Fill Out Your Fmlv 001 Form
The Fmlv 001 form, known as the Certification of Physician or Practitioner, is a vital document under the Family and Medical Leave policies of the Navajo Nation. This form plays a crucial role in allowing employees to take time off for serious health conditions affecting themselves or their family members. It requires the detailing of both the employee’s and patient’s names and explores specific health conditions that may qualify for medical leave. To aid in the certification process, the form provides a checklist of categories that define a "serious health condition," which the physician or practitioner must assess. Key details include the commencement date of the condition, estimated duration, and whether the employee may need to work intermittently or on a reduced schedule due to these circumstances. Additionally, the form requires a description of necessary treatments and their anticipated frequency, along with any other health services required. It further examines the capacity of the employee to perform essential job functions and considers the need for leave to provide care for a family member whose health condition warrants assistance. Benefitting both the employee and employer, the Fmlv 001 form is designed to ensure that the rights and responsibilities surrounding medical leave are respected and that there is an understanding of the medical necessity for such leave.
Fmlv 001 Example
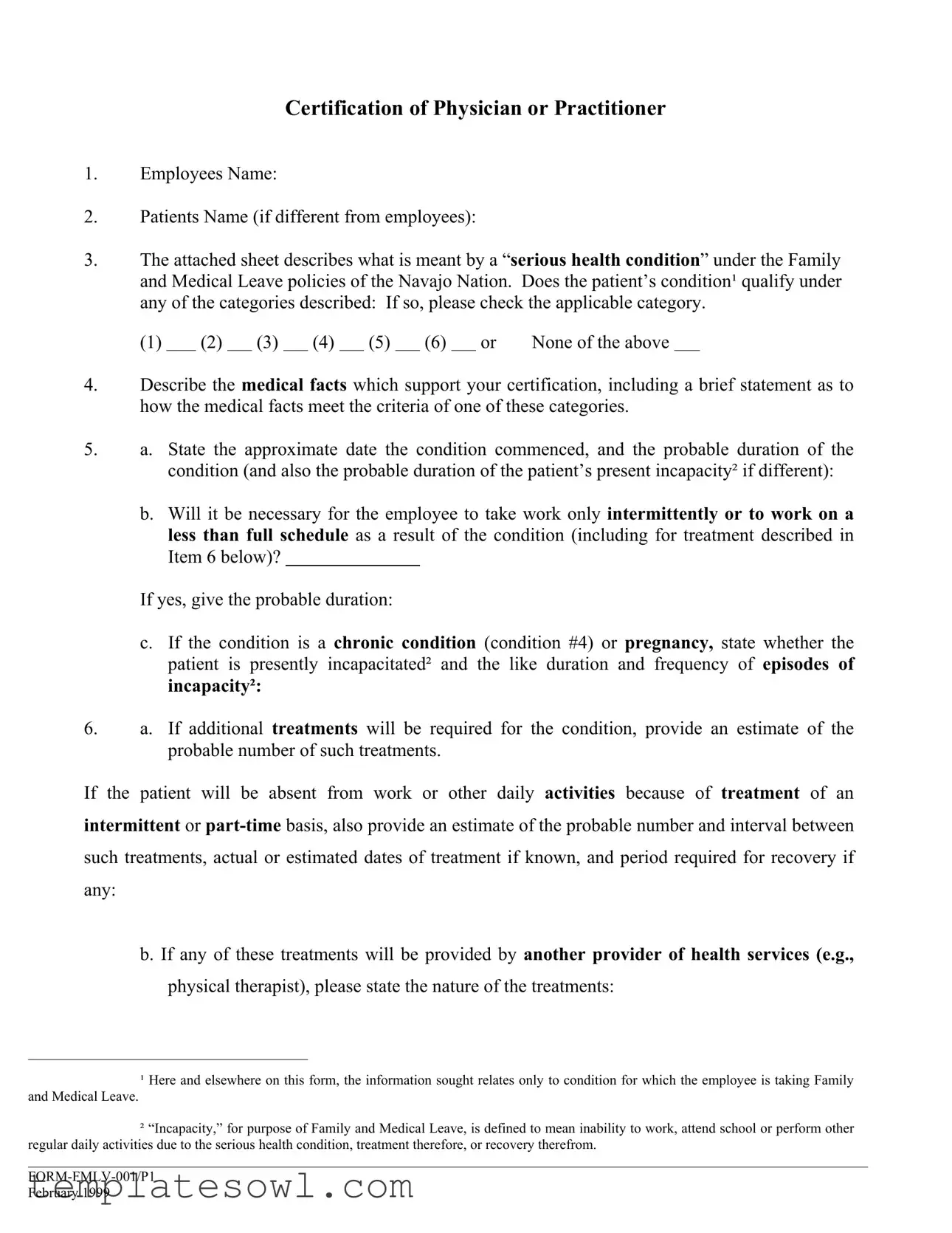
Certification of Physician or Practitioner
1.Employees Name:
2.Patients Name (if different from employees):
3.The attached sheet describes what is meant by a “serious health condition” under the Family and Medical Leave policies of the Navajo Nation. Does the patient’s condition¹ qualify under any of the categories described: If so, please check the applicable category.
