Fill Out Your Har 3 Form
The Har 3 form, specifically the Health Assessment Record issued by the State of Connecticut Department of Education, serves as a crucial document that captures important health information about students. This form comprises two main parts. The first part is designed for parents or guardians, collecting essential health history and information about the student, such as existing medical conditions, medications, and insurance details. It prompts caregivers to reflect on their child's health and report significant issues, ranging from allergies to past hospitalizations. In contrast, Part II is to be completed by a qualified healthcare provider during the medical evaluation and physical examination. This section reviews the health history provided and mandates various screenings like vision and hearing tests, ensuring that students meet health standards before entering school. Connecticut state law highlights the necessity of complete immunizations and health assessments, mandated prior to school enrollment, and also outlines requirements for additional evaluations during specific grade levels. Furthermore, the form addresses the needs of physically active students, supporting annual health assessments for those participating in sports. Collectively, the information gathered through the Har 3 form plays a pivotal role in fostering an environment conducive to the academic and physical well-being of students.
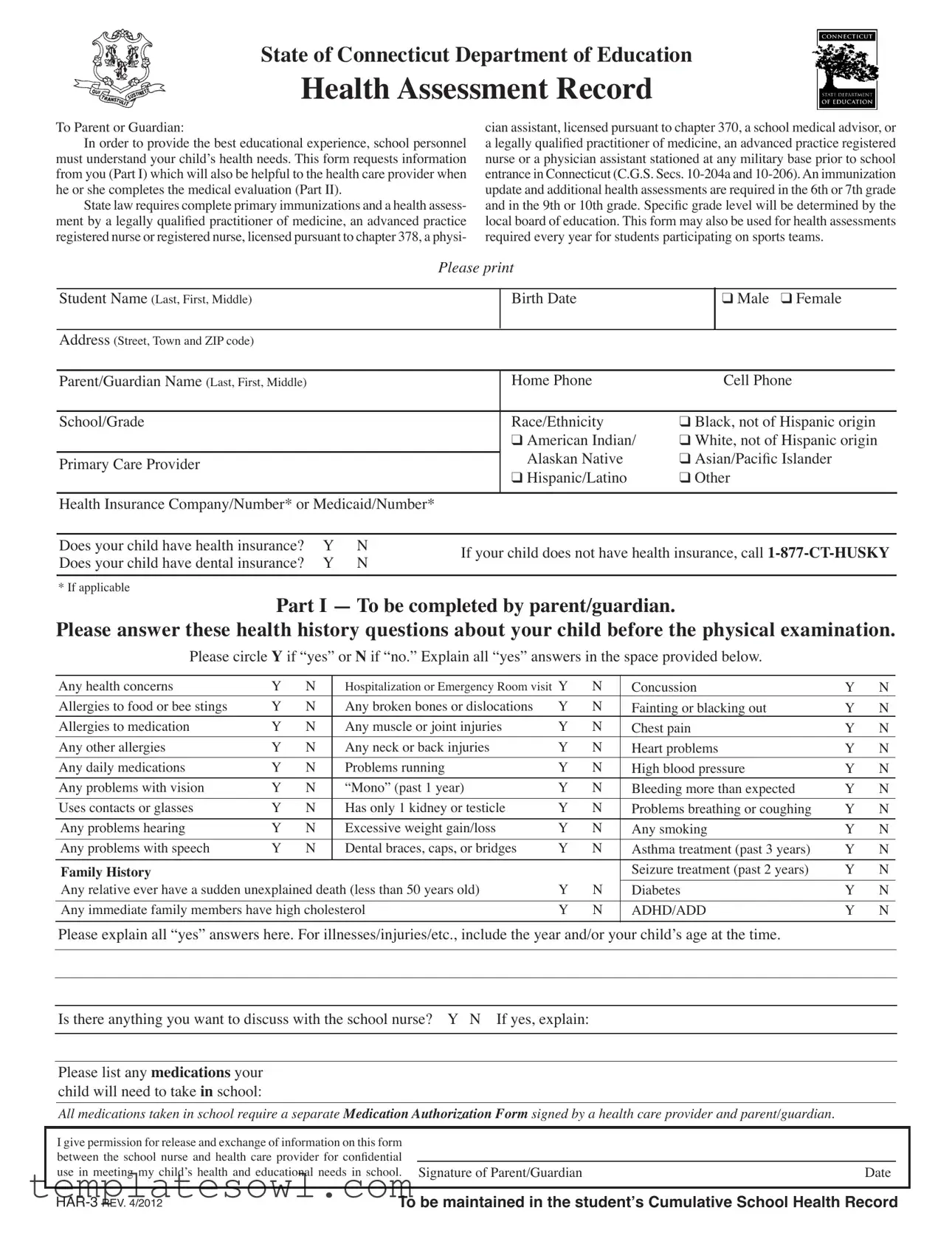
Har 3 Example
State of Connecticut Department of Education
Health Assessment Record
To Parent or Guardian:
In order to provide the best educational experience, school personnel must understand your child’s health needs. This form requests information from you (Part I) which will also be helpful to the health care provider when he or she completes the medical evaluation (Part II).
State law requires complete primary immunizations and a health assess- ment by a legally qualiied practitioner of medicine, an advanced practice
registered nurse or registered nurse, licensed pursuant to chapter 378, a physi-
cian assistant, licensed pursuant to chapter 370, a school medical advisor, or a legally qualiied practitioner of medicine, an advanced practice registered
nurse or a physician assistant stationed at any military base prior to school entrance in Connecticut (C.G.S. Secs.
update and additional health assessments are required in the 6th or 7th grade and in the 9th or 10th grade. Speciic grade level will be determined by the
