Fill Out Your L 1124 Form
The L 1124 form is a critical component of the physician licensure process in Texas, specifically designed for evaluating an applicant's postgraduate training and professional history. This form plays an essential role in verifying the qualifications of medical professionals seeking licensure by the Texas Medical Board. Applicants must provide a wealth of information, including their current personal details, educational affiliations from the past five years, and consent for the release of pertinent information. The form mandates evaluations from every medical facility with which the applicant has been associated, reinforcing the importance of comprehensive feedback. Evaluating physicians, holding authoritative positions such as Chief of Staff or Department Chairman, are required to complete the associated sections, ensuring the authenticity and reliability of the assessments. The completed evaluation must be submitted directly to the Texas Medical Board through specified channels—email, mail, or fax—to maintain confidentiality and compliance with reporting standards. Both the applicant's and evaluating physician's responsibilities are clearly delineated, making this form an indispensable step in the journey to obtaining a medical license in Texas.
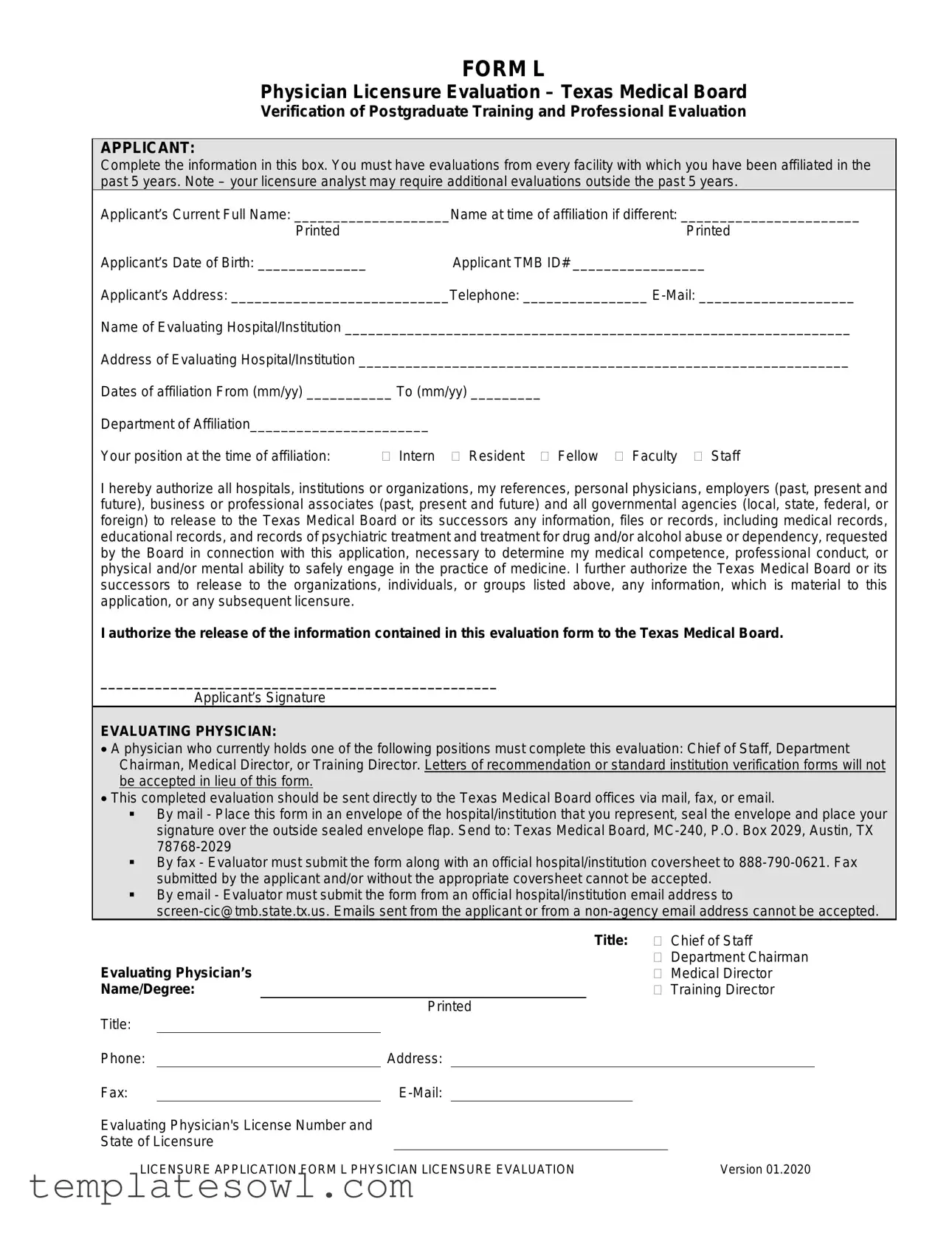
L 1124 Example
FORM L
Physician Licensure Evaluation – Texas Medical Board
Verification of Postgraduate Training and Professional Evaluation
APPLICANT:
Complete the information in this box. You must have evaluations from every facility with which you have been affiliated in the past 5 years. Note – your licensure analyst may require additional evaluations outside the past 5 years.
Applicant’s Current Full Name: ____________________Name at time of affiliation if different: _______________________
Printed |
Printed |
Applicant’s Date of Birth: ______________ |
Applicant TMB ID# _________________ |
Applicant’s Address: ____________________________Telephone: ________________
Name of Evaluating Hospital/Institution _________________________________________________________________
Address of Evaluating Hospital/Institution _______________________________________________________________
Dates of affiliation From (mm/yy) ___________ To (mm/yy) _________
Department of Affiliation_______________________
Your position at the time of affiliation: |
Intern Resident Fellow Faculty Staff |
