Fill Out Your Ia 1 Form
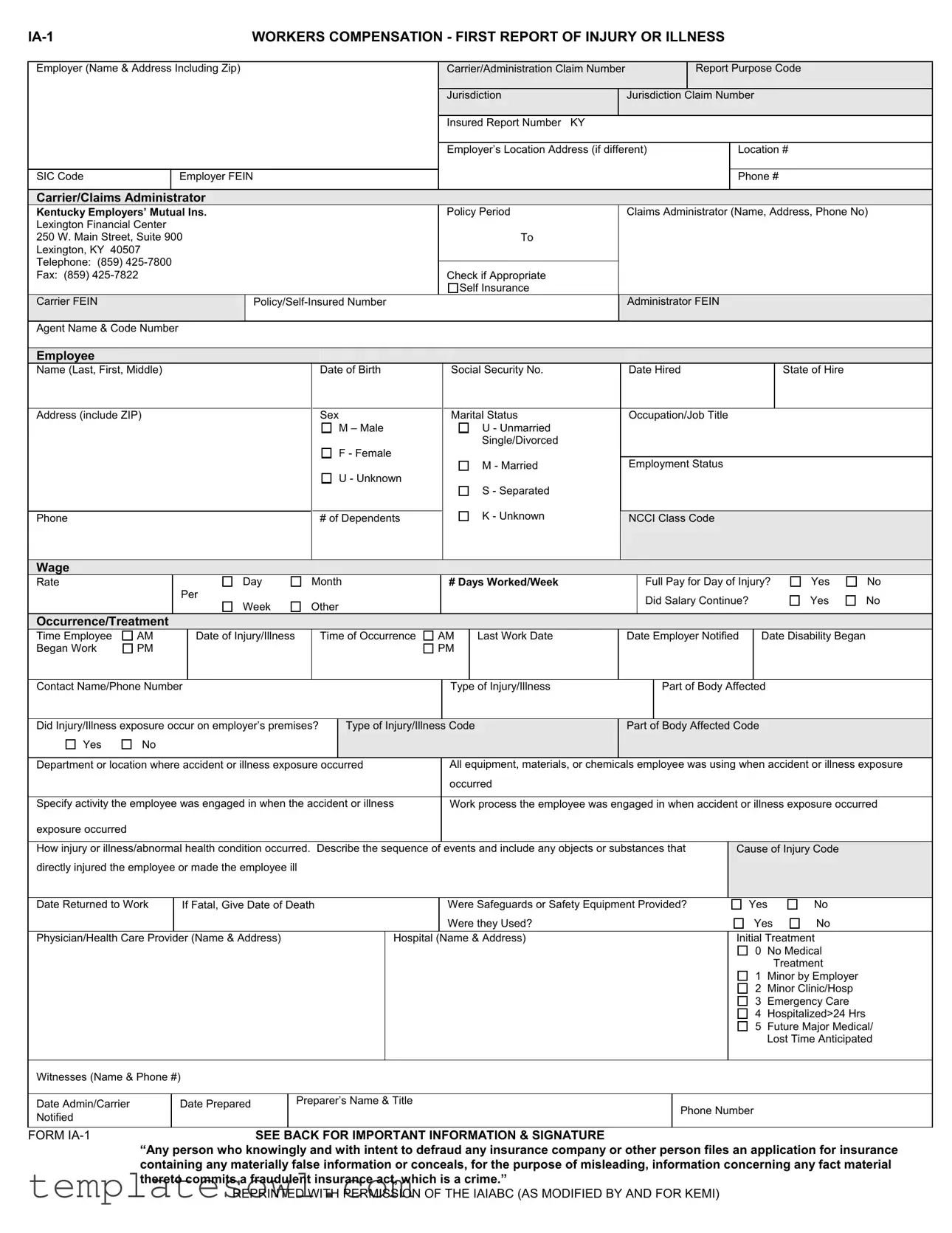
The IA-1 form is essential for reporting workplace injuries and illnesses. It serves a crucial role in ensuring that both employees and employers properly document incidents that occur on the job. Key segments of the form require clear information from the employer, including their name, contact details, and relevant insurance carrier information. The employee’s personal information—like name, date of birth, and job title—is also necessary. Details about the injury or illness, including the date it occurred, time, and specifics about the injury, such as the body part affected, are critical for accurate reporting. Employers must also indicate whether the injury happened on their premises and describe the circumstances surrounding the incident. Additional sections pertain to the type of medical treatment received and any witnesses present during the occurrence. Understanding the importance of each section can streamline the claims process, ensuring efficient management of worker's compensation claims and supporting the employee’s recovery while fulfilling their rights under workplace safety regulations.