local board of education. This form may also be used for health assessments required every year for students participating on sports teams.
Please print
Student Name (Last, First, Middle)
Birth Date
❑Male ❑ Female
Address (Street, Town and ZIP code)
Parent/Guardian Name (Last, First, Middle) |
Home Phone |
Cell Phone |
|
|
|
|
|
School/Grade |
Race/Ethnicity |
❑ Black, not of Hispanic origin |
|
|
❑ American Indian/ |
❑ White, not of Hispanic origin |
|
|
Alaskan Native |
❑ Asian/Paciic Islander |
|
Primary Care Provider |
|||
|
❑ Hispanic/Latino |
❑ Other |
|
|
|
|
|
Health Insurance Company/Number* or Medicaid/Number*
Does your child have health insurance? |
Y |
N |
If your child does not have health insurance, call |
|
Does your child have dental insurance? |
Y |
N |
||
|
||||
|
|
|
|
|
* If applicable |
|
|
|
Part I — To be completed by parent/guardian.
Please answer these health history questions about your child before the physical examination.
Please circle Y if “yes” or N if “no.” Explain all “yes” answers in the space provided below.
Any health concerns |
Y |
N |
Hospitalization or Emergency Room visit Y |
N |
Concussion |
Y |
N |
|
Allergies to food or bee stings |
Y |
N |
Any broken bones or dislocations |
Y |
N |
Fainting or blacking out |
Y |
N |
Allergies to medication |
Y |
N |
Any muscle or joint injuries |
Y |
N |
Chest pain |
Y |
N |
Any other allergies |
Y |
N |
Any neck or back injuries |
Y |
N |
Heart problems |
Y |
N |
Any daily medications |
Y |
N |
Problems running |
Y |
N |
High blood pressure |
Y |
N |
Any problems with vision |
Y |
N |
“Mono” (past 1 year) |
Y |
N |
Bleeding more than expected |
Y |
N |
Uses contacts or glasses |
Y |
N |
Has only 1 kidney or testicle |
Y |
N |
Problems breathing or coughing |
Y |
N |
|
|
|
|
|
|
|
|
|
Any problems hearing |
Y |
N |
Excessive weight gain/loss |
Y |
N |
Any smoking |
Y |
N |
Any problems with speech |
Y |
N |
Dental braces, caps, or bridges |
Y |
N |
Asthma treatment (past 3 years) |
Y |
N |
|
|
|
|
|
|
|
|
|
Family History |
|
|
|
|
|
Seizure treatment (past 2 years) |
Y |
N |
Any relative ever have a sudden unexplained death (less than 50 years old) |
Y |
N |
Diabetes |
Y |
N |
|||
|
|
|
|
|
|
|||
Any immediate family members have high cholesterol |
Y |
N |
ADHD/ADD |
Y |
N |
|||
|
|
|
|
|
|
|
|
|
Please explain all “yes” answers here. For illnesses/injuries/etc., include the year and/or your child’s age at the time.