I hereby authorize all hospitals, institutions or organizations, my references, personal physicians, employers (past, present and future), business or professional associates (past, present and future) and all governmental agencies (local, state, federal, or foreign) to release to the Texas Medical Board or its successors any information, files or records, including medical records, educational records, and records of psychiatric treatment and treatment for drug and/or alcohol abuse or dependency, requested by the Board in connection with this application, necessary to determine my medical competence, professional conduct, or physical and/or mental ability to safely engage in the practice of medicine. I further authorize the Texas Medical Board or its successors to release to the organizations, individuals, or groups listed above, any information, which is material to this application, or any subsequent licensure.
I authorize the release of the information contained in this evaluation form to the Texas Medical Board.
___________________________________________________
Applicant’s Signature
EVALUATING PHYSICIAN:
•A physician who currently holds one of the following positions must complete this evaluation: Chief of Staff, Department Chairman, Medical Director, or Training Director. Letters of recommendation or standard institution verification forms will not be accepted in lieu of this form.
•This completed evaluation should be sent directly to the Texas Medical Board offices via mail, fax, or email.
By mail - Place this form in an envelope of the hospital/institution that you represent, seal the envelope and place your signature over the outside sealed envelope flap. Send to: Texas Medical Board,
By fax - Evaluator must submit the form along with an official hospital/institution coversheet to
By email - Evaluator must submit the form from an official hospital/institution email address to
Title: |
Chief of Staff |
Evaluating Physician’s |
Department Chairman |
Medical Director |
|
Name/Degree: |
Training Director |
Printed
Title:
Phone:Address:
Fax:E-Mail:
Evaluating Physician's License Number and
State of Licensure
LICENSURE APPLICATION FORM L PHYSICIAN LICENSURE EVALUATION |
Version 01.2020 |
FORM L
Applicant's Name___________________________________________ |
Page 2 |
Printed |
|
This is important: All information on this Form L, (including attachments that you provide as the Evaluating Physician) regarding a licensure applicant is confidential pursuant to §164.007(c) of the Medical Practice Act. However, the Board must provide a copy of this Form L and attachments to an applicant when an application is referred to the Licensure Committee for licensure determination. Any information furnished by you is further subject to Chapter 160.010, of the Medical Practice Act, Immunity from Civil Liability.
