Fill Out Your E Khc 3 Form
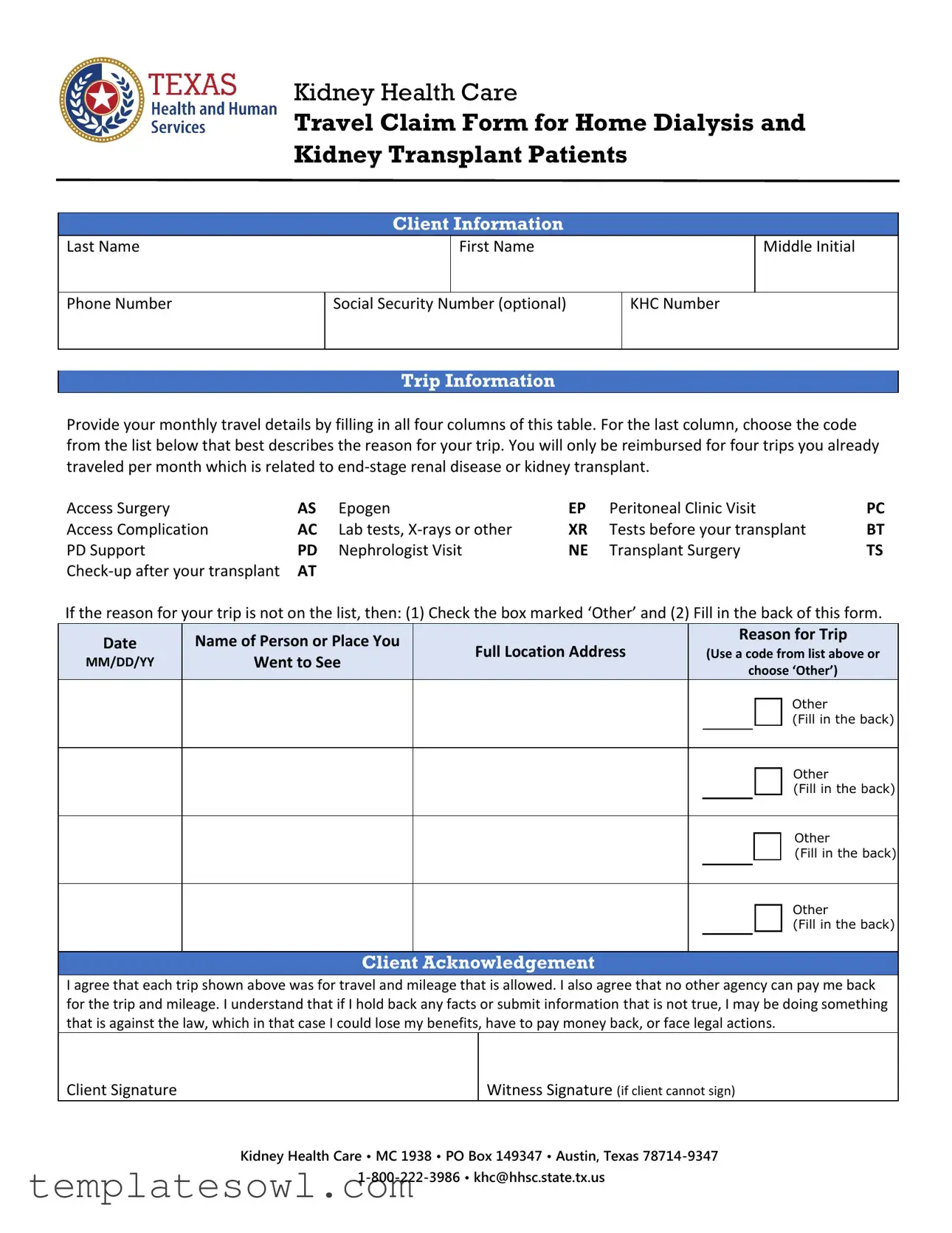
The E Khc 3 form serves as a crucial tool for individuals undergoing home dialysis or kidney transplant procedures to claim travel expenses related to their medical care. This form is specifically designed for patients who have end-stage renal disease and need reimbursement for trips related to their condition. Applicants must provide detailed personal information, including their name, contact number, and KHC number, as well as comprehensive travel details for up to four trips per month. Each trip must correspond to specific medical codes related to the reason for travel, such as Access Surgery or Nephrologist Visit. If a reason is not listed, applicants are prompted to check the ‘Other’ box and provide additional information on the back of the form. After completing the travel information, the client must acknowledge their agreement regarding the accuracy of the trips listed and assert that no other agencies will reimburse them for the same expenses. A signature is required to confirm this declaration, along with necessary witness signatures if applicable. The form also includes a section for further detail if needed, allowing for a medical review to determine eligibility. Additionally, it highlights the patient's rights regarding the privacy of their medical information, providing guidelines for accessing and correcting personal data held by the state.
