Fill Out Your Mhcc 15 Form
The MHCC-15 form plays a crucial role in the process of transporting individuals in need of mental health and addiction services in the state of Connecticut. This form must be completed accurately and submitted within three months of the service to ensure timely processing. It is important for those involved in the transportation of patients—physicians, treatment providers, and receiving facilities—to adhere to specific instructions outlined within the form. First, transportation should be arranged using the least expensive option that still provides necessary safety measures. A key requirement for the form includes the certification that the patient being transported has either psychiatric disabilities or substance abuse issues, with clear indications of the reason for transportation. The authorization section requires the examining physician's signature, as well as the provider's notification that the patient requested the transport. A section is also defined for the receiving facility to acknowledge the patient’s arrival and the details of the transportation service used. Lastly, the ambulance company must attest to the attempts made to secure payment for the transportation. The comprehensive nature of the MHCC-15 form facilitates accountability and streamlines the process for mental health and addiction services transportation within the state. These components together ensure that patients are transported safely and that their needs are properly addressed while providing a clear record for administrative and financial purposes.
Mhcc 15 Example
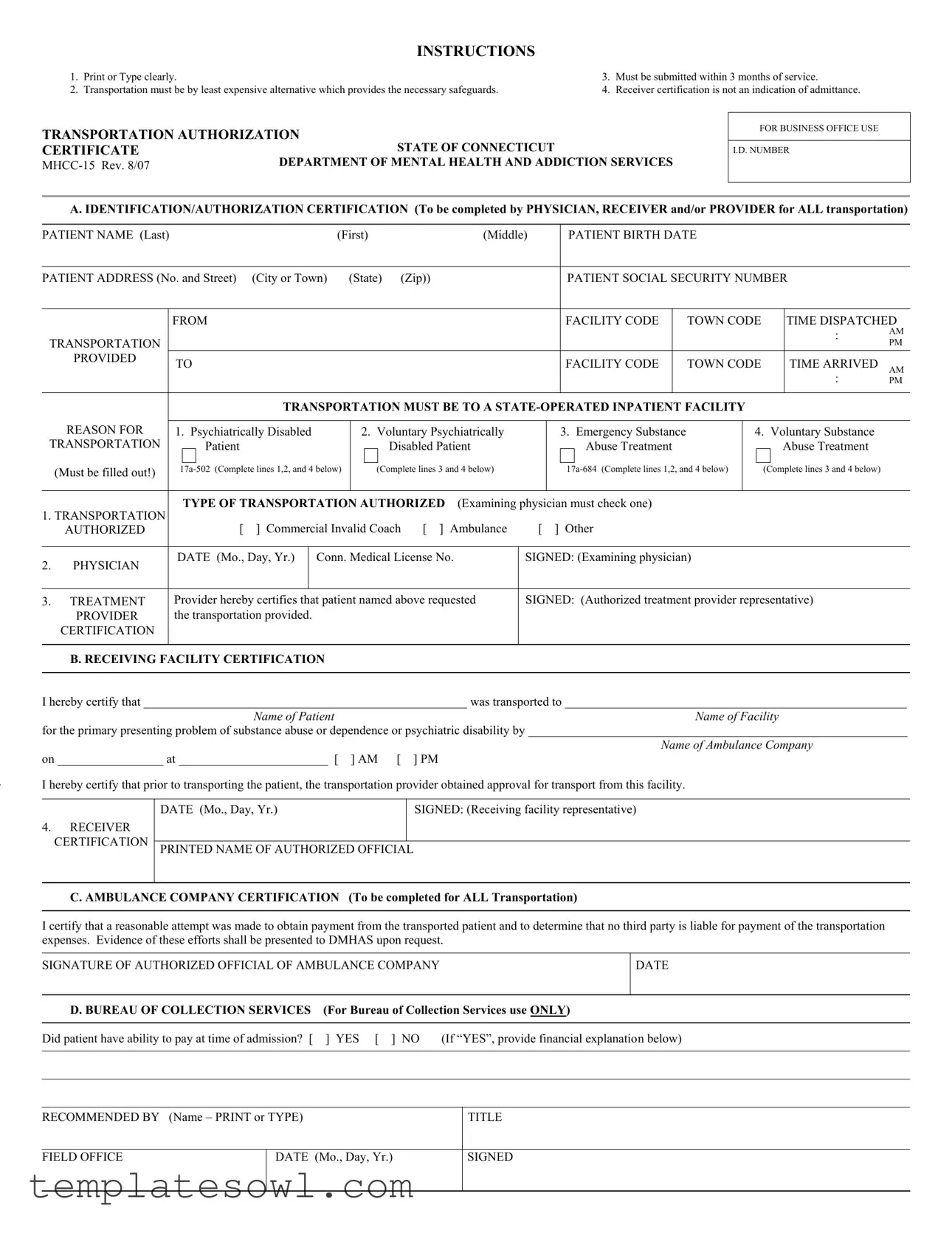
INSTRUCTIONS
1.Print or Type clearly.
2.Transportation must be by least expensive alternative which provides the necessary safeguards.
3.Must be submitted within 3 months of service.
4.Receiver certification is not an indication of admittance.