Ia 1 Example
|
|
|
|
|
WORKERS COMPENSATION - FIRST REPORT OF INJURY OR ILLNESS |
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Employer (Name & Address Including Zip) |
|
|
|
|
|
Carrier/Administration Claim Number |
|
|
|
|
|
Report Purpose Code |
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Jurisdiction |
Jurisdiction Claim Number |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insured Report Number KY |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer’s Location Address (if different) |
Location # |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIC Code |
|
|
Employer FEIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone # |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Carrier/Claims Administrator |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Kentucky Employers’ Mutual Ins. |
|
|
|
|
|
Policy Period |
Claims Administrator (Name, Address, Phone No) |
||||||||||||||||||||
|
Lexington Financial Center |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
250 W. Main Street, Suite 900 |
|
|
|
|
|
|
|
To |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Lexington, KY 40507 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Telephone: (859) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Fax: (859) |
|
|
|
|
|
|
|
|
|
|
Check if Appropriate |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Self Insurance |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Carrier FEIN |
|
|
|
|
|
|
|
|
Administrator FEIN |
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Agent Name & Code Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employee |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name (Last, First, Middle) |
|
|
|
|
|
|
|
Date of Birth |
Social Security No. |
Date Hired |
|
|
|
State of Hire |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Address (include ZIP) |
|
|
|
|
|
|
|
Sex |
Marital Status |
Occupation/Job Title |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
M – Male |
|
|
U - Unmarried |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Single/Divorced |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F - Female |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M - Married |
Employment Status |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
U - Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S - Separated |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Phone |
|
|
|
|
|
|
|
|
|
# of Dependents |
|
|
K - Unknown |
NCCI Class Code |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Wage |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rate |
|
|
|
|
Day |
|
Month |
# Days Worked/Week |
|
Full Pay for Day of Injury? |
Yes |
No |
|||||||||||||||
|
|
|
|
Per |
|
|
|
|
|
|
|
|
|
Did Salary Continue? |
|
|
|
Yes |
No |
|||||||||
|
|
|
|
|
|
Week |
|
Other |
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Occurrence/Treatment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Time Employee |
AM |
|
Date of Injury/Illness |
|
|
Time of Occurrence |
AM |
|
Last Work Date |
Date Employer Notified |
Date Disability Began |
|
|||||||||||||||
|
Began Work |
PM |
|
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Contact Name/Phone Number |
|
|
|
|
|
Type of Injury/Illness |
|
|
Part of Body Affected |
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
Did Injury/Illness exposure occur on employer’s premises? |
|
Type of Injury/Illness Code |
Part of Body Affected Code |
|
|
|
|
||||||||||||||||||||
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
Department or location where accident or illness exposure occurred |
All equipment, materials, or chemicals employee was using when accident or illness exposure |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
occurred |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
Specify activity the employee was engaged in when the accident or illness |
Work process the employee was engaged in when accident or illness exposure occurred |
||||||||||||||||||||||||||
|
exposure occurred |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
How injury or illness/abnormal health condition occurred. Describe the sequence of events and include any objects or substances that |
Cause of Injury Code |
|
|||||||||||||||||||||||||
|
directly injured the employee or made the employee ill |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
Date Returned to Work |
|
If Fatal, Give Date of Death |
|
|
|
Were Safeguards or Safety Equipment Provided? |
Yes |
|
|
No |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Were they Used? |
|
|
|
|
|
|
|
Yes |
No |
|
||||
|
Physician/Health Care Provider (Name & Address) |
|
|
|
|
Hospital (Name & Address) |
|
|
|
|
|
|
Initial Treatment |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 No Medical |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treatment |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 Minor by Employer |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
Minor Clinic/Hosp |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 Emergency Care |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
Hospitalized>24 Hrs |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
Future Major Medical/ |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lost Time Anticipated |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Witnesses (Name & Phone #) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Date Admin/Carrier |
|
|
Date Prepared |
|
Preparer’s Name & Title |
|
|
|
|
|
|
|
Phone Number |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Notified |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
FORM |
|
|
|
|
|
SEE BACK FOR IMPORTANT INFORMATION & SIGNATURE |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
“Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance |
||||||||||||||||||||||||||
containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime.”