FOR TRAINING POSITIONS – Completion of the Verification of Post Graduate Training and the Verification of Professional History sections are required.
FOR
VERIFICATION OF POST GRADUATE TRAINING
This section relates to postgraduate training. If this individual did not complete postgraduate training at this institution please skip to the Verification of Professional History section.
|
|
|
|
|
|
|
|
|
|
|
|
Department: |
|
|
|
|
|
PROGRAM PARTICIPATION: (For |
|
|
|
PGY: _______ |
|
|
___________________________________ |
|
|||||
|
|
training positions only) |
|
|
|
___ Internship |
|
|
From: ___/___/___ |
To: ___/___/___ |
|
||||
|
|
Report incomplete postgraduate years |
|
|
|
___ Residency |
|
|
|
||||||
|
|
|
|
|
|
|
Credit received? |
|
|
||||||
|
|
|
|
|
___ Fellowship |
|
|
|
|
||||||
|
|
(PGY) separately from those that were |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
___ Research |
|
|
Full |
*Partial |
in progress |
|
||||
|
|
successfully completed. |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|||||||
|
|
If the postgraduate year is currently in |
|
|
|
|
|
|
*For partial credit– how many months?______ |
|
|||||
|
|
progress, report the expected completion |
|
|
|
|
|
Department: |
|
|
|
||||
|
|
date in the “To” field. |
|
|
|
|
|
PGY: _______ |
|
|
___________________________________ |
|
|||
|
|
Report Internships, Residencies and |
|
|
|
|
|
|
|||||||
|
|
|
|
|
___ Internship |
|
|
From: ___/___/___ |
To: ___/___/___ |
||||||
|
|
Fellowships separately. Use one section |
|
|
|
|
|||||||||
|
|
|
|
___ Residency |
|
|
|
|
|
|
|||||
|
|
per department. |
|
|
|
|
|
|
|
Credit received? |
|
|
|||
|
|
|
|
|
|
|
___ Fellowship |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
___ Research |
|
|
Full |
*Partial |
in progress |
|
|
|
|
|
|
|
|
|
|
|
|
|
*For partial credit– how many months?______ |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Department: |
|
|
|
|
|
|
|
|
|
|
|
|
PGY: _______ |
|
|
___________________________________ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ Internship |
|
|
From: ___/___/___ |
To: ___/___/___ |
|
|
|
|
|
|
|
|
|
|
|
___ Residency |
|
|
Credit received? |
|
|
|
|
|
|
|
|
|
|
|
|
___ Fellowship |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
___ Research |
|
|
Full |
*Partial |
in progress |
|
|
|
|
|
|
|
|
|
|
|
|
|
*For partial credit– how many months?______ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
UNUSUAL |
|
|
Yes No |
1. |
|
Did this individual ever take a leave of absence or break from training? |
|
||||||
|
|
CIRCUMSTANCES: |
|
|
Yes No |
2. |
|
Did this individual resign from training? |
|
|
|||||
|
|
(For training |
|
|
Yes No |
3. |
|
Were any limitations or special requirements placed upon this individual for |
|
||||||
|
|
positions only) |
|
|
|
|
professionalism or behavioral issues? |
|
|
|
|||||
|
|
Please attach an |
|
|
Yes No |
4. |
|
Did this individual ever receive a written warning or documented counseling |
|
||||||
|
|
|
|
|
|
|
about his/her behavior? |
|
|
|
|
||||
|
|
explanation for any |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Yes No |
5. |
|
Was this individual ever placed on probation for any reason? |
|
|||||||
|
|
“yes” response. |
|
|
|
|
|||||||||
|
|
|
|
Yes No |
6. |
|
Is this individual currently under investigation? |
|
|
||||||
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
Yes No |
7. |
|
Were this individual’s privileges or duties ever reduced, suspended, or |
|
||||||
|
|
|
|
|
|
|
|
revoked? |
|
|
|
|
|||
|
|
|
|
|
Yes No |
8. |
|
Did this individual experience delayed promotion or delayed advancement to |
|
||||||
|
|
|
|
|
|
|
|
the next level? |
|
|
|
|
|||
|
|
|
|
|
Yes No |
9. |
|
Was this individual informed his/her contract would not be renewed? |
|
||||||
|
|
|
|
|
Yes No |