(1) |
|
(2) |
|
(3) |
|
(4) |
|
(5) |
|
(6) |
|
or |
None of the above |
4.Describe the medical facts which support your certification, including a brief statement as to how the medical facts meet the criteria of one of these categories.
5.a. State the approximate date the condition commenced, and the probable duration of the condition (and also the probable duration of the patient’s present incapacity² if different):
b.Will it be necessary for the employee to take work only intermittently or to work on a less than full schedule as a result of the condition (including for treatment described in Item 6 below)?
If yes, give the probable duration:
c.If the condition is a chronic condition (condition #4) or pregnancy, state whether the patient is presently incapacitated² and the like duration and frequency of episodes of incapacity²:
6.a. If additional treatments will be required for the condition, provide an estimate of the probable number of such treatments.
If the patient will be absent from work or other daily activities because of treatment of an
intermittent or
such treatments, actual or estimated dates of treatment if known, and period required for recovery if
any:
b. If any of these treatments will be provided by another provider of health services (e.g.,
physical therapist), please state the nature of the treatments:
¹ Here and elsewhere on this form, the information sought relates only to condition for which the employee is taking Family
and Medical Leave.
²“Incapacity,” for purpose of Family and Medical Leave, is defined to mean inability to work, attend school or perform other regular daily activities due to the serious health condition, treatment therefore, or recovery therefrom.
February 1999
c.If a regiment of continuing treatment by the patient is required under your supervision, provide a general description of such regiment (e.g., prescription drugs, physical therapy requiring special equipment):
7.a. If medical leave is required for the employee’s absence from work because of the employee’s own condition (including absences due to pregnancy or a chronic condition), is the employee unable to work of any kind:
b.If able to perform some work, is the employee unable to perform any one or more of the essential functions of the employee’s job (the employee or the employer should supply you with information about the essential job functions)?
c.If neither a. or b. applies, is it necessary for the employee to be absent from work for treatment?
8.a. If leave is required to care for a family member of the employee with a serious health condition, does the patient require assistance for basic medical or personal needs or safety, or for transportation?
b.If no, would the employee’s presence to provide psychological comfort be beneficial to the patient or assist in the patient’s recovery?
c.If the patient will need care only intermittently or on a
(Signature of Health Care Provider) |
|
(Type of Practice) |
|
|
|
(Address) |
(Telephone number) |
|
To be completed by the employee needing family leave to care for a family member:
State the care you will provide and an estimate of the period during which care will be provided, including a schedule if leave is to be taken intermittently or if it will be necessary for you to work less than a full schedule:
(Employee signature) |
(Date) |
February 1999
Form Characteristics
| Fact Name | Description |
|---|---|
| Purpose | The FMLV 001 form is used to certify a serious health condition for Family and Medical Leave under the Navajo Nation policies. |
| Patient's Condition | The form requires the healthcare provider to determine if the patient's condition qualifies under defined categories from the attached guidelines. |
| Duration of Condition | The form includes sections to estimate the approximate date the condition began, its probable duration, and whether there is a need for intermittent leave. |
| Related Laws | The use of the FMLV 001 form is governed by the Family and Medical Leave Act (FMLA) and the Navajo Nation leave policies. |
Guidelines on Utilizing Fmlv 001
Once you have the Fmlv 001 form in hand, it's important to fill it out accurately. This ensures that all necessary information is provided for the Family and Medical Leave process to proceed smoothly. Carefully follow each step below to complete the form correctly.
- Employee's Name: Enter the full name of the employee requesting leave.
- Patient's Name: If the patient is different from the employee, provide the patient's name.
- Condition Qualification: Review the attached sheet and check the box for any category that applies to the patient’s serious health condition. If none apply, check "None of the above."
