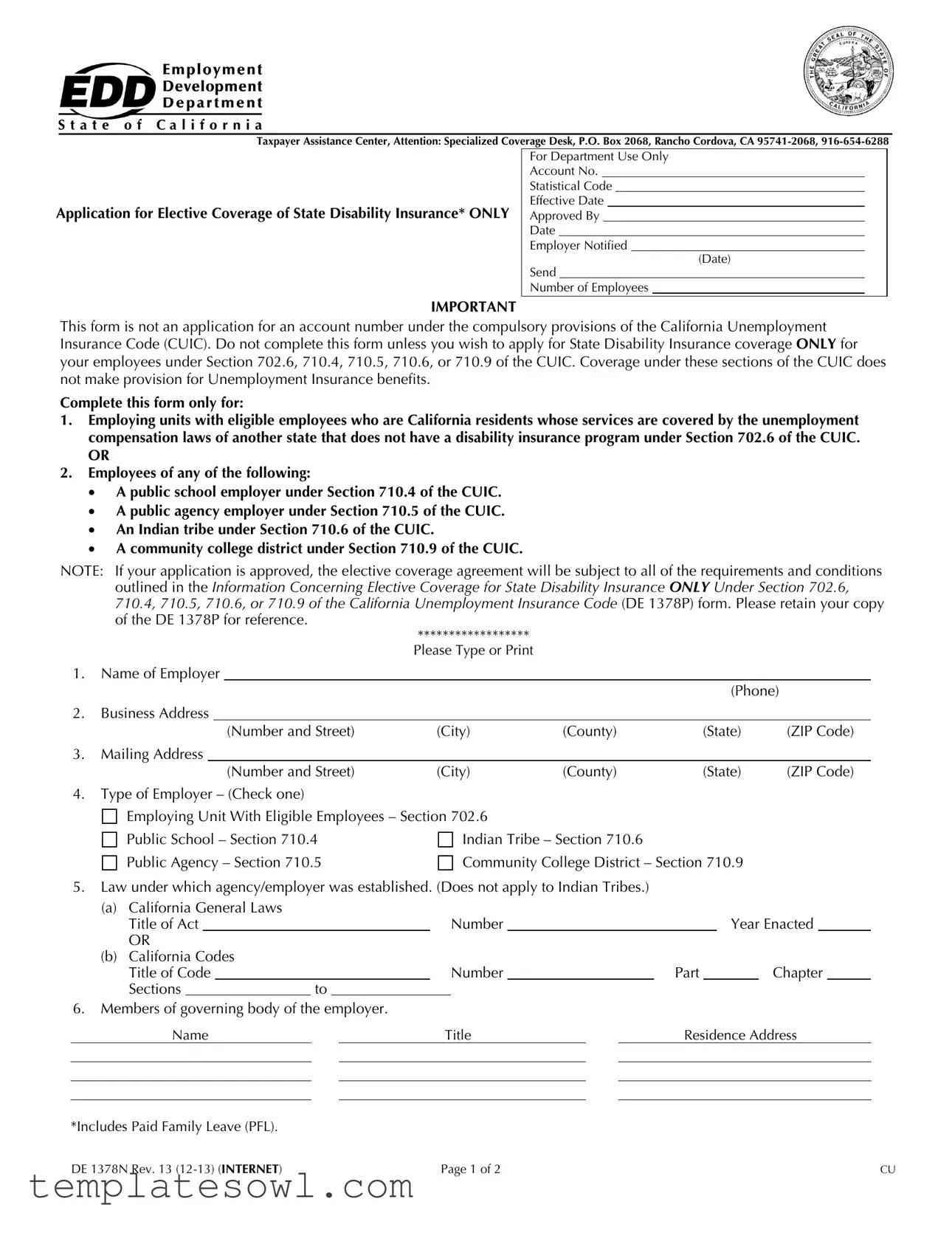
Application for Elective Coverage of State Disability Insurance* ONLY
For Department Use Only
Account No.
