Fill Out Your Ds 326 Form
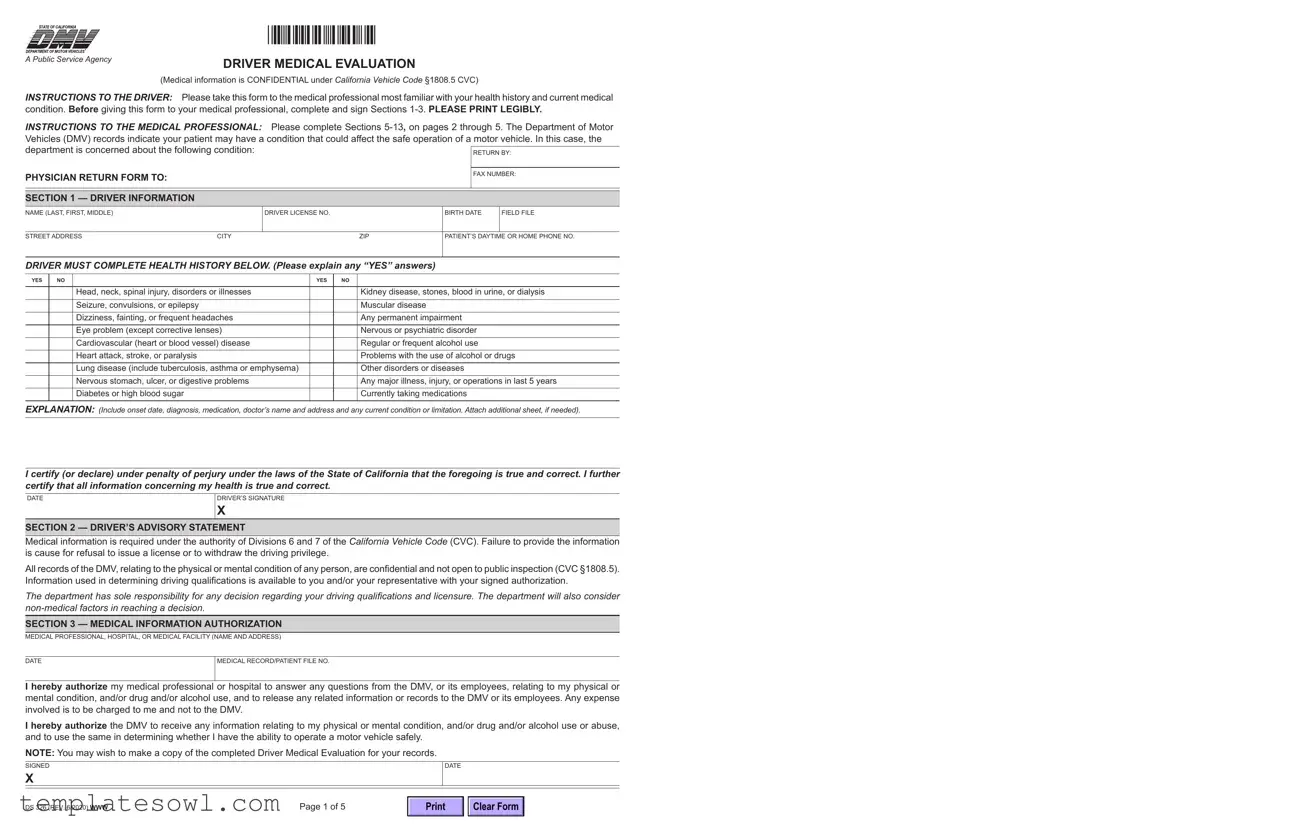
The DS 326 form, known as the Driver Medical Evaluation, serves a crucial function for drivers in California who may have medical conditions affecting their ability to operate a vehicle safely. This form is designed to collect necessary medical information from both the driver and their healthcare provider. The process begins with the driver completing sections that detail their personal information and health history, specifically noting any relevant medical conditions or injuries. Following this, the driver must visit a qualified medical professional who will evaluate their health status in relation to driving safety. This comprehensive evaluation includes assessments of vision, cognitive functioning, and any treatments the driver may be undergoing. Importantly, the form aims to uphold the safety of all road users while ensuring that sensitive medical data remains confidential, adhering to California Vehicle Code §1808.5. Ultimately, the Department of Motor Vehicles (DMV) utilizes this information not only to manage licensing decisions but also to protect the well-being of the driver and the community at large.