Is there anything you want to discuss with the school nurse? Y N If yes, explain:
Please list any medications your child will need to take in school:
All medications taken in school require a separate Medication Authorization Form signed by a health care provider and parent/guardian.
I give permission for release and exchange of information on this form between the school nurse and health care provider for conidential
use in meeting my child’s health and educational needs in school. Signature of Parent/Guardian |
Date |
|
|
|
|
To be maintained in the student’s Cumulative School Health Record |
||
Part II — Medical Evaluation
Health Care Provider must complete and sign the medical evaluation and physical examination
Student Name |
|
Birth Date |
|
Date of Exam |
❑I have reviewed the health history information provided in Part I of this form
Physical Exam
Note: *Mandated Screening/Test to be completed by provider under Connecticut State Law
*Height _____ in. / _____% *Weight _____ lbs. / _____% |
BMI _____ / _____% Pulse _____ |
*Blood Pressure _____ / _____ |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Normal |
|
Describe Abnormal |
|
|
Ortho |
|
|
Normal |
|
Describe Abnormal |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Neurologic |
|
|
|
|
|
|
Neck |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HEENT |
|
|
|
|
|
|
Shoulders |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Gross Dental |
|
|
|
|
|
|
Arms/Hands |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lymphatic |
|
|
|
|
|
|
Hips |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Heart |
|
|
|
|
|
|
Knees |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lungs |
|
|
|
|
|
|
Feet/Ankles |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Abdomen |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Postural |
❑ No spinal |
❑ Spine abnormality: |
|||||||||
|
|
|
|
|
|
|
|
||||||||||
Genitalia/ hernia |
|
|
|
|
|
|
|
|
abnormality |
|
❑ Mild |
❑ Moderate |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❑ Marked ❑ Referral made |
|||
Skin |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Screenings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Vision Screening |
|
|
|
*Auditory Screening |
|
|
|
History of Lead level |
|
Date |
|||||||
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Type: |
Right |
Left |
|
Type: |
Right |
Left |
|
|
≥ 5µg/dL ❑ No ❑ Yes |
|
|
|
||||
|
|
|
|
|
|
❑ Pass |
❑ Pass |
|
|
|
|
|
|
||||
|
With glasses |
20/ |
20/ |
|
|
|
|
*HCT/HGB: |
|
|
|
||||||
|
|
|
|
|
|
|
❑ Fail |
❑ Fail |
|
|
|
|
|
|
|
|
|
|
Without glasses |
20/ |
20/ |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
*Speech (school entry only) |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
❑ Referral made |
|
|
|
❑ Referral made |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
Other: |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
TB: |
❑ No |
❑ Yes |
|
PPD date read: |
|
|
Results: |
|
|
|
Treatment: |
|
|
|
||
*IMMUNIZATIONS
❑Up to Date or ❑
*Chronic Disease Assessment:
Asthma |
❑ No |
❑ Yes: |
❑ Intermittent ❑ Mild Persistent ❑ Moderate Persistent ❑ Severe Persistent ❑ Exercise induced |
||||
|
If yes, please provide a copy of the Asthma Action Plan to School |
|
|||||
Anaphylaxis ❑ No |
❑ Yes: |
❑ Food |
❑ Insects |
❑ Latex |
❑ Unknown source |
|
|
Allergies |
If yes, please provide a copy of the Emergency Allergy Plan to School |
|
|||||
|
History of Anaphylaxis |
❑ No |
❑ Yes |
Epi Pen required ❑ No |
❑ Yes |
||
Diabetes |
❑ No |
❑ Yes: |
❑ Type I |
❑ Type II |
Other Chronic Disease: |
|
|
Seizures |
❑ No |
❑ Yes, type: |
|
|
|
|