Statistical Code
Effective Date
Approved By
Date
Employer Notified
(Date)
Send
Number of Employees
IMPORTANT
This form is not an application for an account number under the compulsory provisions of the California Unemployment Insurance Code (CUIC). Do not complete this form unless you wish to apply for State Disability Insurance coverage ONLY for your employees under Section 702.6, 710.4, 710.5, 710.6, or 710.9 of the CUIC. Coverage under these sections of the CUIC does not make provision for Unemployment Insurance benefits.
Complete this form only for:
1.Employing units with eligible employees who are California residents whose services are covered by the unemployment compensation laws of another state that does not have a disability insurance program under Section 702.6 of the CUIC.
OR
2.Employees of any of the following:
A public school employer under Section 710.4 of the CUIC.
A public agency employer under Section 710.5 of the CUIC.
An Indian tribe under Section 710.6 of the CUIC.
A community college district under Section 710.9 of the CUIC.
NOTE:
1.Name of Employer
|
|
|
|
|
|
(Phone) |
|
2. |
Business Address |
|
|
|
|
||
|
|
|
(Number and Street) |
(City) |
(County) |
(State) |
(ZIP Code) |
3. |
Mailing Address |
|
|
|
|
||
|
|
|
(Number and Street) |
(City) |
(County) |
(State) |
(ZIP Code) |
4.Type of Employer – (Check one)

 Employing Unit With Eligible Employees – Section 702.6
Employing Unit With Eligible Employees – Section 702.6
Public School – Section 710.4
Public Agency – Section 710.5
Indian Tribe – Section 710.6
Community College District – Section 710.9
5.Law under which agency/employer was established. (Does not apply to Indian Tribes.)
(a) |
California General Laws |
|
|
|
|
|
|
|
|
|
|
|
|||
|
Title of Act |
|
|
|
|
Number |
|
|
|
Year Enacted |
|
||||
|
OR |
|
|
|
|
|
|
|
|
|
|
|
|||
(b) |
California Codes |
|
|
|
|
|
|
|
|
|
|
|
|||
|
Title of Code |
|
|
|
|
Number |
|
Part |
|
|
Chapter |
|
|||
|
Sections |
|
to |
|
|
|
|
|
|
|
|
|
|||
6.Members of governing body of the employer.
Name |
|
Title |
|
Residence Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Includes Paid Family Leave (PFL).
DE 1378N Rev. 13 |
Page 1 of 2 |
CU |
7.This application covers employees of the following appropriate units:
Show Name of Bargaining Unit or Describe Type of Services
Bargaining Unit Management Confidential Unrepresented Academic Other
8.Complete this schedule covering all elected officers and appointees who perform services for the agency named in Item 1. Exclude individuals listed in Item 6.
(a)Elected offices: (These individuals are ineligible for coverage.) Title of Position
(b)Person holding appointive positions: (These individuals are eligible for coverage unless appointed to fill a vacant elected office.)
|
No. of Positions |
|
No. of Such Individuals |
|
Title of Position |
in this Category |
By Whom Appointed |
Desiring Coverage |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(c)Total number of employees to be covered (excluding elected officers and those appointed by the Governor).
9.Deductions should not be made from your employees' wages for the purpose of paying employee contributions required under the CUIC until your election is approved.
10.On what date do you wish elective coverage to commence? Keep in mind that the commencement date of an elective coverage agreement shall not be prior to the first day of the calendar quarter in which the application is filed, nor later than the first day of the following calendar quarter.
First day of current quarter |
First day of next quarter |
11.Attach a copy of either:
The negotiated agreement between the employer and the recognized employee organization or written petition signed by a majority of the eligible employees to be covered by the election under Section 702.6 of the CUIC.
OR
The resolution in which the governing body described in Item 6 approved the filing of an application for elective
coverage under Section 710.4, 710.5, 710.6, or 710.9 of the CUIC.