E Khc 3 Example
Kidney Health Care
Travel Claim Form for Home Dialysis and Kidney Transplant Patients
Client Information
Last Name
First Name
Middle Initial
Phone Number
Social Security Number (optional)
KHC Number
Trip Information
Provide your monthly travel details by filling in all four columns of this table. For the last column, choose the code from the list below that best describes the reason for your trip. You will only be reimbursed for four trips you already traveled per month which is related to
Access Surgery |
AS |
Epogen |
EP |
Peritoneal Clinic Visit |
PC |
Access Complication |
AC |
Lab tests, |
XR |
Tests before your transplant |
BT |
PD Support |
PD |
Nephrologist Visit |
NE |
Transplant Surgery |
TS |
AT |
|
|
|
|
If the reason for your trip is not on the list, then: (1) Check the box marked ‘Other’ and (2) Fill in the back of this form.
|
Date |
|
|
Name of Person or Place You |
|
|
Full Location Address |
|
|
Reason for Trip |
|
|
|
|
|
|
|
|
|
(Use a code from list above or |
|
||||
|
MM/DD/YY |
|
|
Went to See |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
choose ‘Other’) |
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
(Fill in the back) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
(Fill in the back) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
(Fill in the back) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
(Fill in the back) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Client Acknowledgement
I agree that each trip shown above was for travel and mileage that is allowed. I also agree that no other agency can pay me back for the trip and mileage. I understand that if I hold back any facts or submit information that is not true, I may be doing something that is against the law, which in that case I could lose my benefits, have to pay money back, or face legal actions.
Client Signature
Witness Signature (if client cannot sign)
Kidney Health Care • MC 1938 • PO Box 149347 • Austin, Texas
Last Name |
First Name |
Middle Initial |
KHC Number
Fill in the blanks below only if you have checked the box ‘Other’ on the other side of this form. KHC needs to know some things in order to figure out if it can pay for your trip(s). If you have trouble filling this part out, you can ask for help from your doctor or someone else from where you get your care.
If KHC has already reviewed and approved your travel for this condition, you only need to fill out Field number 3.