- Medical Facts: Write a brief description supporting the medical certification and explain how the patient’s condition meets the criteria of the selected category.
- Condition Details:
- State the approximate date the condition began and the expected duration.
- Indicate if the employee will need to work intermittently or on a reduced schedule due to the condition, and provide an estimated duration.
- If applicable, state whether the patient is currently incapacitated and provide details about the frequency and duration of any episodes.
- Treatment Frequency:
- Estimate how many additional treatments the patient will require.
- If treatments will keep the patient from daily activities, list the estimated frequency of those treatments and any required recovery period.
- Identify any additional health service providers who will deliver treatments, detailing the type of treatment.
- Continuing Treatment Description: If ongoing treatment is necessary, provide a general description of the regimen, such as medication or therapy types.
- Employee Condition:
- Determine if the employee is unable to work at all due to their own serious condition.
- If the employee can perform some work, specify if they cannot perform any key job functions.
- If applicable, clarify if the employee must be away from work for treatment.
- Family Member Care:
- Indicate if the patient requires assistance for basic needs or transportation.
- If not, assess whether the employee’s presence would provide psychological comfort or aid recovery.
- For intermittent care needs, specify the likely duration of care required.
- Provider Signature: The health care provider should sign and include their type of practice, address, and telephone number.
- Employee Care Commitment: The employee must state the care they will provide, including the estimated duration and any scheduled leaves.
- Sign and Date: Finally, have the employee sign and date the form.
What You Should Know About This Form
What is the purpose of the FMLV 001 form?
The FMLV 001 form is designed to certify a serious health condition under the Family and Medical Leave Act (FMLA) for employees. This form helps document the need for medical leave, whether due to an employee's own health condition or to care for a family member. It provides necessary information for employers to make informed decisions regarding leave requests.
Who needs to fill out the FMLV 001 form?
The form needs to be completed by a health care provider who is responsible for the employee's care or the family member's care. Additionally, the employee may need to fill out specific sections to outline their intended care and the duration of the leave they may need. Both the health care provider and the employee play crucial roles in ensuring that the information is complete and accurate.
What types of health conditions qualify under the FMLV 001 form?
The form outlines various categories that describe what constitutes a "serious health condition." Commonly, this includes conditions that require inpatient care, ongoing medical treatment, or chronic health issues that affect daily activities. It is important to review the attached sheet on the form that details each category to determine if the patient’s condition applies.
What specific information must a health care provider provide on the form?
A health care provider must detail the patient’s medical condition, its duration, and how it meets the criteria for a serious health condition. In addition, the provider should describe any necessary treatments, the expected frequency of visits, and if the patient requires assistance with daily activities. This information is essential for the employer to understand the necessity of the leave.
Can an employee take intermittent leave under the FMLV 001 form?
Yes, employees can request intermittent leave, and the form allows for this option to be documented. If the employee needs to take leave on a part-time basis or only occasionally, this should be clearly stated on the form. Accurate estimates of the probable duration and schedule of such leave are necessary to facilitate the approval process.
What should I do if I have questions while completing the FMLV 001 form?
If you encounter questions or uncertainties while filling out the FMLV 001 form, it's always a good idea to consult with your HR department or your health care provider. They can provide guidance on completing the form correctly and ensuring that all necessary information is included to support your case for leave.
Is there a deadline for submitting the FMLV 001 form?
Yes, there are typically deadlines for submitting the FMLV 001 form, which may vary by employer. Generally, it should be submitted as soon as the need for leave is known, ideally before the leave begins. Check with your HR department for specific timelines to ensure compliance with your employer's policies.
Common mistakes
When filling out the FMLV 001 form, several common mistakes can hinder the approval process for Family and Medical Leave. First, individuals often neglect to provide complete and accurate information about the patient's condition. Missing or vague details on how the condition meets the criteria outlined in the attached sheet can lead to confusion. It is critical to include specific medical facts that clearly illustrate the severity of the health issue.
Another frequent error is failing to check the appropriate category for the serious health condition. Skipping this step can result in unnecessary delays or even rejections of the request. Each category has distinct requirements, and assuring that one is marked accurately can make a significant difference.
Alongside these, individuals often underestimate the importance of estimated dates. Inaccurately stating the commencement and probable duration of the condition can lead to misinterpretation of the need for leave. Providing precise dates allows for better planning and support from the employer during the employee's time off.