******************
The employing unit with eligible employees or governmental or tribal entity described in Item 1 hereby files its application under Section 702.6, 710.4, 710.5, 710.6, or 710.9 of the CUIC to become an employer subject to the CUIC. It is understood that upon approval of the election by the Director, the Employing Unit/Public School/Public Agency/Indian Tribe/Community College District will be an employer subject to the CUIC for State Disability Insurance purposes ONLY to the same extent as other employers as of the date specified in the approval, and will remain a subject employer for at least two complete calendar years and thereafter, until this election is terminated as provided by the CUIC.
I declare that this application has been examined by me, and to the best of my knowledge, it is true and correct and made in good faith under the provisions of the CUIC.
This declaration must be signed by one |
(Signed) |
|
Date |
or more individuals shown under Item 6. |
(Signed) |
|
Date |
|
(Signed) |
|
Date |
DE 1378N Rev. 13 |
Page 2 of 2 |
CU |
Form Characteristics
| Fact Name | Description |
|---|---|
| Governing Laws | The DE 1378N form is governed by Sections 702.6, 710.4, 710.5, 710.6, and 710.9 of the California Unemployment Insurance Code. |
| Application Purpose | This form is an application for elective coverage of State Disability Insurance for certain employees, not for an account number under compulsory provisions. |
| Eligibility Criteria | Only employing units with eligible California resident employees or specific public agencies, including community colleges and Indian tribes, can apply. |
| Commencement Date | The coverage can only begin on the first day of the calendar quarter in which the application is filed or the first day of the next quarter. |
Guidelines on Utilizing De 1378N
Once the DE 1378N form is filled out correctly, it will be submitted for approval. The approval will allow coverage for your employees under certain sections of the California Unemployment Insurance Code. This process is essential for any employer looking to provide State Disability Insurance coverage. Be prepared to follow the steps below to ensure everything is completed properly.
- Enter the Name of Employer and Phone Number in the designated area at the top of the form.
- Fill in the Business Address including Number and Street, City, County, State, and ZIP Code.
- Provide the Mailing Address if different from the business address, including all relevant details.
- Select the Type of Employer by checking only one of the provided options.
- If applicable, fill in the Law under which your agency/employer was established, including the Title of Act or California Codes.
- List the Members of the governing body of the employer, including their Name, Title, and Residence Address.
- Indicate the name of the appropriate units your application covers in Item 7.
- Complete the schedule for elected officers and appointees, as instructed in Item 8.
- Carefully note in Item 9 that deductions for contributions should not be taken until election approval.
- State the desired commencement date for elective coverage in Item 10, ensuring it aligns with the calendar quarter rules.
- Attach the necessary supporting documents required in Item 11, as outlined.
- At the bottom of the form, ensure that the declaration is signed by one or more individuals listed in Item 6, along with the date.
What You Should Know About This Form
What is the purpose of the DE 1378N form?
The DE 1378N form serves as an application for elective coverage of State Disability Insurance (SDI) for specific types of employers and their eligible employees in California. Employers who wish to provide this coverage must apply through this form if their employees are otherwise covered under unemployment compensation laws of another state that lacks a disability insurance program. The form is exclusively for those who want to ensure SDI coverage is in place for their employees without extending to Unemployment Insurance benefits.
Who can use the DE 1378N form?
The DE 1378N form is intended for various employers, including public school employers, public agency employers, Indian tribes, and community college districts. Specifically, it applies to employing units with eligible employees who are California residents yet fall under the unemployment laws of another state. It’s crucial that employers review the criteria carefully to determine their eligibility before submitting the form.
What should I include with my DE 1378N application?
What happens after my DE 1378N application is submitted?
Once you submit the DE 1378N form, it will undergo review by the appropriate authorities. If approved, your elective coverage agreement will be subject to the conditions specified within the California Unemployment Insurance Code. Importantly, this approval sets your employer status regarding State Disability Insurance, which must be maintained for at least two complete calendar years. You'll also want to keep a copy of the DE 1378P document provided for future reference, as it serves as important information concerning the coverage.