|
❑This student has a developmental, emotional, behavioral or psychiatric condition that may affect his or her educational experience. Explain: ____________________________________________________________________________________________________
Daily Medications (specify): ____________________________________________________________________________________
This student may: ❑ participate fully in the school program
❑participate in the school program with the following restriction/adaptation: _____________________________
___________________________________________________________________________________________________________
This student may: ❑ participate fully in athletic activities and competitive sports
❑participate in athletic activities and competitive sports with the following restriction/adaptation: ____________
___________________________________________________________________________________________________________
❑Yes ❑ No Based on this comprehensive health history and physical examination, this student has maintained his/her level of wellness.
Is this the student’s medical home? ❑ Yes ❑ No ❑ I would like to discuss information in this report with the school nurse.
|
|
|
|
|
|
Signature of health care provider MD / DO / APRN / PA |
Date Signed |
Printed/Stamped Provider Name and Phone Number |
|
|
|
|
|
|
Student Name: ______________________________________ Birth Date: ___________________
Immunization Record
To the Health Care Provider: Please complete and initial below.
Vaccine (Month/Day/Year) Note: *Minimum requirements prior to school enrollment. At subsequent exams, note booster shots only.
|
Dose 1 |
Dose 2 |
|
Dose 3 |
|
Dose 4 |
|
Dose 5 |
|
Dose 6 |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
DTP/DTaP |
* |
* |
|
* |
|
* |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DT/Td |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Tdap |
* |
|
|
|
|
|
|
Required for 7th grade entry |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
IPV/OPV |
* |
* |
|
* |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MMR |
* |
* |
|
|
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Measles |
* |
* |
|
|
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Mumps |
* |
* |
|
|
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Rubella |
* |
* |
|
|
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
HIB |
* |
|
|
|
|
|
|
PK and K (Students under age 5) |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Hep A |
* |
* |
|
|
|
|
|
PK and K (born 1/1/2007 or later) |
|
|||
Hep B |
* |
* |
|
* |
|
|
|
Required |
|
|
||
Varicella |
* |
* |
|
|
|
|
|
2 doses required for K & 7th grade as of 8/1/2011 |
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
PCV |
* |
|
|
|
|
|
|
PK and K (born 1/1/2007 or later) |
|
|||
Meningococcal |
* |
|
|
|
|
|
|
Required for 7th grade entry |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
HPV |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Flu |
* |
|
|
|
|
|
|
PK students |
||||
Other |
|
|
|
|
|
|
|
|
|
|
|
|
Disease Hx ________________________________ |
________________________________ |
________________________________ |
|
|
||||||||
of above |
(Specify) |
|
|
(Date) |
|
|
|
(Conirmed by) |
|
|
|
|
|
|
|
|
Exemption |
|
|
|
|
|
|
|
|
|
Religious _____ Medical: Permanent _____ |
Temporary _____ |
Date _____ |
|
|
|
||||||
|
Recertify Date _________ Recertify Date _________ Recertify Date ________ |
|
|
|
||||||||
Immunization Requirements for Newly Enrolled Students at Connecticut Schools
KINDERGARTEN
•DTaP: At least 4 doses. The last dose must be given on or after 4th birthday.