Moreover, people sometimes overlook details regarding the necessity for intermittent leave. If a person can work on a reduced schedule or needs to take time off periodically, this information must be explicitly stated. Indicating the probable duration and frequency of leave contributes to clarity in the application process.
In addition, an incomplete description of treatment regimens poses a major issue. When outlining future treatments, failing to provide estimates regarding frequency and type can create confusion. This information is crucial for judges and employers to assess the legitimacy of the leave request.
Another mistake relates to how the employee’s own incapacity is described. Respondents often provide insufficient information on whether the employee can perform essential job functions. Clear communication regarding the employee's capacity to work in any form is necessary for decision-makers.
Moreover, caregivers often forget to specify the type of assistance the family member requires. If the need for help with basic medical tasks or personal care is unclear, this can justly raise doubts about the legitimacy of the care required. Clarity on the necessity of the employee's presence for psychological support is also essential.
Lastly, one should always ensure to sign and date the form. Missing a signature or the date could result in the form being deemed invalid. A complete and well-prepared FMLV 001 form demonstrates thoroughness and respect for the process, ultimately aiding in a smoother leave application experience.
Documents used along the form
When navigating the process of taking family or medical leave, several forms and documents often accompany the FMLV 001 form, known for certifying the need for leave based on health conditions. Each document serves a unique purpose and helps clarify the situation. Below is a summary of some of the most commonly used forms you may encounter.
- FMLV 002 – Leave Request Form: This form is submitted by the employee to formally request family or medical leave. It outlines the specific dates leave is needed and the type of leave being requested.
- FMLV 003 – Medical Verification Form: This document is required to gather additional medical information from the healthcare provider, ensuring that the employee's situation meets the eligibility criteria for leave.
- FMLV 004 – Recertification Form: Sometimes, ongoing medical conditions require the employee to provide updated information. This form is used for recertifying the need for leave after the initial approval period.
- FMLV 005 – Family Member Information Form: This form allows the employee to provide details about the family member requiring care, including their health condition and the anticipated duration of support needed.
- FMLV 006 – Employee Status Report: Employees might need to submit this report to update their employer about their condition and work readiness during the leave period.
- FMLV 007 – Claim for Benefits Form: This document is necessary if the employee is seeking benefits related to their leave, such as short-term disability or family leave insurance.
- FMLV 008 – Return to Work Certificate: Prior to returning to work, the employee must provide this certification to confirm they are fit to resume their job duties without restrictions, ensuring a smooth transition back to the workplace.
- FMLV 009 – Fitness for Duty Form: In some cases, an employer may require this form to verify that an employee is fully able to perform their job as expected before they can return to work.
Understanding these forms and documents can streamline the leave process, ensuring that both the employee's needs and the employer’s requirements are met efficiently. Being prepared can make a significant difference during what can be a challenging time.
Similar forms
- FMLA Certification of Health Care Provider (Form WH-380): Similar in purpose, this form is used to certify a serious health condition under the Family and Medical Leave Act. Both require detailed medical information about the patient’s condition, including the duration and the necessity of leave.
- Medical Leave Request Form: This document serves to formally request medical leave. Like the FMLV 001 form, it outlines the reason for leave and requires medical verification supporting the request.
- Employee’s Statement of Health Care Provider (Form FMLA-4): This form is designed to provide verification of the employee’s need for FMLA leave. It shares similarities in detailing the health condition and its impact on the employee’s ability to work.
- Personal Medical Leave Form: Often used by companies for employees needing leave due to health issues, this form likewise documents the medical reason for absence and the expected length of time off.
- Family Care Certification Form: This document certifies the need for leave to care for a family member. It, too, collects information about the family member’s health condition and the caregiver’s responsibilities.
- Returning from Leave Form: Employers often require this form to confirm an employee's readiness to return to work after leave. It provides details on recovery and any ongoing care needs, paralleling the certification aspect of the FMLV 001 form.
- Employer's Request for Medical Information: This form, used by employers to gather necessary medical details, mirrors the information sought in FMLV 001, ensuring consistency in understanding an employee’s health condition.
- Chronic Illness Report Form: Used for employees with long-term health issues, it gathers information on condition management and support requirements, similar to the information collected in the FMLV 001.
- Disability Leave Request Form: This form requests leave due to disability and similarly requires medical documentation supporting the leave request, focusing on the employee's ability to work.
- Compassionate Care Leave Form: This document allows employees to request leave to care for a loved one with serious health issues. It parallels the FMLV 001 in detailing care requirements and medical specifics.