1.Date of Trip(s):
2.Where did you go? Place or Doctor’s Name(s), Street Address(es), and Phone Number(s):
3. Describe how the trip is related to your
KHC will do a medical review with this information. KHC may call your doctor(s) for more information. KHC will tell you its decision after it does the review. If KHC decides that the trip(s) are related to
For Use By KHC Reviewer ONLY
Reviewer
Date
Allow Trip(s)
Disallow Trip(s)
Comments:
Notice about Your Right to Privacy
Except in some cases, you have the right to ask for and know the information the State of Texas has about you. You can ask for it at any time. You can get it and make sure it is right. You have the right to ask the state agency to correct anything that is wrong. See http://hhs.texas.gov for more information on Your Right to Privacy. (Reference: Government Code, Section 552.021, 552.023, 559.003 and 559.004)
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose | The E Khc 3 form is designed for kidney health care travel claims specifically for home dialysis and kidney transplant patients. |
| Patient Information | It requires basic client details, including last name, first name, phone number, and optional Social Security number. |
| Monthly Travel Limits | Patients can claim reimbursement for up to four trips per month related to their condition. |
| Travel Codes | An array of codes is provided to categorize trips, such as "Access Surgery" or "Nephrologist Visit." |
| Client Acknowledgment | Patients must acknowledge the accuracy of their submitted information and cannot receive reimbursement from any other agency. |
| Legal Consequences | Submitting false information may result in losing benefits, being obligated to repay, or facing legal action. |
| Privacy Rights | Patients have the right to access their information held by the State of Texas, as outlined in Government Code sections 552.021, 552.023, 559.003, and 559.004. |
Guidelines on Utilizing E Khc 3
Once you have gathered the necessary information, filling out the E KHC 3 form is straightforward. This form is essential for individuals undergoing kidney health care who wish to claim travel expenses. Accurate completion is crucial to ensure timely processing of your claim.
- Provide your Client Information. Fill in your last name, first name, middle initial, phone number, optional social security number, and KHC number in the designated fields.
- For the Trip Information, complete the table provided by entering the date, name of the person or facility you visited, full location address, and the reason for your trip using the appropriate code from the provided list.
- List up to four trips in the table. Make sure to place the correct *reason codes* (such as AS for Access Surgery or NE for Nephrologist Visit) in the last column. If your trip reason is not listed, check the box marked 'Other' and note that on the back of the form.
- In the Client Acknowledgement section, affirm your agreement by signing the form. If you cannot sign, a witness must sign in the designated area.
- If you checked 'Other', fill in the back of the form. Include the date of trip(s), locations visited (including street addresses and phone numbers), and a brief explanation of how your trips relate to your end-stage renal disease or kidney transplant.
- Once completed, submit the form to the address provided at the bottom of the form, ensuring you retain a copy for your records.
Keep in mind that KHC may conduct a medical review based on the information provided. It is advisable to have support from your healthcare provider if you encounter difficulties while filling out the form. KHC will inform you of its decision after reviewing your submissions.
What You Should Know About This Form
What is the purpose of the E Khc 3 form?
The E Khc 3 form is specifically designed for individuals undergoing home dialysis or kidney transplant procedures. It serves as a travel claim form that allows these patients to request reimbursement for related travel expenses. Patients can document their trips, outlining the reasons and ensuring they stay compliant with the guidelines set forth by the Kidney Health Care program.
Who qualifies to use this form?
This form is intended for kidney health care clients who suffer from end-stage renal disease or those who have undergone a kidney transplant. If you have a KHC number and are making travel related to medical appointments, check-ups, or related treatments, you can utilize this form to seek reimbursement for your trip expenses.
How do I fill out the trip information section?
To complete the trip information section, you will need to provide details of your monthly travels. This includes stating the date, the name of the person or facility you visited, the full location address, and the reason for your trip. You’ll select a code from a provided list that categorizes your reason for travel—such as a check-up or a clinic visit. Remember, you can only claim up to four trips per month, so keep that in mind while filling it out.
What if my reason for travel is not listed on the form?
If your reason for travel doesn’t appear on the list provided, you can check the box labeled “Other.” Then, it’s essential to provide additional details on the back of the form. This helps the Kidney Health Care program understand the specifics of your situation. They may reach out to your healthcare provider for further clarification, so ensure the information is as accurate and complete as possible.
What happens after I submit the E Khc 3 form?
After you submit your E Khc 3 form, the Kidney Health Care program will conduct a review. They might contact your doctor for further information related to your travel and treatment. Once a decision is made, you will be informed of their review outcome. If approved, your file will be updated, allowing for easier reimbursement for future related trips. It’s crucial to keep a copy of the submitted form for your records.