•Polio: At least 3 doses. The last dose must be given on or after 4th birthday.
•MMR: 2 doses given at least 28 day apart – 1st dose on or after the 1st birthday.
•Hib: 1 dose on or after 1st birthday (Children 5 years and older do not need proof of Hib vaccination).
•Pneumococcal: 1 dose on or after 1st birthday (born 1/1/2007 or later and less than 5 years old).
•Hep A: 2 doses given six months
•Hep B: 3
•Varicella: For students enrolled before August 1, 2011, 1 dose given on or after 1st birthday; for students enrolled on or after August 1, 2011
2 doses given 3 months apart – 1st dose on or after 1st birthday or veriication of disease*.
GRADES
•DTaP /Td/Tdap: At least 4 doses. The last dose must be given on or after 4th birthday; students who start the series at age 7 or older only need a total of 3 doses of
•Polio: At least 3 doses. The last dose must be given on or after 4th birthday.
•MMR: 2 doses given at least 28 days apart- 1st dose on or after the 1st birthday.
•Hep B: 3 doses – the last dose on or after 24 weeks of age.
•Varicella: 1 dose on or after the 1st birthday or veriication of disease*.
GRADE 7
•Tdap/Td: 1 dose of Tdap for students 11 yrs. or older enrolled in 7th grade who completed their primary DTaP series; For those students who start the series at age 7 or older a total of 3 doses of
•Polio: At least 3 doses. The last dose must be given on or after 4th birthday.
•MMR: 2 doses given at least 28 days apart – 1st dose on or after the 1st birthday.
•Meningococcal: one dose for students enrolled in 7th grade.
•Hep B: 3
•Varicella: 2 doses given 3 months apart – 1st dose on or after 1st birthday or veriication of
disease*.
GRADES
•Td: At least 3 doses. Students who start the series at age 7 or older only need a total of 3 doses of
•Polio: At least 3 doses. The last dose must be given on or after 4th birthday.
•MMR: 2 doses given at least 28 days apart- 1st dose on or after the 1st birthday.
•Hep B: 3
•Varicella: For students <13 years of age, 1 dose given on or after the 1st birthday. For students
13 years of age or older, 2 doses given at least
4 weeks apart or veriication of disease*.
*Veriicationofdisease:Conirmation in writ- ing by a MD, PA, or APRN that the child has a previous history of disease, based on family or medical history.
Note: The Commissioner of Public Health may issue a temporary waiver to the schedule for active immunization for any vaccine if the National Centers for Disease Control and Prevention recognizes a
|
|
|
|
|
|
Initial/Signature of health care provider MD / DO / APRN / PA |
Date Signed |
Printed/Stamped Provider Name and Phone Number |
|
|
|
|
|
|
Form Characteristics
| Fact Name | Details |
|---|---|
| Purpose of the Form | The HAR 3 form is designed to gather health information relevant to a child's educational experience and health assessments. |
| State Governing Law | This form is governed by Connecticut General Statutes Sections 10-204a and 10-206, requiring health assessments and immunizations for school entry. |
| Immunization Requirement | State law mandates that children must have complete primary immunizations before entering school. Specific updates are required in the 6th or 7th grade and again in the 9th or 10th grade. |
| Health Insurance Query | The form includes questions regarding whether the child has health and dental insurance, providing resources for those who do not. |
| Disclosure of Medical Needs | Parents or guardians can discuss their child's specific health concerns and necessary medications, facilitating communication with school health personnel. |
Guidelines on Utilizing Har 3
Completing the HAR-3 form is a necessary step for ensuring that your child’s health needs are documented for school entry and participation in activities. The following steps will guide you through the process of filling out this form accurately and completely.
- Student Information: Print your child’s full name (last, first, middle) and birth date in the designated fields. Check the appropriate box for your child's gender.