REPRINTED WITH PERMISSION OF THE IAIABC (AS MODIFIED BY AND FOR KEMI)

EMPLOYER’S INSTRUCTIONS
DO NOT ENTER DATA IN SHADED FIELDS
DATES:
Enter all dates in MM/DD/YY.
SIC CODE:
This is the code that represents the nature of the employer’s business that is contained in the Standard Industrial Classification Manual published by the Federal Office of Management and Budget.
CARRIER:
The licensed business entity issuing a contract of insurance and assuming financial responsibility on behalf of the employer or the claimant.
CLAIMS ADMINISTRATOR:
Enter the name of the carrier, third party administrator, state fund, or
AGENT NAME & CODE NUMBER:
Enter the name of your insurance agent and his/her code number if known. This information can be found on your insurance policy.
OCCUPATION/JOB TITLE:
This is the primary occupation of the claimant at the time of the accident or exposure.
EMPLOYMENT STATUS:
Indicate the employee’s work status. The valid choices are:
DATE DISABILITY BEGAN:
The first day on which the claimant originally lost time from work due to the occupational injury or disease or as otherwise designated by the statute.
CONTACT NAME/PHONE NUMBER:
Enter the name of the individual at the employer’s premises to be contacted for additional information.
TYPE OF INJURY/ILLNESS:
Briefly describe the nature of the injury or illness, (e.g. Lacerations to the forearm).
PART OF BODY AFFECTED:
Indicate the part of body affected by the injury/illness, (e.g. Right forearm, lower back).
DEPARTMENT OR LOCATION WHERE ACCIDENT OR ILLNESS EXPOSURE OCCURRED:
(e.g. Maintenance Department or Client’s office at 452 Monroe St., Washington, DC 26210) If the accident or illness exposure did not occur on the employer’s premises, enter the address or location. Be specific.
ALL EQUIPMENT, MATERIAL OR CHEMICALS EMPLOYEE WAS USING WHEN ACCIDENT OR ILLNESS EXPOSRE OCCURRED:
(e.g., Acetylene cutting torch, metal plate)
List all equipment, materials and/or chemicals the employee was using, applying, handling or operating when the injury or illness occurred. Be specific, for example: decorator’s scaffolding, electric sander, paintbrush, and paint.
Enter “NA” for not applicable if no equipment, materials or chemicals were being used. NOTE: The items listed do not have to be directly involved in the employee’s injury or illness.
SPECIFIC ACTIVITY THE EMPLOYEE WAS ENGAGED IN WHEN THE ACCIDENT OR ILLNESS EXPOSURE OCCURRED:
(e.g., Cutting metal plate for flooring)
Describe the specific activity the employee was engaged in when the accident or illness exposure occurred, such as sanding ceiling woodwork in preparation of painting.
WORK PROCESS THE EMPLOYEE WAS ENGAGED IN WHEN ACCIDENT OR ILLNESS EXPOSURE OCCURRED:
Describe the work process the employee was engaged in when the accident or illness exposure occurred, such as building maintenance. Enter “NA” for not applicable if employee was not engaged in a work process (e.g., walking along a hallway).
HOW INJURY OR ILLNESS/ABNORMAL HEALTH CONDITION OCCURRED. DESCRIBE THE SEQUENCE OF EVENTS AND INCLUDE ANY OBJECTS OR SUBSTANCES THAT DIRECTLY INJURED THE EMPLOYEE OR MADE THE EMPLOYEE ILL:
(Worker stepped back to inspect work and slipped on some scrap metal. As worker fell, worker brushed against the hot metal.)
Describe how the injury or illness/abnormal health condition occurred. Include the sequence of events and name any objects or substance that directly injured the employee or made the employee ill. For example: Worker stepped to the edge of the scaffolding to inspect work, lost balance and fell six feet to the floor. The worker’s right wrist was broken in the fall.
DATE RETURN(ED) TO WORK:
Enter the date following the most recent disability period on which the employee returned to work.
“Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime.”