10. Was this individual suspended, terminated, or dismissed from training? |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LICENSURE APPLICATION FORM L PHYSICIAN LICENSURE EVALUATION |
Version 01.2020 |
FORM L
Applicant's Name___________________________________________ |
|
Page 3 |
|||
|
|
|
|
|
|
|
VERIFICATION OF PROFESSIONAL HISTORY |
|
|
|
|
1. |
This evaluation is based on Personal Knowledge |
Review of Credential File |
|
||
2. |
How long have you known the applicant? Years________ Months ________ |
|
|||
3. |
Is the applicant related to you? |
|
Yes |
No |
|
4. |
Do you know the applicant well? |
|
Yes |
No |
|
5. |
Has your acquaintance with the applicant continued until recent date? |
Yes |
No |
||
6.Do you consider the applicant:
(a) Reliable? |
Yes |
No |
(b) Ethical? |
Yes |
No |
(c) Of good character? |
Yes |
No |
7.Please rate the applicant:
Excellent |
Good |
Average |
Poor |
(a)Professional ability
(b)Attention to duties
(c)Breadth of education
(d)Interpersonal skills
8.Has applicant, to your knowledge, ever been guilty of:
(a) Fraud or dishonesty? |
Yes |
No |
(b) Unprofessional conduct? |
Yes |
No |
9.To your knowledge, has the applicant ever:
(a) been warned, censured, reprimanded, disciplined, had admissions monitored or privileges limited
or suspended? |
Yes |
No |
(b) had disciplinary action taken against him/her by a licensing agency? |
Yes |
No |
(c) been denied or surrendered a federal or state controlled substance permit? |
Yes |
No |
(d) been arrested, fined, charged with or convicted of a crime, indicted, imprisoned |
|
|
or placed on probation? |
Yes |
No |
(e) been a defendant in a legal action involving professional liability (malpractice) or had a |
|
|
professional liability claim paid in his/her behalf or paid such a claim him/herself? |
Yes |
No |
(f) been placed on probation, asked to withdraw, or reprimanded? |
Yes |
No |
(g) been terminated, resigned in lieu of termination or during investigation? |
Yes |
No |
If you answered "yes" to any of the above questions, please provide any additional information you may have, including the names of other individuals who may have information concerning this applicant.
10. Are the dates of privileges provided by the applicant on the top portion of this form accurate? |
Yes |
No |
11.If not, please provide the correct dates: Beginning month _____ / year ____Ending month _____ / year _______
Evaluating Physicians Name:
Printed |
|
Signature |
Date:
LICENSURE APPLICATION FORM L PHYSICIAN LICENSURE EVALUATION |
Version 01.2020 |
Form Characteristics
| Fact Name | Details |
|---|---|
| Form Purpose | The L 1124 form is used for physician licensure evaluation to verify postgraduate training and professional conduct in Texas. |
| Governing Law | This form is governed by the Texas Medical Practice Act, specifically under §164.007(c) and Chapter 160.010. |
| Applicant Requirements | Applicants must provide evaluations from all facilities with which they have been affiliated in the past five years. |
| Evaluator Credentials | The form must be completed by a physician in a senior position such as Chief of Staff, Department Chairman, Medical Director, or Training Director. |
| Submission Methods | The completed form can be submitted via mail, fax, or email to the Texas Medical Board. Specific guidelines must be followed for each method. |
| Confidentiality Clause | All information submitted through the L 1124 form is confidential but may be provided to the applicant under certain conditions as stipulated by law. |
Guidelines on Utilizing L 1124
Once applicants fill out the L 1124 form, they are taking an important step toward licensure in Texas. After completing the form, it must be submitted to the appropriate evaluating physician, who will add their evaluation before sending it to the Texas Medical Board. Accuracy is essential, as any mistakes could delay the licensing process.