- Contact Information: Provide your current address, including street, town, and ZIP code. Fill in your name as the parent or guardian, along with your home and cell phone numbers.
- School and Grade: Indicate the school your child will be attending and their current grade level.
- Race/Ethnicity: Check the box that best describes your child's race or ethnicity.
- Primary Care Provider: Enter the name of your child’s primary care provider and the name of the health insurance company or Medicaid number, if applicable.
- Health Insurance: Answer whether your child has health insurance and dental insurance by marking “Y” for yes or “N” for no.
- Health History Questions: Answer each question regarding your child's health by circling “Y” for yes or “N” for no. If any answers are “yes,” provide detailed explanations in the space provided.
- Medications: List any medications your child will need to take at school. Ensure you know that separate authorization is needed for these medications.
- Discussion with School Nurse: If there are any concerns to discuss with the school nurse, indicate “Y” for yes and provide details.
- Signature: Sign and date the form, confirming that the information you provided is accurate.
Next, ensure that the completed section is submitted to the appropriate school personnel, allowing school health staff to review the information and prepare for your child’s educational needs and health assessments.
What You Should Know About This Form
What is the purpose of the HAR 3 form?
The HAR 3 form, officially known as the Health Assessment Record, serves a critical role in ensuring that a student’s health needs are understood and addressed within the school environment. The form is divided into two parts: Part I, which is completed by a parent or guardian, gathers essential health information. This includes details about previous illnesses, allergies, medications, and any particular health concerns. Part II requires completion by a licensed health care provider, who conducts a physical examination and assesses the child's health status. Together, these sections help the school personnel provide the best educational experience possible by ensuring that any health challenges are adequately managed.
Who is required to fill out the HAR 3 form?
The HAR 3 form must be filled out by both a parent or guardian and a qualified health care provider. Parents or guardians begin by completing Part I, which includes vital health history questions specific to the child. This section requires information about allergies, past hospitalizations, and any medications the child may be taking. Subsequently, a licensed health care provider – which can include a physician, nurse practitioner, or physician assistant – must complete Part II by performing a physical exam and documenting their findings, ensuring that the child is fit for school and sports participation.
When is the HAR 3 form required?
What information is requested in Part I of the HAR 3 form?
Part I of the HAR 3 form seeks a broad range of information from parents or guardians. This includes basic details about the student, such as their name, birth date, and contact information. Crucially, it also requests responses to various health history questions that cover potential health concerns like allergies, past injuries, and any daily medications being taken. Parents are encouraged to answer thoroughly and explain any "yes" responses to provide a clear picture of the student’s health. This information supports health care providers in their assessments and allows school staff to accommodate any special health needs.
What happens if the HAR 3 form is not completed and submitted?
If the HAR 3 form is not completed and submitted, a student may face delays in starting school or may not be allowed to participate in school activities, including sports. Compliance with state law mandates the submission of this record, and schools take these regulations seriously to ensure the health and safety of all students. Parents should be proactive in completing and returning the form on time to avoid any interruptions in their child's education.
Common mistakes
Filling out the HAR 3 form can seem straightforward, but it is crucial that parents and guardians approach this process carefully. Mistakes can lead to complications regarding a child’s health records and school compliance. Here are five common errors to avoid when completing this important document.
One frequent mistake is incomplete information. Parents often overlook sections that require thorough responses, such as health history questions. It’s essential to provide detailed answers, especially to questions about allergies, past hospitalizations, and existing medical conditions. Omitting critical information can result in insufficient care during school hours and could prevent your child from being included in sports or extracurricular activities.
Another common error involves misunderstanding immunization requirements. The HAR 3 form mandates that children have specific immunizations completed before entering school. Parents sometimes confuse the requirements or fail to attach necessary immunization records. Ensuring that your child’s immunizations are up to date and that all documentation is included is vital to meet state regulations.