Employee Signature: |
|
DATE: |
|
REPRINTED WITH PERMISSION OF THE IAIABC (AS MODIFIED BY AND FOR KEMI) |
|
Form Characteristics
| Fact Name | Details |
|---|---|
| Form Purpose | The IA-1 form is used to report an employee's injury or illness to ensure proper compensation claims are filed. |
| Governing Law | This form adheres to the Kentucky Workers' Compensation Act, which includes regulations surrounding workplace injuries. |
| Submission Timing | The employer must submit this report promptly after being notified of the injury or illness to comply with state regulations. |
| Information Required | The form requires details about the employee, the nature of the injury, and the circumstances surrounding the incident. |
| Medical Treatment Options | Sections of the form allow employers to indicate whether medical treatment was provided and what type it was (e.g., emergency care). |
| Fraud Warning | A notice emphasizes that knowingly providing false information on this form constitutes a fraudulent act. |
| Follow-Up Requirements | The employer is responsible for keeping track of the employee’s return to work date and report it appropriately in the form. |
Guidelines on Utilizing Ia 1
Completing the IA-1 form is an essential step after a workplace injury or illness. This process requires careful attention to detail to ensure that all necessary information is provided accurately. Following these steps will help in filling out the form correctly and efficiently.
- Gather necessary information: Collect details about the employer, the employee, and the incident. This includes names, addresses, dates, and descriptions of the injury or illness.
- Complete employer information: Fill in the employer's name and address, including zip code. Include the carrier or claims administrator’s details and the claim numbers.
- Fill out employee information: Enter the employee's name (last, first, middle), date of birth, Social Security number, and the address with zip code. Indicate the employee's marital status and occupation or job title.
- Injury or illness details: Record the date and time of the injury or illness, last work date, and the date the employer was notified. Specify the type of injury or illness and part of the body affected.
- Describe the circumstances: Detail the sequence of events that led to the injury or illness. Include specific activities, equipment, and materials involved.
- Provide treatment information: Indicate whether medical treatment was received and the type of treatment provided. Include the name and address of any healthcare providers involved.
- Complete other details: Fill in the questions regarding safeguards and safety equipment, names of witnesses, and dates related to the disability.
- Sign and date the form: Ensure that the employee signs and dates the form to acknowledge the information provided is accurate.
Once you have completed these steps, review the entire form to confirm that all sections are filled in correctly. Submit the IA-1 form according to your employer’s guidelines or the instructions provided by the claims administrator. Correct and timely submission is crucial for processing the claim efficiently.
What You Should Know About This Form
What is the IA-1 form used for?
The IA-1 form is the First Report of Injury or Illness, primarily used for workers' compensation claims. It helps employers report an injury or illness that occurs in the workplace to the insurance carrier or claims administrator.
Who needs to fill out the IA-1 form?
The employer is responsible for completing the IA-1 form. They provide details about the incident, the employee involved, and any medical treatment that may be necessary.
What information is required on the IA-1 form?
Key information includes the employer's name and address, employee details (like name, date of birth, and occupation), the nature of the injury or illness, and any medical treatment received. Specific dates related to the injury or illness must also be included.
When should the IA-1 form be submitted?
The IA-1 form should be completed and submitted as soon as possible after an injury or illness occurs. Prompt reporting helps ensure a smoother claims process and quicker access to necessary benefits.
Are there any fields on the IA-1 form that should not be filled out?
Yes, certain sections are designated as shaded fields and should not be filled out. It is crucial to follow the instructions provided carefully to avoid errors.
What happens if the IA-1 form is filled out incorrectly?
Filling out the IA-1 form incorrectly can delay the claims process. If there are mistakes, the claims administrator may request corrections, which can prolong the time it takes for benefits to be issued.
Is there a deadline for submitting the IA-1 form?
While there is no specific federal deadline, it is best to submit the IA-1 form as soon as possible after the injury or illness occurs. Each state may have its own regulations regarding timely reporting, so it's important to be aware of local rules.
How does the IA-1 form affect workers' compensation claims?
The IA-1 form serves as the official record for the injury or illness. It provides essential details that will be reviewed by the insurance carrier when processing a workers' compensation claim. Accurate and complete information can help facilitate a smoother claims process.
What can I do if I have more questions about the IA-1 form?
If you have questions about completing the IA-1 form, it’s best to reach out to your employer or a representative from your insurance carrier. They can provide guidance and ensure that you have all the necessary information.
What does the fraud warning on the IA-1 form mean?
The fraud warning indicates that providing false information on the form with the intent to deceive is illegal. It is important to ensure that all information submitted is truthful and accurate to avoid legal consequences.