Ds 326 Example
|
*DS326* |
A Public Service Agency |
DRIVER MEDICAL EVALUATION |
|
|
|
(Medical information is CONFIDENTIAL under California Vehicle Code §1808.5 CVC) |
INSTRUCTIONS TO THE DRIVER: Please take this form to the medical professional most familiar with your health history and current medical condition. Before giving this form to your medical professional, complete and sign Sections
INSTRUCTIONS TO THE MEDICAL PROFESSIONAL: Please complete Sections
Vehicles (DMV) records indicate your patient may have a condition that could affect the safe operation of a motor vehicle. In this case, the
department is concerned about the following condition: |
|
|
|
||
|
|
RETURN BY: |
|||
|
|
|
|
|
|
PHYSICIAN RETURN FORM TO: |
|
|
|
FAX NUMBER: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION 1 — DRIVER INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
NAME (LAST, FIRST, MIDDLE) |
|
DRIVER LICENSE NO. |
BIRTH DATE |
FIELD FILE |
|
|
|
|
|
|
|
STREET ADDRESS |
CITY |
ZIP |
PATIENT’S DAYTIME OR HOME PHONE NO. |
||
|
|
|
|
|
|
DRIVER MUST COMPLETE HEALTH HISTORY BELOW. (Please explain any “YES” answers)
YES |
NO |
|
YES |
NO |
|
|
|
|
|
|
|
|
|
Head, neck, spinal injury, disorders or illnesses |
|
|
Kidney disease, stones, blood in urine, or dialysis |
|
|
Seizure, convulsions, or epilepsy |
|
|
Muscular disease |
|
|
Dizziness, fainting, or frequent headaches |
|
|
Any permanent impairment |
|
|
Eye problem (except corrective lenses) |
|
|
Nervous or psychiatric disorder |
|
|
Cardiovascular (heart or blood vessel) disease |
|
|
Regular or frequent alcohol use |
|
|
Heart attack, stroke, or paralysis |
|
|
Problems with the use of alcohol or drugs |
|
|
Lung disease (include tuberculosis, asthma or emphysema) |
|
|
Other disorders or diseases |
|
|
Nervous stomach, ulcer, or digestive problems |
|
|
Any major illness, injury, or operations in last 5 years |
|
|
Diabetes or high blood sugar |
|
|
Currently taking medications |
EXPLANATION: (Include onset date, diagnosis, medication, doctor’s name and address and any current condition or limitation. Attach additional sheet, if needed).
I certify (or declare) under penalty of perjury under the laws of the State of California that the foregoing is true and correct. I further certify that all information concerning my health is true and correct.
DATE
DRIVER’S SIGNATURE
X
SECTION 2 — DRIVER’S ADVISORY STATEMENT
Medical information is required under the authority of Divisions 6 and 7 of the California Vehicle Code (CVC). Failure to provide the information is cause for refusal to issue a license or to withdraw the driving privilege.
All records of the DMV, relating to the physical or mental condition of any person, are confidential and not open to public inspection (CVC §1808.5). Information used in determining driving qualifications is available to you and/or your representative with your signed authorization.
The department has sole responsibility for any decision regarding your driving qualifications and licensure. The department will also consider
SECTION 3 — MEDICAL INFORMATION AUTHORIZATION
MEDICAL PROFESSIONAL, HOSPITAL, OR MEDICAL FACILITY (NAME AND ADDRESS)
DATE |
MEDICAL RECORD/PATIENT FILE NO. |
I hereby authorize my medical professional or hospital to answer any questions from the DMV, or its employees, relating to my physical or mental condition, and/or drug and/or alcohol use, and to release any related information or records to the DMV or its employees. Any expense involved is to be charged to me and not to the DMV.
I hereby authorize the DMV to receive any information relating to my physical or mental condition, and/or drug and/or alcohol use or abuse, and to use the same in determining whether I have the ability to operate a motor vehicle safely.