Common mistakes
When completing the DE 1378N form, people often make several common mistakes that can delay the process or even lead to outright denial. One frequent error is not using the correct format when entering employer information. Make sure to type or print clearly, as illegible handwriting can create confusion and cause issues in the processing. Always double-check that everything is filled out legibly.
Another mistake involves the failure to provide all required addresses. Many applicants forget to complete both the business address and mailing address sections. Ensure that you provide a clear description of where you operate and where you want any correspondence sent. Missing any of this information can slow down your application.
Some applicants also neglect to scroll down to complete all parts of the form. It’s crucial to go through the entire document. Each section holds important questions that could affect your coverage. Leaving sections blank or incomplete may lead to unnecessary delays.
Furthermore, errors can occur when checking the type of employer. Picking the wrong category, whether it’s a public school employer or a community college district, can lead to complications. Take a moment to carefully read the options and ensure you choose the one that accurately reflects your situation.
People often miscalculate the effective date for elective coverage. It is important to remember that the start date cannot be before the first day of the quarter in which you filed the application. Be sure to adhere to this guideline, as it is rigorously enforced.
Another commonly overlooked requirement is attaching the necessary documents. Many applicants forget to include copies of the negotiated agreements or resolutions that support the coverage request. Make a checklist to ensure that all necessary attachments are included with your submission.
Finally, not signing the declaration or having the signatures of the appropriate individuals can result in immediate rejection. The declaration section is key and must be filled out correctly. Always verify that all required signatures are present before submitting the form.
Documents used along the form
The DE 1378N form is a critical document for employers wishing to apply for elective coverage for State Disability Insurance in California. Alongside this form, there are several other documents that may also be required for a smooth application process. Understanding these forms can help ensure compliance and ease any potential confusion when applying.
- DE 1378P: This form, known as "Information Concerning Elective Coverage for State Disability Insurance," details the regulations and guidelines related to the elective coverage agreement. It offers valuable insights into the requirements that must be met and should be retained for reference throughout the coverage period.
- Written Petition: A written petition must be signed by a majority of eligible employees seeking elective coverage under Section 702.6 of the California Unemployment Insurance Code. This document demonstrates employee support for the application, making it a crucial component of the process.
- Negotiated Agreement: Employers are required to attach a copy of the negotiated agreement between themselves and the recognized employee organization. This document should outline the terms and conditions surrounding coverage and reflect the consensus of both parties involved.
- Governing Body Resolution: In cases where an employer is applying under Sections 710.4, 710.5, 710.6, or 710.9, a resolution from the governing body must accompany the application. This resolution showcases formal approval for the application and represents the governing body’s consensus regarding elective coverage.
- Employer Information Form: This form collects vital employer details, including names, addresses, and the type of employer. It ensures that the California Employment Development Department has complete and accurate information about the entity applying for coverage.
Gathering and understanding these documents alongside the DE 1378N form can streamline the application process and help ensure that all necessary information is submitted accurately. Proactive preparation will lead to a smoother experience and a higher likelihood of obtaining the desired coverage.
Similar forms
The DE 1378N form serves a specific purpose in applying for elective coverage of State Disability Insurance. Several other documents share similarities with this form, particularly in their functions and requirements. Below is a list of documents that bear resemblance to the DE 1378N form:
- DE 1378P: This form outlines the requirements for elective coverage under the same sections of the California Unemployment Insurance Code. It should be retained for reference once an application is approved.
- DE 2501: This document is designed for employees to apply for State Disability Insurance benefits. Like the DE 1378N, it focuses on coverage and eligibility requirements.
- DE 2500: Similar to the DE 2501, this form allows employees to initiate a claim for disability benefits, ensuring they are aware of the coverage associated with their employment.
- DE 2508: This document serves as an employer's notification to employees about their rights and responsibilities regarding State Disability Insurance. It parallels the DE 1378N in informing employees of coverage details.
