Fill Out Your Health Insurance Form
The Health Insurance Benefit Agreement is a crucial document in the landscape of healthcare provisions in the United States. It empowers providers to receive payments under Title XVIII of the Social Security Act, ensuring they comply with Federal regulations. Central to this agreement is the commitment by healthcare providers to adhere to important provisions that promote civil rights and protect individuals with disabilities, as established under the Civil Rights Act of 1964 and the Rehabilitation Act of 1973. This agreement must be signed by both the provider and the Secretary of Health and Human Services, establishing a binding relationship that persists even through changes in ownership of the service provider. A critical aspect of the form includes a cautionary note regarding the legal ramifications of falsifying any information, emphasizing the seriousness with which the government treats accuracy and honesty. The agreement encompasses numerous logistical elements, such as the identification of the parties involved, signatures from authorized individuals, and a description of the terms of acceptance. Furthermore, it incorporates a requirement for transparency regarding the time and effort needed to complete the form, adhering to the standards set out by the Paperwork Reduction Act of 1995. Understanding this form is vital for both service providers and beneficiaries, as it governs the operational framework of healthcare services and funding in America.
Health Insurance Example
DEPARTMENT OF HEALTH AND HUMAN SERVICES |
FORM APPROVED |
CENTERS FOR MEDICARE & MEDICAID SERVICES |
OMB No. |
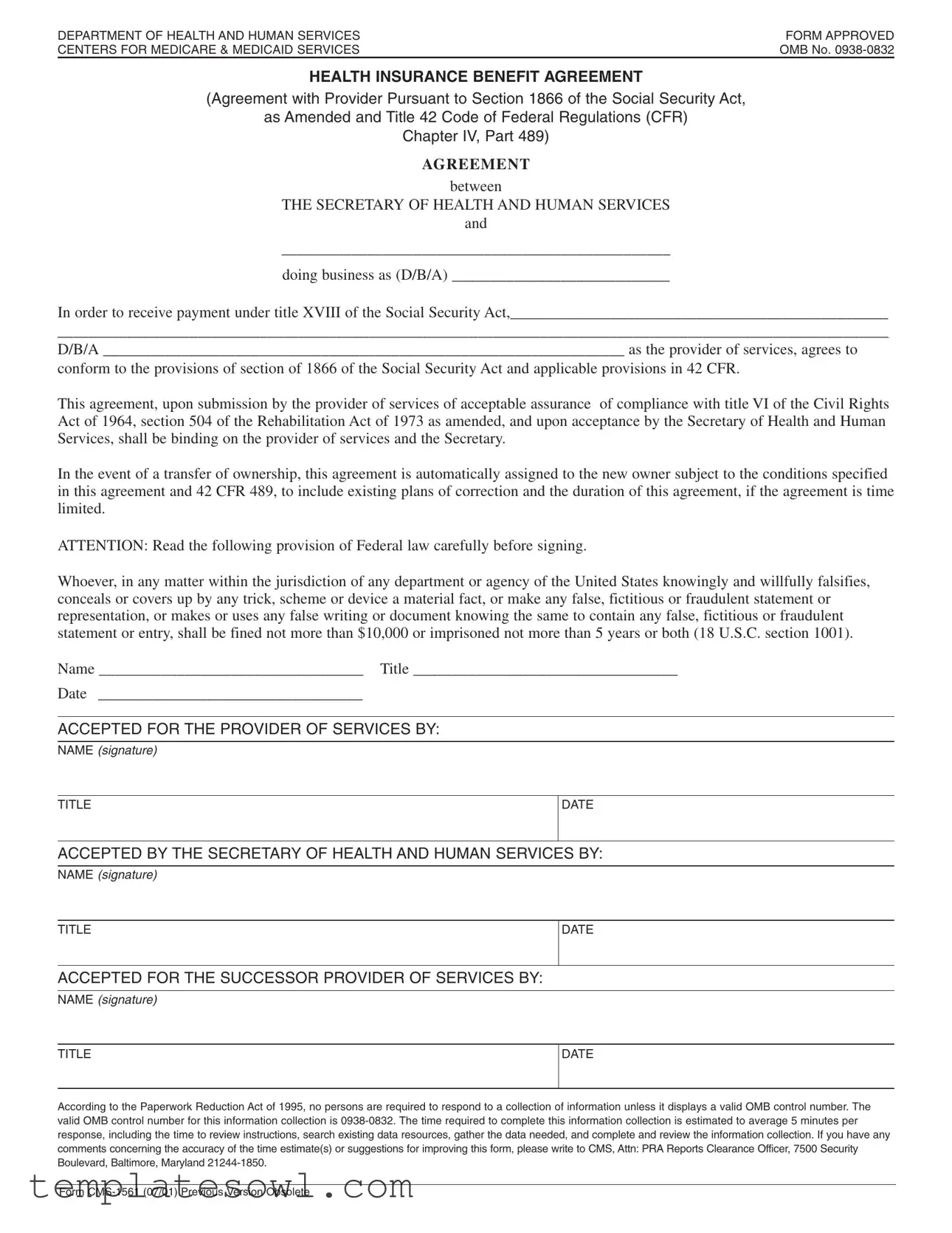
HEALTH INSURANCE BENEFIT AGREEMENT
(Agreement with Provider Pursuant to Section 1866 of the Social Security Act,
as Amended and Title 42 Code of Federal Regulations (CFR)
Chapter IV, Part 489)
AGRE E ME NT
between
THE SECRETARY OF HEALTH AND HUMAN SERVICES
and
__________________________________________________
doing business as (D/B/A) ____________________________
In order to receive payment under title XVIII of the Social Security Act,_________________________________________________
___________________________________________________________________________________________________________
D/B/A ___________________________________________________________________ as the provider of services, agrees to
conform to the provisions of section of 1866 of the Social Security Act and applicable provisions in 42 CFR.