NOTE: You may wish to make a copy of the completed Driver Medical Evaluation for your records.
SIGNED
X
DATE
DS 326 (REV. 6/2020) WWW |
Page 1 of 5 |
Clear Form
SECTIONS 5
SECTION 4 — MEDICAL PROFESSIONAL’S MEDICAL EVALUATION INSTRUCTIONS
INSTRUCTIONS TO THE MEDICAL PROFESSIONAL (MP): The DMV records indicate your patient may have a condition that could affect the safe operation of a motor vehicle. (See Instructions to the Medical Professional, page 1 for the specific medical condition that is a concern to the department.) With your assistance, the department hopes to resolve the matter with a minimum of inconvenience to all concerned.
The Health History and Medical Information Authorization sections on page 1 must be completed and signed by the patient before you complete this Driver Medical Evaluation form.
Your experience and knowledge of the patient’s condition, results of medical examinations and treatment plans, will be of great value in assisting the department to determine a proper licensing decision. PLEASE ANSWER ALL QUESTIONS on this form. If questions do not apply, indicate “N/A”. You may furnish a narrative report if you prefer, but please include all information pertinent to your patient. The department has sole responsibility for any decision regarding the patient’s driving qualifications and licensure. The department will also consider
SECTION 5 — VISION
|
VISUAL ACUITY (without bioptic telescope) |
BOTH EYES |
RIGHT EYE |
|
LEFT EYE |
|
Without Lenses |
20/ |
20/ |
|
20/ |
|
With Present Lenses |
20/ |
20/ |
|
20/ |
|
ANY EYE INJURY OR DISEASE? (LIST) |
|
IS FURTHER EYE EXAMINATION SUGGESTED? |
||
|
|
|
Yes |
No |
|
|
|
|
|
|
|
SECTION 6 — TREATMENT BY OTHER MEDICAL PROFESSIONAL(S)
IS THIS PATIENT BEING TREATED FOR ANY CONDITION BY ANOTHER MP?

 Yes
Yes  No
No
IF YES, PLEASE INDICATE NAME OF TREATING MP(S)
CONDITION BEING TREATED
SECTION 7 — TREATMENT UNDER YOUR SUPERVISION
DIAGNOSIS (IF THE DIAGNOSIS IS A DISORDER CHARACTERIZED BY LAPSES OF CONSCIOUSNESS, DEMENTIA, OR DIABETES, COMPLETE PAGE 3,4 OR 5.)
DO YOU NEED TO SEE YOUR PATIENT AT REGULAR INTERVALS? IF YES, HOW OFTEN?
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PROGNOSIS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
IS THE CONDITION |
|
|
|
(IF MULTIPLE CONDITIONS, PLEASE DESCRIBE STATUS AND PROGNOSIS IN |
|||||
Improving |
Stable |
Worsening or deteriorating |
Subject to change |
||||||
COMMENTS BELOW.) |
|
||||||||
MANIFESTATIONS (SYMPTOMS): |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
(PRESENT) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
(PAST) |
|
|
|
|
|
|
MAY CONDITION IMPAIR VISION? |
||
|
|
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|||||
HOW LONG HAS THIS PERSON BEEN YOUR PATIENT? |
|
DATE OF LAST EXAMINATION |
|
|
|||||
|
|
|
|||||||
IS YOUR PATIENT UNDER A CONTROLLED MEDICAL PROGRAM? |
|
HOW LONG HAS CONTROL BEEN MAINTAINED? |
|||||||
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|||||||
IS THE PATIENT ADHERING TO THE MEDICAL REGIMEN? |
|
IS THE PATIENT KNOWLEDGEABLE ABOUT THE MEDICAL CONDITION? |
|||||||
Yes |
No |
If no, please explain: |
|
Yes |
No |
|
|||
|
|
|
|
|
|||||
LIST THE MEDICATIONS PRESCRIBED. PLEASE INCLUDE DOSAGE AND FREQUENCY OF USE |
|
|
|
|
|||||
|
|
|
|
|
|
||||
|
|
|
|
|
|
||||
WHEN WAS THE LAST MEDICATION CHANGE MADE? |
|
|
|
|
|
||||
|
|
|
|
|
|||||
WOULD THE SIDE EFFECTS FROM THE PRESCRIBED MEDICATIONS INTERFERE WITH YOUR PATIENT’S ABILITY TO DRIVE SAFELY? |
|
|
|
||||||
Yes |
No |
If yes, please describe: |
|
|
|
|
|
||
|
|
|
|
|
|
||||
DOES YOUR PATIENT’S MEDICAL CONDITION CURRENTLY AFFECT SAFE DRIVING? |
|
|
|
|
|
||||
Yes |
No |
If yes, please explain: |
|
|
|
|
|
||
|
|
|
|||||||
DO YOU CURRENTLY ADVISE AGAINST DRIVING? |
|
WOULD YOU RECOMMEND A DRIVING TEST BE GIVEN BY DMV? |
|||||||
Yes |
No |
|
|
|
Yes |
No |
|
||
|
|
|
|
|
|
|
|
|
|
MP COMMENTS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 2 of 5 |
DS 326 (REV. 6/2020) WWW |
SECTION 8 — LEVELS OF FUNCTIONAL IMPAIRMENTS
Functional impairments that may affect safe driving ability. Please check where applicable.