Common mistakes
Completing the IA-1 form accurately is crucial for ensuring that an employee receives the necessary workers' compensation benefits. However, several common mistakes can complicate this process. Understanding these errors may help individuals avoid unnecessary delays or claims denials.
One frequent mistake is failing to provide complete employer details. This section includes the employer's name, address, and other identifying information. Omitting any of these can result in confusion and may hinder claim processing. Ensure that every specification is complete and correct to facilitate swift communication between all parties involved.
Another common error is entering incorrect dates. Whether it's the date of the incident or the date the employer was notified, precision is essential. Using the format MM/DD/YY is a must. Mistakes in dates may lead to misunderstandings about the timeline of the event, potentially affecting the claim's validity.
People often overlook the type of injury or illness and the specific parts of the body affected. Providing vague descriptions can create ambiguity in the claim. Detailed accounts help the claims administrator understand the severity and nature of the injury, thereby ensuring proper evaluation and compensation.
Employment status is another area where people make mistakes. Selecting the incorrect status can lead to discrepancies, which may affect benefit eligibility. It's important to choose the most accurate depiction of the employee’s work situation at the time of the incident, as multiple employment statuses exist, such as full-time, part-time, or seasonal.
In addition, individuals frequently neglect to list all equipment and materials involved in the incident. Completing this section thoroughly can prove essential. This information can significantly aid in comprehending the incident's context and assessing any potential employer liability.
The section requesting a description of how the injury occurred often suffers from lack of detail. Claimants sometimes provide overly general statements, which do not fully capture the events leading up to the injury. A clear and comprehensive account of the sequence of events can prevent complications later in the claims process.
Lastly, failing to include witness information is a critical mistake. Providing witness names and contact details can be invaluable in corroborating the incident. Witnesses can provide additional insights or details about the event that may support the employee's claim.
Taking the time to carefully review and complete each section of the IA-1 form can significantly impact the successful processing of a workers' compensation claim. By avoiding these common mistakes, employees enhance their chances of a smoother claims process.
Documents used along the form
The IA-1 form, or Workers Compensation - First Report of Injury or Illness, is a critical document in the reporting of workplace injuries and illnesses. Alongside this form, several other documents may be necessary to complete the reporting and claims process effectively. Below is a list of common forms and documents that are often used in conjunction with the IA-1 form.
- Employee Incident Report: This report is often filled out by the employee to provide a detailed account of the incident that led to the injury or illness. It includes information about the circumstances of the accident, any witnesses present, and the sequence of events leading to the injury.
- Physician's Report: This document is completed by the treating physician. It outlines the nature of the injury, recommended treatment, and the employee's ability to return to work. It plays a significant role in determining the worker's compensation benefits.
- Employer's Accident Investigation Report: Conducted by the employer, this report investigates the causes of the accident. It details the findings and any corrective actions taken to prevent future incidents, showcasing the employer's commitment to workplace safety.
- Claim Form (e.g., Form WC-1): This is a specific claim form submitted to the insurance carrier, detailing the employee's information, the nature of the claim, and other relevant data. It serves as the official request for workers' compensation benefits.
- Return to Work Release: Upon recovery, a physician issues this document, indicating that the employee is fit to return to work. It may specify any restrictions or accommodations that should be considered upon the employee's return.
- Earned Wage Statements: These documents outline the employee's wage history, which may be required to calculate compensation benefits. It helps verify the employee's earnings prior to the date of injury.
- Additional Medical Records: Depending on the severity of the injury, comprehensive medical records may be requested to support the claim. This can include past medical histories, treatment plans, and any necessary future medical care.
- Witness Statements: Statements from coworkers or witnesses provide critical accounts of the accident. These documents can help corroborate the employee's report and offer additional context regarding the event.
These forms and documents each play a vital role in the claims process for workers' compensation. Together, they create a comprehensive narrative of the incident, facilitate communication among involved parties, and ensure that injured workers receive the benefits and support they need.
Similar forms
- First Report of Injury (FROI): This document serves a similar purpose in reporting workplace injuries or illnesses. It includes essential information about the injured employee, the nature of the incident, and the date it occurred.
- Claim Form: Used to initiate a claim for workers' compensation benefits. Like the IA-1 form, it captures details about the employee, the injury, and relevant employer information.