This agreement, upon submission by the provider of services of acceptable assurance of compliance with title VI of the Civil Rights Act of 1964, section 504 of the Rehabilitation Act of 1973 as amended, and upon acceptance by the Secretary of Health and Human Services, shall be binding on the provider of services and the Secretary.
In the event of a transfer of ownership, this agreement is automatically assigned to the new owner subject to the conditions specified in this agreement and 42 CFR 489, to include existing plans of correction and the duration of this agreement, if the agreement is time limited.
ATTENTION: Read the following provision of Federal law carefully before signing.
Whoever, in any matter within the jurisdiction of any department or agency of the United States knowingly and willfully falsifies, conceals or covers up by any trick, scheme or device a material fact, or make any false, fictitious or fraudulent statement or representation, or makes or uses any false writing or document knowing the same to contain any false, fictitious or fraudulent statement or entry, shall be fined not more than $10,000 or imprisoned not more than 5 years or both (18 U.S.C. section 1001).
Name __________________________________ Title __________________________________
Date __________________________________
ACCEPTED FOR THE PROVIDER OF SERVICES BY:
NAME (signature)
TITLE
DATE
ACCEPTED BY THE SECRETARY OF HEALTH AND HUMAN SERVICES BY:
NAME (signature)
TITLE
DATE
ACCEPTED FOR THE SUCCESSOR PROVIDER OF SERVICES BY:
NAME (signature)
TITLE
DATE
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is
Form
Form Characteristics
| Fact Name | Details |
|---|---|
| Governing Law | This form is governed by Section 1866 of the Social Security Act and Title 42 Code of Federal Regulations (CFR) Chapter IV, Part 489. |
| Purpose | The form serves as a Health Insurance Benefit Agreement between the Secretary of Health and Human Services and the provider of services. |
| Compliance Requirement | Providers must comply with Title VI of the Civil Rights Act of 1964 and Section 504 of the Rehabilitation Act of 1973. |
| Transfer of Ownership | In case of a transfer of ownership, this agreement is automatically assigned to the new owner, with specific conditions. |
| Falsification Penalties | Willful falsification of information may lead to a fine of up to $10,000 or imprisonment for up to 5 years. |
| Signature Requirement | Both the provider and the Secretary of Health and Human Services must sign this agreement for it to be valid. |
| OMB Control Number | The valid OMB control number for this information collection is 0938-0832. |
| Estimated Completion Time | It is estimated to take about 5 minutes to complete this information collection. |
Guidelines on Utilizing Health Insurance
Filling out the Health Insurance Benefit Agreement form is an important step for providers to ensure they comply with regulations and receive payments appropriately. Carefully follow the steps below to complete the form accurately.
- Provide the name of the entity entering into the agreement in the designated space. Ensure that the full legal name is used.
- Fill in the "doing business as" (D/B/A) name, if applicable. This is the name under which services will be provided.
- Complete the section that includes the full address of the provider services organization.
- Read the Federal law provision about falsifying information carefully. Acknowledge your understanding.
- Enter your name in the section labeled "Name." This should be the person authorized to sign the agreement.
- Include the title of the individual signing the form in the provided space.
- Fill in the date when the agreement is being signed.
- Ensure that the area labeled "ACCEPTED FOR THE PROVIDER OF SERVICES BY" is signed by the authorized representative. Include the representative's name, title, and date next to the signature.
- Check that the "ACCEPTED BY THE SECRETARY OF HEALTH AND HUMAN SERVICES" section is left blank as this will be completed by the authorized personnel from the department.
- If applicable, fill out the section for acceptance by a successor provider of services. Include the name, title, and date for their authorized representative's signature.