- Begin by filling out the applicant section.
- Enter your current full name.
- If your name was different at the time of affiliation, include that as well.
- Provide your date of birth.
- Fill in your Texas Medical Board ID number, if applicable.
- List your current address.
- Include your phone number and email address.
- Specify the evaluating hospital or institution's name and address.
- Indicate your dates of affiliation (month/year) with the institution.
- Mention your department of affiliation and your position (Intern, Resident, Fellow, Faculty, or Staff).
- Sign the authorization statement, allowing information release to the Texas Medical Board.
- Make sure an evaluating physician fills out their section.
- The physician must hold a position such as Chief of Staff, Department Chairman, Medical Director, or Training Director.
- They need to enter their title, name, degree, contact information, and license number.
- They should complete the appropriate sections regarding postgraduate training if applicable.
- Ensure the evaluating physician answers all relevant questions regarding professional history.
- Lastly, check that the completed form is sent directly to the Texas Medical Board via mail, fax, or email as specified.
Every point they address provides essential insights into your qualifications.
What You Should Know About This Form
What is the purpose of the L 1124 form?
The L 1124 form, also known as the Physician Licensure Evaluation, is used by the Texas Medical Board to verify an applicant's postgraduate training and professional history. It gathers an individual's evaluations from medical facilities they have been associated with within the past five years, ensuring that the applicant meets the necessary qualifications for licensure in Texas.
Who is required to complete the evaluating physician section of the form?
A physician who holds specific roles must complete the evaluating section. The eligible positions include Chief of Staff, Department Chairman, Medical Director, or Training Director. This requirement ensures that only qualified individuals provide evaluations based on the applicant's experience and conduct.
How should the completed L 1124 form be submitted to the Texas Medical Board?
The form can be submitted through one of three methods:
1. By mail—Seal the form in an envelope marked with the evaluating hospital's name and place your signature across the sealed flap. Send it to the designated Texas Medical Board address.
2. By fax—The evaluating physician must send the form with an official coversheet to the designated fax number; submissions from the applicant cannot be accepted.
3. By email—The email must be sent from an official hospital email address to the board. Personal email accounts or those not authorized will not be accepted.
What information is required from the applicant on the L 1124 form?
The applicant must provide their full name, date of birth, TMB ID number, contact information, and details about all affiliated medical institutions within the last five years. This includes the name of the institution, dates of affiliation, department, and the position held during that time.
What confidentiality measures are in place for information on the L 1124 form?
All information provided on the L 1124 form is confidential under the Medical Practice Act. However, the Texas Medical Board is required to give a copy of the form to the applicant if their application is referred to the Licensure Committee for review.
Are there any circumstances that require additional explanations from the evaluating physician?
Yes, if the evaluating physician responds “yes” to any unusual circumstances regarding the applicant's training, they must attach a detailed explanation. Such circumstances could include leaves of absence, disciplinary actions, or suspensions, among others.
How long is the evaluating physician expected to know the applicant?
The evaluating physician should indicate how long they have known the applicant in years and months. This information helps to establish the depth of their knowledge about the applicant's professional conduct and abilities.
What happens if any queries on the L 1124 form receive a "yes" answer?
If a "yes" answer is provided for any question regarding past misconduct or disciplinary actions, the evaluating physician must elaborate on the situation. This ensures that the evaluations are thorough and include relevant context about the applicant's history.