Common mistakes
When completing the E Khc 3 form, individuals commonly make several mistakes that can lead to delays or complications in their claims. One frequent error is failing to provide complete information in the Client Information section. Omitting crucial details such as the full name or KHC number can result in confusion and hinder the processing of the claim. Always ensure that every required field is filled out accurately.
Another mistake is seen when travelers neglect to include all four reasons for their trips in the Trip Information section. The form allows for reimbursement of up to four trips per month related to end-stage renal disease or kidney transplants. If fewer trips are recorded, clients may face limits on reimbursement, potentially leaving them with out-of-pocket expenses. Keeping a clear record of trips is essential.
A third pitfall occurs with the selection of trip reasons. Some clients choose codes inaccurately or fail to select an appropriate code altogether. This not only complicates the review process but can also lead to outright denial of the claim. Clients should familiarize themselves with the provided codes beforehand to ensure accurate selection that reflects their travel purpose.
Lastly, there is the issue of signatures in the Client Acknowledgment section. Clients sometimes forget to sign or mistakenly leave the witness signature blank if they cannot sign themselves. This oversight can void the claim entirely. Always double-check that all necessary signatures are provided before submitting the form.
Documents used along the form
When completing the E Khc 3 form, additional documentation may be needed to support your travel claims related to kidney health care. Below is a list of other forms and documents that are often used in conjunction with this form. Each document plays a critical role in ensuring that your travel claims are accurate and adequately supported.
- Patient Referral Form: This document is typically used when a patient is referred to a specialist or different facility for treatment. It helps provide context about why the trip is necessary.
- Medical Treatment Verification Form: Patients may need to submit this form to verify that the medical treatment was related to their kidney condition. It often requires a doctor's signature.
- Travel Itinerary: A detailed travel plan outlining the dates, locations, and purposes of trips. This document helps clarify any travel-related questions that might arise during reimbursement processing.
- Mileage Log: This log tracks the miles traveled for each trip, which is vital for calculating reimbursements. It ensures all reported mileage aligns with what KHC considers allowable.
- Patient Medical Records: These records may be requested to substantiate the medical necessity of the trips. They usually include details about diagnoses, treatments, and doctors' notes.
- Consent for Release of Information Form: This consent form allows healthcare providers to share necessary information with the Kidney Health Care program. It is a crucial step in protecting patient privacy while ensuring that KHC has the relevant details to process claims.
By gathering these additional documents, you can enhance your claim’s accuracy and completeness. This collaborative approach with your healthcare provider can lead to a smoother and more efficient reimbursement process.
Similar forms
- Medicare Travel Claim Form: Similar to the E Khc 3 form, this document allows patients to claim reimbursement for travel related to medical care under Medicare. It requires patient details and trip information, ensuring that all claims are valid and necessary for treatment.
- Medicaid Travel Reimbursement Form: This form serves a similar purpose for Medicaid recipients. It documents travel for medical services and requires the patient's signature, highlighting compliance with travel-related reimbursement rules.
- Health Insurance Travel Claim Form: Patients submit this document to their health insurance provider for reimbursement of travel expenses incurred during medical treatment. Like the E Khc 3 form, it demands specific trip details and verification of medical necessity.
- Veteran's Administration Travel Claim Form: This document allows veterans to claim travel expenses for medical appointments or treatments. Much like the E Khc 3, it focuses on documenting the trip purpose and specifics to ensure reimbursement eligibility.
- Worker's Compensation Travel Claim Form: Similar in function, this form helps employees request reimbursement for travel related to work-related injuries. It necessitates details regarding the trip and its connection to the claim, paralleling the process outlined in the E Khc 3 form.
- Transportation Request Form for Patients: Used in healthcare facilities, this document requests transportation services for patients needing assistance to and from appointments. It shares a common goal with the E Khc 3 form by ensuring patients receive necessary care.
- Hospital Outpatient Travel Claim Form: Patients use this form to seek reimbursement for travel expenses incurred when receiving outpatient services. It adheres to a similar structure by requiring trip details and the purpose of travel.