Upon completion, ensure that all information is accurate and clear before submitting the form. Retain a copy of the signed agreement for your records.
What You Should Know About This Form
What is the Health Insurance Benefit Agreement?
The Health Insurance Benefit Agreement is a contract between the Secretary of Health and Human Services and service providers. It allows providers to receive payment under Title XVIII of the Social Security Act. This agreement requires providers to comply with specific federal regulations, ensuring that they meet quality and fairness standards in their services.
Who needs to fill out the Health Insurance form?
This form is typically filled out by healthcare providers who wish to participate in Medicare and receive payments for their services. If you are a provider wishing to establish a relationship with Medicare, this form is necessary to formalize that agreement.
What are the responsibilities of the provider under this agreement?
Providers must adhere to the provisions set forth in Section 1866 of the Social Security Act and applicable parts of the Code of Federal Regulations. This includes maintaining compliance with civil rights laws and demonstrating a commitment to providing equal access and non-discriminatory services.
What happens if the ownership of a provider changes?
If the ownership of a provider changes, the Health Insurance Benefit Agreement is automatically assigned to the new owner. However, specific conditions and existing plans of correction must still be honored under the original terms of the agreement. This ensures that quality standards are maintained even after ownership transfers.
What penalties exist for providing false information on this form?
Providing false or misleading information on the Health Insurance form can lead to severe penalties. This includes fines up to $10,000 and imprisonment for up to five years. It's essential to provide accurate data as any form of falsification can have serious legal consequences.
How long does it take to complete the form?
On average, it takes about five minutes to complete the Health Insurance Benefit Agreement. This estimate includes time spent reviewing the instructions, gathering necessary information, and completing the form itself. It is advisable to have all required documentation ready to streamline the process.
Where should I send my completed Health Insurance form?
The completed Health Insurance Benefit Agreement should be submitted to the Centers for Medicare & Medicaid Services (CMS). Specific mailing details or electronic submission guidelines may be detailed on the form or on the CMS website, so checking for the latest updates is recommended to ensure proper submission.
Common mistakes
Filling out the Health Insurance Benefit Agreement can be a straightforward process, but several common mistakes can lead to complications. Understanding these pitfalls can help ensure the form is completed accurately and efficiently.
One frequent error is incomplete information. Individuals often overlook sections such as the name or title of the provider, which can delay processing. Ensure every required field is filled out completely to avoid unnecessary back-and-forth communication.
Another mistake involves illegible handwriting. If the form is filled out by hand, it's important to write clearly. Illegible entries can lead to misunderstandings regarding the provider's information. In many cases, typing the form or using an online submission method can prevent this issue.
The third common mistake is incorrect dates. Applicants sometimes forget to enter accurate dates, especially on signatures. This can undermine the validity of the agreement. Always double-check that the dates correspond with the signing and submission of the form.
Additionally, some individuals fail to read the fine print. Ignoring the legal implications of the form can result in unintentional violations. A careful review of all provisions helps ensure compliance with the regulations from the outset.
Providing misleading or false information constitutes another critical error. Deliberately or accidentally misrepresenting facts can lead to severe legal consequences. Hence, it is vital to ensure all entries are truthful and accurately reflect the provider's situation.
Lastly, neglecting to gather supporting documents is a mistake many encounter. Certain applications require additional information or confirmations. Collecting and attaching these documents ahead of time facilitates a smoother review process.
By avoiding these mistakes, applicants can enhance the accuracy and efficiency of their submissions. Careful attention to detail is essential to ensure that the Health Insurance Benefit Agreement is processed without delays or complications.
Documents used along the form
When dealing with health insurance, several other forms and documents can often accompany the main Health Insurance Benefit Agreement. These documents help facilitate an efficient process for obtaining and providing medical services. Below is a list of related forms that you may encounter.
- Health Insurance Claim Form: A form used to request payment from an insurance provider for healthcare services rendered. It includes details about the patient, provider, and services provided.
- Authorization for Release of Information: This document allows healthcare providers to share a patient’s medical records with the insurance company, ensuring that claims can be processed without delay.
- Enrollment Form: This form is used by individuals to enroll in a health insurance plan. It collects personal information and selections about coverage options.
- Provider Agreement: A contract between a healthcare provider and the insurance company that outlines the terms of service, payment, and obligations of both parties.
- Medical Necessity Form: A document that justifies the need for specific services or treatments, often required by insurance companies to approve claims.
- Continuity of Care Form: This form allows patients to maintain their care with a specific provider while ensuring that the insurance policies align, especially during transitions between plans.
- Supplemental Insurance Application: This application is filled out to request additional coverage, which can help cover out-of-pocket costs that the primary insurance does not pay.
- Summary of Benefits and Coverage (SBC): An informative document that provides a clear summary of what an insurance plan covers, including costs, limits, and coverage specifics.