MILD MODERATE SEVERE
Visual neglect |
......................................... |
Left side |
Right side |
Loss of upper extremity motor control ....
Left side |
Right side |
Loss of lower extremity motor control.....
Left side |
Right side |
WOULD ADAPTIVE DEVICES AID YOUR PATIENT IN COMPENSATING FOR THEIR DISABILITY AS IT PERTAINS TO SAFE DRIVING?

 Yes
Yes  No
No

 Uncertain
Uncertain
IF YES, PLEASE DESCRIBE
SECTION 9 — DEMENTIA OR COGNITIVE IMPAIRMENTS
Alzheimer’s Disease
Other Dementia (Please describe the type of dementia below, e.g.,
HISTORY OF DISEASE, RESULTS OF TESTING, ETC.
Using the definitions given below, please rate the severity of the following forms of cognitive impairments in this patient.
Mild: |
Judgment is relatively intact but work or social activities are significantly impaired. Ability to safely operate a motor vehicle may |
|
or may not be impaired. |
Moderate: Independent living is hazardous and some degree of supervision is necessary. The individual is unable to cope with the environment and driving would be dangerous.
Severe: |
Activities of daily living are so impaired that continual supervision is required. This person is incapable of driving a motor vehicle. |
|
|
NONE |
MILD MODERATE SEVERE UNCERTAIN |
Memory Loss ...................................
Depression, secondary to dementia
Diminished Judgment ......................
Impaired Attention............................
Impaired Language Skills ................
Impaired Visual Spatial Skills ..........
Impulsive Behavior ..........................
Problem Solving Deficits..................
Loss of Awareness of Disability .......
OVERALL DEGREE OF IMPAIRMENT
DS 326 (REV. 6/2020) WWW |
Page 3 of 5 |
SECTION 10 — LAPSE OF CONSCIOUSNESS DISORDER
PLEASE IDENTIFY THE LAPSE OF CONSCIOUSNESS DISORDER BEING REPORTED (Type of seizure, nocturnal, isolated,syncope, blackouts, |
DATE(S) OF EPISODE(S) IN THE PAST THREE YEARS |
|
etc.) |
|
|
|
|
|
DATE OF ONSET, IF KNOWN |
DATE AND TIME OF LAST EPISODE |
|
Please indicate the impairments identified below that are presently shown by your patient.
YES |
NO |
UNCERTAIN |
Sporadic loss of conscious awareness.......................................................................................
Loss of consciousness ...............................................................................................................
Impaired motor function..............................................................................................................
EFFECTS AFTER EPISODE
Confusion ...................................................................................................................................
Diminished concentration ...........................................................................................................
Diminished judgment ..................................................................................................................
Memory loss ...............................................................................................................................
If medication is taken to control seizures, are the serum levels recorded?................................
Are the serum levels medically acceptable? ..............................................................................