- Medical Transportation Authorization Form: This document is used to authorize non-emergency medical transportation. It aligns with the E Khc 3 in terms of confirming travel necessity related to medical appointments.
- Chronic Care Management Travel Claim: Similar to the E Khc 3, this form is utilized for travel reimbursement related to chronic condition management appointments, focusing on ensuring proper documentation for validation.
- Medically Necessary Travel Verification Form: This form supports claims by verifying that travel was medically necessary. It complements the E Khc 3 by emphasizing the importance of connecting trip details with the medical condition being treated.
Dos and Don'ts
Things to Do:
- Provide accurate and complete information for each trip, including dates and reasons.
- Use the provided codes for trip reasons whenever applicable.
- Sign the Client Acknowledgement section to confirm your information is true.
- Fill in the “Other” section completely if your trip does not fit the provided reasons.
Things to Avoid:
- Do not leave any required fields blank, as this may delay processing.
- Avoid including trips that are not related to end-stage renal disease or kidney transplant.
- Do not submit false information, as it could lead to legal issues or loss of benefits.
- Refrain from using codes that are not on the list provided.
Misconceptions
Misconceptions about the E Khc 3 form can lead to confusion and mistakes in the application process. Here are some common misunderstandings:
- Only one trip can be claimed per month. Many people think they can only claim one trip, but you can actually claim up to four trips related to end-stage renal disease or kidney transplant per month.
- You must have a doctor's signature for all trips. While you can ask a doctor for help, a doctor’s signature is only necessary if the client cannot sign the form themselves.
- The code for the reason for the trip is optional. In fact, you must choose a code from the provided list to specify the reason for your trip, as this information is crucial for the review process.
- Trips unrelated to dialysis or transplant are reimbursable. Trips must be specifically related to end-stage renal disease or kidney transplant to qualify for reimbursement.
- Submitting false information is minor. It can lead to serious consequences, including loss of benefits and possible legal actions.
- You need to fill out the entire form every time. If KHC has previously approved your travel, you only need to complete Field number 3 on the section for ‘Other’ trips.
- Privacy rights are not important. You have the right to request and correct any personal information the State of Texas has about you, which is an important aspect of the process.
- Your Social Security Number is mandatory. Providing your Social Security Number is optional, though it may assist in identifying your file quicker.
Key takeaways
Here are some key takeaways regarding the E Khc 3 form for kidney health care travel claims:
- Understand the Purpose: This form is designed for home dialysis and kidney transplant patients to claim travel reimbursement related to their medical care.
- Client Information: Fill out your personal details accurately, including your last name, first name, and KHC number. Phone numbers and social security numbers are optional.
- Trip Information: You must provide details about your trips. The form has a table where you give the date, person or place visited, full location address, and the reason for your trip.
- Choose Correct Codes: It's important to select the appropriate code that describes the reason for your trip, such as “Access Surgery” or “Nephrologist Visit.”
- Limit on Reimbursements: You can only get reimbursed for up to four trips per month related to your condition.
- Fill Out ‘Other’: If your trip reason doesn’t fit the provided codes, check the ‘Other’ box and complete the additional section at the back of the form.
- Client Acknowledgement: You must agree that all trips were for approved travel. Acknowledge that you cannot receive reimbursement from any other agency.
- Legal Implications: Be truthful in your responses. Providing false information could lead to legal consequences, including loss of benefits.
- Right to Privacy: You have the right to access and correct your information held by the State of Texas. If needed, you can request help from your healthcare team when filling out the form.
It’s essential to follow these guidelines carefully to ensure your claims are processed smoothly. If you have questions or concerns, reach out for assistance.
Browse Other Templates
Self Storage Rent - Awareness of the exclusions and limitations is essential for making informed decisions about added insurance.
Player Contract Template - Missed training sessions and games come with specific penalties as detailed in the contract.