Additionally, failing to provide an accurate primary care provider's information is a mistake many make. This section must include correct contact details for the child’s healthcare provider. Being able to contact a provider quickly, especially in a medical emergency, is crucial. A wrong phone number or an outdated address could delay vital communication about your child's health.
An often-overlooked area is the actual signature and date. Parents may forget to sign the form or put the correct date on it, which can lead to it being considered invalid. This seemingly minor detail can lead to delays in processing the form within the school system.
Lastly, some parents forget to review the completed form before submission. Failing to double-check for errors, such as forgotten answers or misspellings, can result in misunderstandings and delays. Taking a moment to carefully review your responses can smooth the process and ensure that all information is accurate and complete.
By being mindful of these common pitfalls, parents can fill out the HAR 3 form with greater confidence, ensuring their child’s health needs are met efficiently and effectively.
Documents used along the form
When completing the HAR 3 form for health assessment in Connecticut schools, several related forms and documents often accompany it. These documents streamline the process of ensuring that students meet health requirements and receive the best care at school. Below is a list of commonly used forms along with a brief description of each.
- Immunization Record: This document details the vaccination history of the student. It must be filled out by the healthcare provider and includes required vaccines and the dates they were administered. This record is essential for confirming that a student has met the state vaccination requirements.
- Medication Authorization Form: Parents need to complete this form to authorize school personnel to administer prescribed medications during school hours. It requires signatures from both the parent and the child's healthcare provider.
- Emergency Contact Form: This form provides alternative contacts for the student in case of an emergency. It is crucial to ensure that someone is available to make decisions if parents cannot be reached.
- Sports Physical Examination Form: A specific form required for students participating in sports, it documents a physical examination conducted by a healthcare provider. It ensures that students are fit to participate in physical activities.
- Health Insurance Verification Form: This document confirms a student's health insurance coverage. It includes information about the provider and policy number, which is crucial for managing healthcare expenses incurred at school.
- Dental Health Assessment: Similar to the HAR 3 form, this assessment focuses on a child’s dental health. It usually requires a dental provider to complete and submit it to provide a comprehensive view of the student's health.
- Allergy Action Plan: This plan is vital for students with known allergies. It lays out how to handle allergic reactions, specifies triggers, and includes treatment options like the use of an EpiPen.
- Asthma Action Plan: This specialized document helps manage asthma symptoms and outlines steps to take during an asthma attack. Parents must provide this to ensure that school staff can respond appropriately in emergencies.
- 504 Plan (if applicable): This plan outlines accommodations for students with disabilities, ensuring they have equal access to education. It's tailored based on individual health or learning needs.
These forms collectively assist in creating a supportive and healthy educational environment for students in Connecticut. Ensuring that all necessary documents are properly filled out and submitted helps schools address the individual health needs of their students effectively.
Similar forms
- Health History Questionnaire: This document collects information about an individual’s medical history, current conditions, and any medications they may be taking. Like the HAR 3 form, it aims to establish a comprehensive health profile that can assist healthcare providers in delivering appropriate care.
- Immunization Records: These records document the immunizations a child has received. Similar to HAR 3, immunization records require detailed information about vaccines administered, which is essential for school enrollment and compliance with state health regulations.
- Authorization for Medication Administration: This document is used to grant permission for a student to receive medication during school hours. Such authorization parallels HAR 3 as both forms involve parental consent and the necessity for healthcare provider input for student health needs.
- Physical Exam Form: This document outlines the findings from a physical examination conducted by a healthcare provider. Like Part II of the HAR 3 form, it includes details about a student’s health status and may be used as a prerequisite for participation in school sports and extra-curricular activities.
- Emergency Health Information Form: This form provides vital health details that school officials can use in case of a medical emergency. It shares similarities with the HAR 3, as both forms aim to ensure that health care providers and school personnel have critical information necessary for responding to a child's health concerns effectively.