COMMENT
SECTION 11 — DIABETES
PLEASE INDICATE THE TYPE OF DIABETES THIS PATIENT HAS |
|
DATE OF DIAGNOSIS |
|
|
||
Type I |
Type 2 |
Gestational |
|
|
|
|
|
|
|
|
|
||
WHAT METHOD OF TREATMENT IS REQUIRED? |
|
|
|
|
||
Controlled diet |
Oral diabetes medication |
Insulin injections |
Insulin pump |
Other: |
||
HAS THIS PATIENT RECEIVED DIABETES EDUCATION FROM A HEALTH CARE TEAM?

 Yes
Yes  No
No
DOES THIS PATIENT COMPLY WITH THE PRESCRIBED TREATMENT PLAN?

 Yes
Yes  No
No
IF NO, PLEASE EXPLAIN
IS THE DIABETES MANAGED AT THIS TIME? |
|
|
|
Yes |
No |
|
|
|
|
||
IF YES, HOW LONG HAS DIABETES BEEN MANAGED OR MAINTAINED? |
IF NO, PLEASE EXPLAIN |
||
|
|
||
WHAT ARE THIS PATIENT’S FASTING BLOOD GLUCOSE LEVELS? |
AFTER HOW MANY HOURS OF FASTING? |
||
|
|
||
WITHIN THE LAST THREE YEARS, HAS THIS PATIENT EXPERIENCED |
REASON FOR EPISODES (e.g., |
||
Hypoglycemic episodes? |
Hyperglycemic episodes? |
|
|
|
|
|
|
Please indicate the complications manifested by the hypoglycemic or hyperglycemic episodes and rate the severity of each.
NONE |
MILD |
MODERATE SEVERE UNCERTAIN |
Abdominal pain................................
Cognitive deficits .............................
Confusion ........................................
Disorientation...................................
Incoordination..................................
Hypoglycemic unawareness............
Lack of stamina ...............................
Loss of consciousness ....................
Stupor ..............................................
Visual changes ................................
Ketoacidosis ....................................
Slowed reactions .............................
Seizures...........................................
Weakness or fatigue........................
Other................................................
Page 4 of 5 |
DS 326 (REV. 6/2020) WWW |
DOES THIS PATIENT MANAGE HYPOGLYCEMIC OR HYPERGLYCEMIC EPISODES? |
|
|||
Yes |
No |
If no, please explain: |
|
|
|
|
|||
HAS THIS PATIENT’S DIABETES CAUSED ANY OF THE FOLLOWING CHRONIC COMPLICATIONS? |
|
|||
Visual changes |
Kidney disease |
Nervous system disease |
Vascular disease |
|
PLEASE DESCRIBE THE EXTENT OF THE COMPLICATIONS
HAS THE PATIENT BEEN HOSPITALIZED WITHIN THE LAST THREE YEARS DUE TO DIABETES COMPLICATIONS? |
WHAT COMPLICATIONS NECESSITATED |
|
Yes |
No If yes, please give dates: |
HOSPITALIZATION? |
HAS AMPUTATION BEEN NECESSARY?

 Yes
Yes  No
No
IF YES, PLEASE EXPLAIN
SECTION 12 — ADDITIONAL COMMENTS BY MEDICAL PROFESSIONAL CONCERNING ANY CONDITION AFFECTING SAFE DRIVING
SECTION 13 — MEDICAL PROFESSIONAL’S SIGNATURE
MP’S SIGNATURE |
MP’S NAME (PRINTED) |
DATE |
|
X |
|
|
|
CLASSIFICATION OR SPECIALTY |
MEDICAL LICENSE NUMBER |
TELEPHONE NUMBER |
|
|
|
( |
) |
|
|
|
|
DS 326 (REV. 6/2020) WWW |
Page 5 of 5 |
Clear Form
Form Characteristics
| Fact Name | Description |
|---|---|
| Document Purpose | The DS 326 form is used for Driver Medical Evaluation in California. |
| Governing Law | This form is governed by the California Vehicle Code, specifically sections 1808.5 and Divisions 6 & 7. |
| Medical Confidentiality | All medical information provided is confidential, as mandated by California law. |
| Submission Requirements | The driver must complete and sign Sections 1-3 before the medical professional fills out the rest. |
| Return Instructions | The completed form must be returned by fax to the Department of Motor Vehicles. |
| Health History Disclosure | Drivers must disclose any medical history that may affect their ability to operate a vehicle safely. |
| Vision Evaluation | Sections 5-13 include vision assessments, with specific instructions for eye health evaluation. |
| Medical Professional's Role | Medical professionals are to assess and report on the driver's medical fitness for safe driving. |
| Possible Outcomes | The DMV uses the evaluation to determine whether to issue or withdraw driving privileges. |
| Patient Record Maintenance | Patients are advised to keep a copy of the completed DS 326 for their records. |
Guidelines on Utilizing Ds 326
When preparing to submit the DS 326 form, it’s important to ensure that all sections are accurately completed. This document plays a key role in evaluating whether the driver meets the medical standards to operate a vehicle safely. Here’s how to fill it out to guarantee proper submission.