Common mistakes
Filling out the L 1124 form can be straightforward, but many make common mistakes that can delay the process. One of the first mistakes is failing to provide complete information in the applicant section. It is essential for the applicant's full name, date of birth, and other personal details to be accurate and up-to-date. If names differ from those used during affiliation, the applicant must clearly indicate this.
Another frequent error occurs when applicants overlook collecting evaluations from all relevant facilities. The form requires evaluations from every facility affiliated with an applicant in the past five years. Ignoring this requirement can lead to complications or potential rejection of the application.
Sometimes, applicants incorrectly assume all previous evaluations satisfy the requirements. The licensure analyst may ask for additional evaluations beyond the last five years. Applicants should be prepared for this possibility and ensure they have all necessary documentation in hand.
Leaving out the applicant's Texas Medical Board ID number is another mistake. This number must be filled in to help streamline the evaluation. Without it, the form could become confusing for reviewers, which might slow down the processing time.
Providing an incorrect or outdated email address can also lead to communication issues. Evaluators and the Texas Medical Board often reach out for further information or clarification. It’s vital to confirm that the email is current and accessible.
Applicants sometimes misunderstand which parts of the form they need to fill out. Not completing both the Verification of Postgraduate Training and Verification of Professional History sections can lead to further delays. Understanding the requirements for training and non-training positions is crucial.
Another common misstep is neglecting to sign the form. The applicant's signature is a necessary step in granting permission for evaluations and records to be released. Without this, the form will be considered incomplete.
Miscommunication can arise when evaluators fail to send the completed form directly to the Texas Medical Board. It must be sent via the provided channels—mail, fax, or email—without any extra steps like personal delivery by the applicant.
Sometimes, evaluators submit the form without the required coversheet or from a personal email. This will lead to a refusal of the submission. Ensuring that the evaluation is complete and follows all submission guidelines is key.
Lastly, failing to provide truthful and thorough answers about the applicant's professional history can have serious consequences. Dishonesty can lead to denials, delays, or reputational issues down the line. Clear and honest communication throughout the evaluation process is best.
Documents used along the form
When applying for a medical license in Texas, it's essential to have the necessary documents ready. Along with the FORM L, applicants may need additional forms to support their application. Each of these forms plays a vital role in presenting a complete and accurate profile to the Texas Medical Board.
- FORM L-1: Verification of Postgraduate Training - This form confirms the details of the applicant's training and experience. It includes information about internships, residencies, and fellowships, documenting the applicant's medical training history.
- FORM L-2: Verification of Professional History - This document outlines the applicant's professional conduct and history. It gathers insights from colleagues and supervisors regarding the applicant's reliability, ethics, and overall character in a professional setting.
- FORM L-3: Letters of Recommendation - While not a formal requirement, letters from reputable professionals in the medical field can supplement the application. These letters provide personal insights and validations of the applicant's character and competency.
- COPY OF MEDICAL DEGREE - A photocopy of the applicant's medical degree is necessary to verify their educational background. This document confirms the completion of medical education and serves as proof of qualification to practice medicine.
Gathering these documents ensures a thorough and well-supported application. Take care to complete each form accurately. Demonstrating a complete picture of training, professional history, and qualifications helps the Texas Medical Board make a fair assessment of your application.
Similar forms
- Form L serves a specific purpose like the ACGME Verification Form. Both documents require detailed evaluations of a physician's training and professional history. ACGME also mandates information about postgraduate training, much like Form L.
- Medical Board Verification Form is similar to Form L in that both necessitate verification from prior training institutions. Each form aims to ensure that data regarding a physician's qualifications and training is accurate and complete.
- State License Application often parallels Form L because both include personal information, educational background, and professional evaluations. They serve as crucial tools in assessing a physician's qualifications to practice medicine.
- Credentialing Application mirrors Form L by collecting pertinent data from various medical facilities. The credentialing process requires similar information about medical training and any affiliations a physician may have held.