Dos and Don'ts
When filling out the Fmlv 001 form, it is essential to be diligent and thoughtful. Below is a guide outlining nine important dos and don’ts to consider during this process.
- Do read the entire form carefully before starting.
- Do ensure all names are accurately spelled, including both the employee's and the patient's names.
- Do provide detailed descriptions of the medical facts to support your certification.
- Do note the dates related to the condition, including when it started and potential duration.
- Do clarify whether the employee can perform essential job functions.
- Don’t leave any section blank or incomplete unless it is explicitly indicated as optional.
- Don’t use vague terms; be as specific as possible about the medical treatments required.
- Don’t falsify or exaggerate information regarding the condition or treatment needs.
- Don’t forget to sign and date the form appropriately before submission.
Taking care to follow these guidelines can help ensure that the form is filled out correctly, facilitating a smoother process for obtaining family and medical leave. Compassion and accuracy are key in this serious matter.
Misconceptions
Understanding the FMLV 001 form can feel overwhelming, especially with the various assumptions people tend to make about it. Here are six common misconceptions, along with clarifications to help you navigate the requirements confidently.
- This form is only for employees with serious illnesses. Many believe that the FMLV 001 form is exclusively for employees suffering from severe health conditions. In reality, the form can also be used for cases involving chronic conditions, pregnancy, or when caring for a family member with a serious health issue.
- The form must be completed by the employee. Some individuals think that only the employee can fill out the FMLV 001 form. However, the certification requires input from a healthcare provider, emphasizing the medical aspects that support the need for leave.
- Certification is immediate once the form is submitted. A common assumption is that submission of the FMLV 001 form guarantees immediate approval for leave. Approval involves a review process by the employer, who will determine if all criteria are met based on the healthcare provider's certification.
- All health conditions are automatically covered. There is a misconception that any health condition qualifies for leave without further assessment. In truth, only those conditions defined as "serious" under Family and Medical Leave policies will be accepted, reinforcing the importance of following the specific definitions outlined in the form.
- Intermittent leave is not an option. Some believe that the FMLV 001 form only allows for continuous leave. This is false; the form includes provisions for intermittent leave, allowing employees to take time off as needed based on their situations.
- Once approved, the employee cannot return to work until fully recovered. It is often assumed that once leave is taken, the employee must remain out of work until complete recovery. In actuality, employees may return to work on a part-time basis or modify their schedules as their health allows.
Being informed about the true nature of the FMLV 001 form can help alleviate anxiety surrounding the process. It is essential to approach it with accurate knowledge, ensuring that both employees and their healthcare providers fill it out effectively. Doing so will facilitate smoother communication and a better understanding of the rights and responsibilities of those involved.
Key takeaways
Filling out the FMLV 001 form, which certifies a serious health condition, is a crucial step in applying for Family and Medical Leave with the Navajo Nation. Here are some key takeaways to guide you through the process:
- Understand the Purpose: This form is designed to certify that an employee has a serious health condition or needs to care for someone with such a condition.
- Complete Accuracy: Ensure that every section is filled out accurately. Incomplete or incorrect information may delay approval.
- Clearly Identify Names: Clearly specify the employee’s name and, if applicable, the name of the patient. This helps avoid confusion.
- Assess Eligibility: Review the attached sheet for categories that define a “serious health condition.” Check the applicable box if the patient qualifies.
- Provide Medical Facts: Describe the medical facts supporting your certification. A detailed explanation can strengthen the application.
- Indicate Dates: Provide approximate dates for when the condition started, how long it may last, and any expected absences from work.
- Intermittent Leave: If the employee needs to take leave intermittently or work reduced hours, specify the expected duration of this need.
- Detail Treatment Requirements: Include information about any additional treatments necessary for the patient, including why those treatments are needed.
- Sign the Form: A healthcare provider must sign the form. Their signature adds credibility and confirms the assessment provided.
- Employee's Responsibility: The employee should also provide a detailed account of the care they will offer and how long they anticipate needing leave.
By following these guidelines, you can help ensure the FMLV 001 form is completed correctly. This precision can streamline the process of obtaining Family and Medical Leave, allowing the employee to focus on recovery or caregiving without unnecessary delays.
Browse Other Templates
How to Apply for Leave of Absence - Submitting the form does not guarantee approval; official response will follow.
Nyc Commercial Rent Tax Due Dates - Forms must be filled out using either printed or typed information.