- Gather Personal Information: Before starting, find your driver’s license number, birth date, street address, and contact information.
- Complete Sections 1-3: In these sections, fill out your personal details. Make sure to answer all health-related questions truthfully, indicating ‘YES’ or ‘NO.’ If you answer ‘YES’ to any questions, provide detailed explanations in the space provided. Sign and date this section.
- Bring to Medical Professional: Take the completed form to your medical professional who knows your health history. Ensure they are familiar with the DMV’s requirements for assessing your medical condition.
- Medical Evaluation Sections (5-13): Allow your medical professional to complete the remaining sections. They will detail your vision, treatment history, and any conditions affecting your driving ability.
- Sign Authorization: Ensure that your medical professional signs Section 13, confirming they have assessed you and agree with the information provided.
- Review the Entire Form: Check that all sections are filled out completely and accurately. Look for any missing signatures or information.
- Submit the Form: Return the form to the DMV or fax it as instructed. Ensure that you keep a copy for your records.
What You Should Know About This Form
What is the DS 326 form used for?
The DS 326 form, also known as the Driver Medical Evaluation form, is intended for individuals who may have a health condition that could impact their ability to drive safely. The California Department of Motor Vehicles (DMV) uses this form to gather medical information to assess a driver's fitness for operation of a motor vehicle. Completion of this form is often necessary when the DMV has identified a concern related to the driver's medical history or current health status.
Who needs to fill out the DS 326 form?
The driver must complete Sections 1-3 of the DS 326 form before it is taken to a medical professional. The medical professional, who is most familiar with the driver’s health history, then completes Sections 5-13. It is essential that both the driver and the medical professional provide accurate and thorough information, as this will be used to determine whether the individual can safely operate a vehicle.
Are the medical details provided on the DS 326 form confidential?
Yes, medical information submitted through the DS 326 form is kept confidential under California law. Specifically, this falls under California Vehicle Code §1808.5, which ensures that details related to the physical or mental condition of any person are not open to public inspection. Only authorized personnel at the DMV will have access to this information for the purpose of evaluating driving qualifications.
What should I do if I have concerns about completing the form?
If you have any concerns about filling out the DS 326 form, it is important to discuss them with both your medical professional and the DMV. Your doctor can clarify what information needs to be provided based on your health condition. Additionally, the DMV provides contact information, and their representatives can answer questions regarding the process and help alleviate any worries you may have.
What happens once the DS 326 form is submitted?
After the DS 326 form is completed and submitted to the DMV, it will be reviewed. The DMV will consider both the medical information provided and non-medical factors when making a decision about the driver's ability to safely operate a vehicle. Depending on the review, the driver may be authorized to continue driving, or additional evaluations, such as a driving test, may be required. It is crucial that the information provided is accurate, as it can directly influence the outcome of the evaluation.
Common mistakes
Filling out the DS 326 Driver Medical Evaluation form can be a straightforward process, but many people make common mistakes that can lead to delays or complications. One frequent error is failing to provide complete and legible information. The form specifically instructs individuals to print legibly. Illegible handwriting can cause misunderstandings regarding critical health information, which may affect driving eligibility.
Another common mistake involves not addressing all "YES" responses in the health history section. If a driver indicates "YES" to any health conditions, it is essential to include thorough explanations. This section serves to clarify any potential risks that may arise from medical conditions when operating a vehicle. Omitting this information can lead to unnecessary follow-up inquiries from the DMV.