- DE 2260: This form provides information about eligibility for State Disability Insurance. It complements the DE 1378N by detailing the applicant's responsibilities once coverage is obtained.
- DE 2502: This form, like the DE 1378N, is related to State Disability Insurance and is used for the approval process concerning coverage for various employee categories.
- DE 2525XX: This document covers the conditions under which employers must notify their employees about State Disability Insurance. It is similar in its intent to ensure clarity about coverage.
- DE 1995: This form is a request for information about a worker's State Disability Insurance claim. It relates to the DE 1378N in that both address aspects of coverage and claims.
- DE 1273: This document is used to report employee contributions to disability insurance. It shares a common objective with the DE 1378N: ensuring compliance with coverage obligations.
Each of these documents plays a role in the larger process of managing State Disability Insurance, emphasizing the significance of understanding coverage and compliance requirements.
Dos and Don'ts
Here are some important things to remember when filling out the DE 1378N form:
- Do: Ensure all information is accurate and truthful.
- Do: Retain a copy of the DE 1378P for your records.
- Do: Complete the form only if you want to apply for State Disability Insurance coverage for your employees.
- Do: Clearly mark the type of employer on the form.
- Do: Attach the necessary documentation, such as the negotiated agreement or resolution.
- Don't: Submit the form without reviewing it for any errors or omissions.
- Don't: Deduct employee contributions from wages until the election is approved.
Following these guidelines will help streamline the process and avoid delays.
Misconceptions
Misconceptions surrounding the DE 1378N form can lead to confusion for employers and employees alike. Understanding the truth can help clarify the purpose and requirements of this important document.
- Misconception 1: The DE 1378N form is an application for an unemployment insurance account.
- Misconception 2: All employers are eligible to apply using this form.
- Misconception 3: Completing the DE 1378N will automatically provide coverage for all employees.
- Misconception 4: There are no limitations on the coverage commencement date.
- Misconception 5: Elected officials are automatically covered under this form.
- Misconception 6: Once elected coverage is obtained, it cannot be terminated.
This form is specifically intended for elective coverage of State Disability Insurance only. It does not serve as an application for unemployment insurance benefits.
Only certain employers, such as public schools, public agencies, Indian tribes, and community college districts, can use the DE 1378N to apply for elective coverage. Specific eligibility requirements must be met based on employee residency and coverage laws.
The application must be approved for coverage to take effect. Deductions from employee wages cannot begin until this approval is granted.
The coverage start date must align with specific timing rules. It cannot begin before the quarterly application date or later than the next quarter’s first day.
Elected officials are generally not eligible for coverage through the DE 1378N application. However, certain appointed individuals may be covered unless they fill vacant elected positions.
Elective coverage can eventually be terminated as outlined by the California Unemployment Insurance Code. Employers should be aware of these provisions for ongoing compliance.
Key takeaways
When filling out and utilizing the DE 1378N form, keep in mind several critical points to ensure a smooth process.
- Applicability of the Form: This form is specifically for requesting elective coverage for State Disability Insurance. It's essential to understand that it is not an application for an account number under the California Unemployment Insurance Code.
- Eligibility Criteria: Complete this form only if you have eligible employees who are California residents and covered by the unemployment laws of another state without disability insurance.
- Documentation Requirement: Attach necessary documentation, such as a negotiated agreement or governing body resolution, to support your application for elective coverage.
- Commencement Date: Indicate the desired start date for coverage, ensuring it aligns with the first day of the calendar quarter in which you file the application.
- Retention of Documents: Keep a copy of the DE 1378P form for future reference, as it contains vital information regarding the conditions of your elective coverage once approved.
Understanding these key points will facilitate a more straightforward application process and comply with the regulations in place regarding State Disability Insurance.
Browse Other Templates
Register Car in Wisconsin - Failure to include all requisite fees may result in processing delays or rejection of the application.
After Marriage Checklist - It is critical that all sections of the form are accurately filled out.