Dos and Don'ts
When filling out the HAR-3 form, there are specific practices to take into consideration to ensure completeness and accuracy. Below is a list of essential actions to undertake and pitfalls to avoid.
- Do: Provide complete and accurate information regarding your child's health history, including any relevant medical conditions.
- Do: Include emergency contact information, ensuring that it is up to date and accurate.
- Do: Sign the form where indicated to allow for communication between the school and healthcare providers.
- Do: Indicate if your child has any daily medications and provide necessary details.
- Don't: Leave any sections blank; incomplete forms may delay your child's enrollment process.
- Don't: Provide outdated or incorrect immunization records, as it may lead to issues with school attendance.
- Don't: Forget to explain any “yes” answers in the designated space, as this information is crucial for your child's health management.
- Don't: Submit the form without carefully reviewing it for errors or omissions that could affect processing.
Misconceptions
Misconceptions about the HAR 3 form can lead to confusion among parents, guardians, and students alike. Understanding the facts is crucial for ensuring that children's health needs are correctly addressed. Below are seven common misconceptions:
- It is optional to fill out the HAR 3 form. Many believe that submitting the HAR 3 is not mandatory when enrolling a child in school. However, completing this form is a state requirement in Connecticut and essential for understanding students' health needs.
- The HAR 3 form only concerns physical health. Some individuals think this form is solely focused on physical health. In reality, it also collects information on mental and emotional health, providing a comprehensive view of the child’s overall well-being.
- Only doctors can complete the medical evaluation section. There is a misconception that only physicians can fill out the medical evaluation part of the form. In fact, any legally qualified healthcare provider, including nurse practitioners and physician assistants, is permitted to complete it.
- Immunization records don’t need to be attached for the HAR 3. Many parents may assume that providing the HAR 3 form is sufficient. However, an updated immunization record must accompany the form to comply with state regulations.
- Health insurance information is not necessary. Some believe that including health insurance details is optional. However, this information helps to guide care decisions, making it an important part of the form.
- Completing the form guarantees my child will not need repeated assessments. While the HAR 3 form is important for initial enrollment, periodic health assessments, particularly during specific grade transitions, are still necessary as mandated by state law.
- The HAR 3 form only needs to be completed once. Another common misunderstanding is that the HAR 3 form only needs to be completed at the time of entry into school. In fact, updates may be required at various stages, especially if health circumstances change or during annual evaluations for sports participation.
Recognizing and addressing these misconceptions can help create a smoother process for students’ health assessments and pave the way for better educational experiences.
Key takeaways
When filling out the HAR-3 form, consider these essential points to ensure a smooth process regarding your child's health assessment.
- Complete All Sections: Take your time to fill out every part of the form, especially the health history questions in Part I. This information is crucial for school personnel and healthcare providers.
- Check Immunization Requirements: Be aware that Connecticut law mandates specific immunizations prior to school entrance. Ensure that your child’s immunization records are up to date and attached.
- Address Health Concerns: If your child has any health issues or concerns, it’s important to detail these in the provided sections. Clear communication helps school staff support your child effectively.
- Signature Matters: Don’t forget to sign and date the form. Your signature is necessary to authorize the release of your child's health information between the school and healthcare provider.
- Follow-Up Requirements: Remember that additional health assessments are required in certain grades, such as 6th and 9th. Keep track of these milestones to ensure compliance.
Overall, filling out the HAR-3 form is a straightforward but vital process. By paying attention to the details, you help create a safe and supportive educational environment for your child.
Browse Other Templates
Annual Activity Consent Form,Girl Scout Participation Approval,Troop Engagement Permission Slip,Comprehensive Parent Authorization,Yearly Scout Activity Release,All-in-One Girl Scout Consent Form,Troop Activity Agreement,Parent/Guardian Event Permiss - Activity fees may apply, and the responsibility for them lies with you as the parent.
North Carolina Driver License - The letter is part of the overall legal process aimed at reducing impaired driving incidents.