Additionally, leaving sections incomplete can cause significant issues. The form has several parts that require specific details about medical conditions, current treatment, and medications. Incomplete sections can be interpreted as a failure to disclose pertinent medical history, which could result in the denial of a driver's license or permit.
Some individuals may neglect to sign the form. Signatures are crucial as they verify that the information provided is accurate and true to the best of the driver's knowledge. Not signing the form can render it invalid, resulting in further complications in the evaluation process.
Providing outdated contact information is another mistake that can occur. The driver must update their address, phone number, and any contact details to ensure that communication with the DMV proceeds smoothly. Incorrect information may lead to missed notifications or requests for further medical information.
Lastly, failing to include necessary supporting documents can hinder the evaluation process. The DMV may request medical records or additional assessments based on the information provided. Including all relevant documents and reports can streamline the process and enhance the chances of a favorable outcome.
Documents used along the form
The DS 326 form serves an essential purpose by gathering medical evaluations relevant to a driver's ability to operate a vehicle safely. When filling out this form, it is often necessary to accompany it with other documents and forms that further establish the driver’s medical history, condition, or related legal matters. Below is a list of commonly used forms and documents that might be required in conjunction with the DS 326.
- Medical History Form: This form provides a comprehensive overview of the individual’s medical background and conditions. It is essential for healthcare providers to ascertain any prior health issues that may influence driving capabilities.
- Driver’s License Application: In cases where the driver is applying for or renewing a license, this application is critical. It collects personal information, including identification and residency details, along with the medical evaluation that the DS 326 provides.
- Vision Test Report: A document confirming the driver’s visual acuity and overall eye health is often needed. Eye problems can directly affect driving safety, making this report a key supplement to the DS 326.
- Medical Authorization Release Form: This document allows the medical professional to share the driver's medical information with the Department of Motor Vehicles (DMV). It ensures that relevant information is disclosed while maintaining patient confidentiality.
- Physician's Narrative Report: In addition to the DS 326, a physician may provide a detailed narrative explaining the driver's condition and its impact on driving abilities. This report can offer insights that the standard form may not fully capture.
- Follow-Up Appointment Documentation: If further evaluations or treatments are necessary, this documentation can show compliance with medical recommendations. It may also include notes on the driver's attendance and any follow-up tests that have been performed.
- DMV Decision Letter: If the DMV makes a decision regarding the driver’s medical fitness based on the DS 326, this letter outlines the outcome. It is crucial for understanding the implications of the medical evaluation and any further actions required.
In summary, the DS 326 form works hand-in-hand with various other documents to ensure that all aspects of a driver’s medical fitness are thoroughly examined. Having the right forms on hand can streamline the process and help clarify any medical concerns that may arise during evaluations. Each document plays a vital role in protecting both the driver and the safety of others on the road.
Similar forms
The DS 326 form is important for assessing a driver's medical fitness. Several other forms share similar purposes and processes in evaluating a person’s ability to operate a vehicle safely. Here are eight documents that are notably similar to the DS 326 form:
- Form DMV 89: This is used for a medical evaluation when someone's driving privileges are questioned due to health concerns. Like the DS 326, it requires both the driver and a medical professional's input to assess safety.
- Form DL 44: This application for a driver’s license includes a health questionnaire. It asks similar health-related questions to assess any possible impairments that could affect driving safety.
- Form DMV 396: This is a medical report form that assesses the ability of a person to drive safely due to a history of medical conditions, resembling the focus on health in the DS 326.
- Form MV-62: This is required when someone applying for a disability driver license or permit. It collects medical details to ensure the applicant meets health standards for safe driving.
- Form DMV 706: Known as the "Medical Examination Report," it is a comprehensive review that examines health conditions affecting a driver's ability to operate a vehicle safely, similar to the medical evaluation sections of the DS 326.
- Form PS-22: This form is for reporting physical impairments and conditions affecting a driver's ability. Like the DS 326, it necessitates both a driver’s disclosures and medical professional verification.
- Form MC-991: Intended for motorcycle operators, this medical evaluation form closely resembles the DS 326 in that it evaluates the specific medical fitness required for safe motorcycle operation.