- Peer Review Evaluation showcases similarities with Form L, particularly regarding the evaluation of a physician's professional conduct and competence. Both require feedback from colleagues and supervisors to assess a physician's qualifications accurately.
Dos and Don'ts
When filling out the L 1124 form, consider the following do's and don'ts to ensure a smooth application process:
- Do provide accurate and complete information on the form.
- Do list every facility you have been affiliated with in the past five years.
- Do ensure the evaluating physician is qualified and holds an appropriate position.
- Do have the evaluating physician submit the form directly to the Texas Medical Board via the approved methods.
- Don't send the form without the necessary coversheet when submitting by fax.
- Don't use personal email addresses for submission; always use professional or institutional email accounts.
It's vital to follow these guidelines closely. This helps avoid unnecessary delays in your licensure evaluation. Make double-checking details part of your routine. Taking these steps seriously reflects your professionalism and respect for the process.
Misconceptions
- Misconception 1: The L 1124 form is only necessary for new applicants.
- Misconception 2: Evaluations are only needed for the last year of training.
- Misconception 3: Any physician can complete this evaluation form.
- Misconception 4: Submitting the form by fax is an informal method.
- Misconception 5: Only training history is evaluated.
- Misconception 6: Providing an evaluation guarantees licensure.
- Misconception 7: The information in the evaluation can be shared without restrictions.
- Misconception 8: Audits of submitted evaluations do not occur.
- Misconception 9: Evaluating physicians are not held accountable for their assessments.
- Misconception 10: Email submissions are the preferred method for this evaluation.
This form is also required when current license holders apply for reinstatement or additional privileges, not just for new applicants.
Applicants must have evaluations from every facility affiliated with them in the past five years. This requirement ensures a comprehensive view of their training history.
The evaluation must be completed by specific positions such as Chief of Staff or Medical Director. Letters of recommendation are not acceptable substitutes.
Fax submissions must include an official coversheet. Applications without this can be rejected. It ensures documentation and verification are handled professionally.
Both the Verification of Postgraduate Training and the Verification of Professional History sections must be completed. This includes assessing professional conduct and history.
The evaluation is only one component of the application process. The final decision rests with the Texas Medical Board after considering all submitted information.
Most information is kept confidential. However, if an application is referred to the Licensure Committee, the applicant may receive copies of their evaluation and attachments.
The Texas Medical Board may verify the information provided. Inaccurate or misleading information may result in penalties or refusal of licensure.
Evaluating physicians must provide accurate and truthful evaluations. Legal protections are in place for those who provide honest assessments, but there are consequences for providing false information.
Email submissions must originate from a valid hospital or institution email address. Applications sent from the applicant’s personal email will not be accepted.
Key takeaways
- Complete all sections of the L 1124 form accurately, including personal information and details about postgraduate training.
- It is essential to obtain evaluations from every facility affiliated with the applicant over the past five years, with possible additional evaluations required by the licensure analyst.
- Gather all required signatures before submitting the form to ensure it is considered valid.
- The evaluating physician must hold a specific position—such as Chief of Staff or Medical Director—to complete the evaluation section of the form.
- Submit the completed form directly to the Texas Medical Board by mail, fax, or email, ensuring the correct procedures are followed for each submission method.
- All evaluations are confidential and are protected under the Medical Practice Act, though the applicant may review information if their application is referred to the Licensure Committee.
- For training positions, both the Verification of Postgraduate Training and Verification of Professional History sections must be filled out.
- For non-training positions, only the Verification of Professional History section is necessary.
- Complete the unusual circumstances section thoroughly to provide a clear understanding of the applicant's professional history.
Browse Other Templates
Michigan Medicaid Eligibility for Seniors - If assistance is needed, local offices are available for direct support during office hours.
Libc-500 - Contact information for the employer's insurance company is mandatory.
Credit Repair Agreement Template - Clients will receive a disclosure about their credit file rights prior to signing the contract.