- Incident Report: Created to document the specifics of an incident in the workplace. This report shares similarities in detailing the events leading to an injury or illness.
- Medical Report: This document reviews the medical aspects of an injury, providing a diagnosis and treatment details. It’s closely related to the IA-1 form, which also assesses the nature and extent of the injury.
- Employer's Report of Injury: Specifically required by some state regulations, this report outlines the employer's perspective on a workplace incident. It parallels the IA-1 form in gathering information about the event and its aftermath.
- Safety Incident Analysis: A document that identifies the causes and preventive measures for incidents. It shares the IA-1 form’s focus on understanding how and why injuries occur in the workplace.
Dos and Don'ts
When filling out the IA-1 form, there are several important considerations to keep in mind. Here is a list of things you should and shouldn't do:
- Do ensure accuracy. Double-check all entries for typos or mistakes, as errors can lead to delays or denials.
- Do specify job details clearly. Provide detailed descriptions of injuries, job titles, and activities to avoid confusion.
- Do seek assistance if needed. If unsure about any section, consult your supervisor or the claims administrator for guidance.
- Do keep copies of the completed form. Retaining a copy for your records can be beneficial for future reference.
- Don't leave fields blank. Fill in all required sections to ensure the form is complete.
- Don't provide vague descriptions. Lack of detail can complicate the claims process.
- Don't forget to check the shaded fields. Data should not be entered in specified shaded areas.
- Don't delay submission. Promptly submitting the form helps ensure that the claim is processed as quickly as possible.
Misconceptions
Common misconceptions about the IA-1 form can lead to errors and confusion. Here’s a list of those misconceptions explained:
- The IA-1 form is only for serious injuries. Many believe this form is only necessary for severe workplace injuries. However, any injury or illness, regardless of severity, should be reported using the IA-1 form.
- Filing the form is optional. Some people think submitting the IA-1 is voluntary. In reality, it is a required document for reporting workplace injuries and illnesses to ensure compliance with state laws.
- The employer is the only one responsible for completing the form. While employers typically fill out the IA-1, employees must provide accurate details about their injuries and illnesses to ensure the report is correct.
- Delays in reporting do not matter. Many workers believe they can wait to report their injury or illness. Timely reporting is crucial, as delays can affect benefits and claim approval.
- Only physical injuries need to be reported. Some individuals think that only visible injuries are reportable. Mental health issues and illnesses related to work exposure should also be documented.
- Every employee must submit their own IA-1 form. There’s a misconception that each injured worker needs to file separate forms. Instead, the employer typically handles this process for all incidents.
- Once submitted, the form cannot be amended. People often believe that the IA-1 is final. Corrections can be made if additional information or corrections arise after submission.
- The IA-1 form is only for workers covered by workers' compensation insurance. Some assume only insured workers need to report. However, all workplace injuries or illnesses should be documented, even for self-insured cases.
- All injuries must result in lost time from work to be reported. Some employees think that only injuries causing them to miss work require filing. In truth, every injury or illness should be reported, even if it does not lead to time off.
- Reporting an injury could lead to job loss. Fear of retaliation stops some employees from reporting injuries. In fact, it is illegal for employers to discriminate against employees who report workplace injuries.
Understanding these misconceptions can help ensure that injuries and illnesses are properly documented, leading to better outcomes for affected workers.
Key takeaways
1. Accurate Information is Essential: Ensure that all sections of the IA-1 form are filled out accurately. This includes the employer's details, employee information, and specifics about the injury or illness.
2. Clarity on Injury Details: Clearly describe the type of injury or illness and the part of the body affected. A detailed account will help in processing the claim efficiently.
3. Notify Relevant Parties Promptly: Keep in mind that the employer and the insurance carrier must be notified in a timely manner regarding any incidents. This helps in ensuring that the employee receives timely assistance and support.
4. Use a Clear Contact Person: Designate a specific contact person within your organization for any follow-up regarding the claim. Include their name and phone number on the form to facilitate direct communication.
Browse Other Templates
Notice of Related Cases California - Multiple related cases can be detailed within the same form if necessary.
Ex Parte Notice Declaration,Temporary Restraining Order Notice,Family Law Ex Parte Notice,Application for Emergency Hearing,Declaration of Notice for Ex Parte Application,Notice of Hearing Declaration,Ex Parte Petition Notice,Urgent Application Notif - It is a vital part of the court record concerning ex parte applications in family law.