- Form DMV 30: This form serves to update physical conditions affecting driving capability, similar to the ongoing evaluations outlined in the DS 326, which monitors health changes over time.
Each of these documents is designed to ensure the safety of drivers and the public while addressing individual health considerations. Proper completion of these forms plays a crucial role in determining a driver's fitness to operate a motor vehicle.
Dos and Don'ts
When filling out the DS 326 form, it is crucial to follow certain guidelines to ensure accuracy and compliance. Below is a list of essential dos and don'ts to help streamline the process.
- Do make sure to print legibly in all sections of the form.
- Do complete and sign Sections 1-3 before presenting the form to the medical professional.
- Do provide detailed explanations for any 'YES' answers in the health history section.
- Do discuss any medications you are currently taking with your medical professional.
- Do keep a copy of the completed form for your records.
- Don't leave any sections blank; indicate 'N/A' if a question does not apply.
- Don't rush through the form; take your time to ensure all information is accurate.
- Don't forget to provide your medical professional with any additional documentation that may be relevant.
- Don't hesitate to ask for clarification on any questions you do not understand.
- Don't forget to consider non-medical factors that may affect your driving qualifications.
Misconceptions
Misconceptions about the DS 326 form can lead to confusion and potentially impact drivers who are required to submit this medical evaluation. Here are ten common misunderstandings along with clarifications:
- The DS 326 form is required for all drivers. Not all drivers need to fill out this form. It is specifically for individuals who have medical conditions that may affect their ability to drive safely.
- Filling out the form guarantees that I will keep my driver's license. Completing the DS 326 does not ensure that you will retain your driving privileges. The final decision rests with the DMV, which considers various factors.
- Medical information shared is not confidential. All medical information provided on the form is confidential and protected under California law. The DMV cannot disclose this information publicly.
- I can fill out the entire form by myself. Sections 1-3 must be completed by the driver, but Sections 5-13 require input from a qualified medical professional based on their evaluation.
- My doctor can fill out the form without my consent. The doctor requires your authorization to disclose any medical information to the DMV. It is crucial to sign the Medical Information Authorization.
- I can skip questions that don’t apply to me. It’s essential to answer every question, marking “N/A” for those that do not apply, to avoid any processing delays.
- Once submitted, the DMV will make a decision immediately. The DMV review process can take time. It is important not to expect an immediate result after submission.
- All medical conditions are treated equally. The DMV assesses the severity of conditions differently. Some might require further tests or evaluations based on their potential impact on driving.
- The form only concerns physical health. The evaluation includes mental health, cognitive abilities, and certain medication side effects, which can all affect driving safety.
- There’s no need to keep a copy of the form. It’s a good idea to keep a copy for your records. Having documentation can be helpful if there are questions or disputes later.
Key takeaways
The DS-326 form is utilized for evaluating the medical conditions of drivers, ensuring they are capable of safely operating a vehicle. It is crucial for drivers to complete sections 1-3 before presenting it to a medical professional.
Medical information provided is confidential under California law, meaning that it cannot be publicly accessed. Only specific parties like the DMV can review this information when necessary to assess driving qualifications.
Drivers must provide detailed medical history, including any pre-existing conditions, medications, and recent treatments. This information aids the medical professional in making a thorough assessment.
Returning the completed form to the DMV is vital. This can be done by the medical professional via fax, ensuring timely processing of the driver's medical evaluation.
Medicals professionals must accurately fill out sections 5-13 of the form. They should use their knowledge to report on the driver’s ability to operate a vehicle safely, taking into account both medical and non-medical factors.
Browse Other Templates
Duplicate Vehicle Registration Request,Replacement Registration Card Application,Lost Plate Replacement Form,Vehicle Registration Update Request,Registration Plate Replacement Application,Weight Class Sticker Replacement Form,Illegible Plate Authoriz - Make sure to fill in all sections that apply to your situation.
Shipping Container Count Sheet,Container Inventory Form,Material Shipment Tally,Logistics Container Tracking Document,Supply Chain Inventory Report,Requisition and Shipment Summary,Shipping Materials Inventory Sheet,Container Shipment Record,Federal - The DD Form 1149 is important for planning and executing shipments.