Understanding and having these documents prepared can streamline the interactions between patients, providers, and insurance companies. They play an important role in ensuring compliance, processing claims, and ultimately providing patients with the care they need.
Similar forms
- Health Care Services Agreement: Similar to the Health Insurance form, this document establishes a formal relationship between a healthcare provider and a patient or insurance company, outlining the terms, responsibilities, and expected deliverables of the service provision.
- Provider Enrollment Form: This form is used by healthcare providers to enroll in a health insurance plan. Like the Health Insurance form, it collects key information that defines the provider's qualifications and compliance with regulations.
- Release of Information Form: This document allows healthcare providers to share patient information with third parties. It resembles the Health Insurance form in that both require consent and adherence to privacy laws under the Health Insurance Portability and Accountability Act (HIPAA).
- Claim Submission Form: This form is essential for billing and collecting payment for services rendered. It shares similarities with the Health Insurance form as it documents the provider’s agreement to accept payment conditions while ensuring compliance with insurance rules.
- Patient Consent Form: Aimed at securing patient approval for treatment, this form is like the Health Insurance form in that both articulate rights, responsibilities, and legal implications attached to healthcare services.
- Durable Power of Attorney for Health Care: This legal document allows individuals to designate someone to make health care decisions on their behalf. Its point of focus on compliance with healthcare regulations parallels the obligations set forth in the Health Insurance form.
- Advanced Beneficiary Notice of Noncoverage (ABN): This form informs patients of services that may not be covered by Medicare, similar to the Health Insurance form due to its role in outlining provider responsibilities and service conditions.
Dos and Don'ts
When filling out the Health Insurance form, it is important to follow certain guidelines to ensure accuracy and compliance. Below is a list of things to do and avoid.
- Do read all instructions carefully before completing the form.
- Do provide accurate information about the provider's name and contact details.
- Do check all entries for errors before submitting the form.
- Do sign and date the form where indicated.
- Do keep a copy of the completed form for your records.
- Don’t leave any required fields blank.
- Don’t use unclear abbreviations or jargon that could be misinterpreted.
- Don’t provide false or misleading information under any circumstances.
- Don’t forget to review the submission guidelines for delivery of the form.
Misconceptions
Understanding health insurance forms can be challenging, and several misconceptions often arise. Here are five common misunderstandings about the Health Insurance Benefit Agreement:
- This form is just a contract. Many believe that the form serves only as a legal contract, but it's more than that. It establishes compliance with specific regulations of the Social Security Act and outlines the terms under which services will be reimbursed.
- Completion guarantees payment. Some assume that merely filling out the form ensures payment for their services. However, payment is contingent upon acceptance by the Secretary of Health and Human Services and adherence to various compliance standards.
- The form is the same for all providers. This misconception is misleading. While the general structure may be similar, details such as provider-specific agreements or conditions can vary significantly based on location and type of services provided.
- Once signed, it cannot change. It’s commonly thought that the agreement is set in stone post-signature. However, changes can occur, especially in the case of ownership transfer, where the agreement may be automatically assigned under certain conditions.
- Paperwork is a one-time task. Many assume that submitting this form is a one-time effort. In reality, providers may need to revisit and update their submissions as regulations evolve or as their own business circumstances change.
It is important to approach these forms with a clear understanding of their purpose and implications. Misunderstandings can lead to compliance issues or payment delays.
Key takeaways
Understanding the Health Insurance form is essential for service providers aiming to receive payment under Medicare. Here are some key takeaways to consider:
- Accurate Information is Crucial: Ensure that all fields are filled out accurately, including the provider's name and title. Inaccuracies can delay payment or lead to complications down the line.
- Compliance is Mandatory: Familiarize yourself with the provisions of the Social Security Act and the relevant parts of the Code of Federal Regulations. Compliance with these regulations is necessary to maintain your ability to receive reimbursements.
- Signature Requirement: The form must be signed by both the provider and the Secretary of Health and Human Services to be valid. This step is vital for the agreement to take effect.
- Understand the Consequences: Be aware that falsifying information on the form can lead to serious consequences, including fines or imprisonment. Always provide truthful and transparent information.
Completing the Health Insurance form correctly and understanding your obligations can pave the way for smoother transactions and fewer headaches in the future. Stay informed and diligent to ensure compliance and reliability in your services.
Browse Other Templates
Movers Contract Template - It details moving charges based on hourly rates and travel fees.
Hdfc Form - The form serves as an official record of your intent to dispute specific transactions.
West Virginia 2019 S-Corp Partnership Tax Form,WV Pass-Through Entity Tax Document 2019,S Corporation and Partnership Tax Filing 2019,WV Income Tax Return for Pass-Through Entities,2019 West Virginia S-Corporation and Partnership Return,WV Tax Form S - The form requires a state of domicile to be indicated.