TRANSPORTATION AUTHORIZATION
CERTIFICATE |
STATE OF CONNECTICUT |
DEPARTMENT OF MENTAL HEALTH AND ADDICTION SERVICES |
|
|
FOR BUSINESS OFFICE USE
I.D. NUMBER
A. IDENTIFICATION/AUTHORIZATION CERTIFICATION (To be completed by PHYSICIAN, RECEIVER and/or PROVIDER for ALL transportation)
PATIENT NAME (Last) |
|
|
|
|
(First) |
(Middle) |
|
PATIENT BIRTH DATE |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
PATIENT ADDRESS (No. and Street) |
(City or Town) |
(State) (Zip)) |
|
|
|
PATIENT SOCIAL SECURITY NUMBER |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM |
|
|
|
|
|
|
|
|
FACILITY CODE |
|
TOWN CODE |
|
|
TIME DISPATCHED |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
: |
AM |
TRANSPORTATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
PROVIDED |
|
TO |
|
|
|
|
|
|
|
|
FACILITY CODE |
|
TOWN CODE |
|
|
TIME ARRIVED |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AM |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
: |
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
TRANSPORTATION MUST BE TO A |
|
|
|
|
|||||||||||||
|
REASON FOR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
1. Psychiatrically Disabled |
2. Voluntary Psychiatrically |
|
|
3. Emergency Substance |
|
4. Voluntary Substance |
|
||||||||||||||
TRANSPORTATION |
|
|
|
Patient |
|
|
|
|
Disabled Patient |
|
|
|
Abuse Treatment |
|
|
|
|
Abuse Treatment |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
(Must be filled out!) |
|
|
(Complete lines 3 and 4 below) |
|
|
|
|
(Complete lines 3 and 4 below) |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TYPE OF TRANSPORTATION AUTHORIZED |
(Examining physician must check one) |
|
|
|
|
|
|
|
|||||||||||
1. TRANSPORTATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AUTHORIZED |
|
[ |
] Commercial Invalid Coach [ ] Ambulance |
[ |
] Other |
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
2. |
PHYSICIAN |
|
DATE (Mo., Day, Yr.) |
Conn. Medical License No. |
|
SIGNED: (Examining physician) |
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|||||||||||||||||
3. |
TREATMENT |
|
Provider hereby certifies that patient named above requested |
SIGNED: (Authorized treatment provider representative) |
|
||||||||||||||||||
|
PROVIDER |
|
the transportation provided. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
CERTIFICATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. RECEIVING FACILITY CERTIFICATION
I hereby certify that ____________________________________________________ was transported to _______________________________________________________
Name of PatientName of Facility
for the primary presenting problem of substance abuse or dependence or psychiatric disability by _____________________________________________________________
Name of Ambulance Company
on _________________ at ________________________ [ ] AM [ ] PM
I hereby certify that prior to transporting the patient, the transportation provider obtained approval for transport from this facility.
4.RECEIVER CERTIFICATION
DATE (Mo., Day, Yr.) |
SIGNED: (Receiving facility representative) |
|
|
PRINTED NAME OF AUTHORIZED OFFICIAL
C. AMBULANCE COMPANY CERTIFICATION (To be completed for ALL Transportation)
I certify that a reasonable attempt was made to obtain payment from the transported patient and to determine that no third party is liable for payment of the transportation expenses. Evidence of these efforts shall be presented to DMHAS upon request.
SIGNATURE OF AUTHORIZED OFFICIAL OF AMBULANCE COMPANY
DATE
D. BUREAU OF COLLECTION SERVICES |
(For Bureau of Collection Services use ONLY) |
|
|
Did patient have ability to pay at time of admission? [ |
] YES [ ] NO (If “YES”, provide financial explanation below) |
|
|
|
|
RECOMMENDED BY (Name – PRINT or TYPE)
TITLE
FIELD OFFICE
DATE (Mo., Day, Yr.)
SIGNED
Form Characteristics
| Fact Name | Fact Description |
|---|---|
| Purpose of Form | The MHCC-15 form is used to authorize transportation for patients with psychiatric or substance abuse issues. |
| Legislation Reference | This form is governed by Connecticut General Statutes, specifically sections 17a-502 and 17a-684. |
| Submission Timeline | It must be submitted within three months from the date of service to ensure processing. |
| Identification Requirement | Identification details, including the patient's name, birth date, and social security number, are mandatory to complete the form. |
| Transportation Method | The transportation chosen must be the least expensive option that still ensures proper safety for the patient. |
| Receiver Certification | Receiver certification does not guarantee that the patient has been admitted to the facility. |
| Certification Responsibilities | Physicians, receivers, and providers all share the responsibility for certifying patient transportation. |
| Documentation Requirement | It is essential to document the reason for transportation, including options like psychiatric disability or substance abuse treatment. |
| Amended Version | The current version of the MHCC-15 form was last revised in August 2007. |
| Ambulance Company Certification | The ambulance company must also certify that attempts were made to obtain payment from the patient before transport. |
Guidelines on Utilizing Mhcc 15
Completing the MHCC-15 form is an essential step for ensuring that transportation is documented correctly within Connecticut’s mental health and addiction services framework. This structured format helps in gathering necessary information about the patient and the transportation process itself. After filling out this form, the next steps would typically involve submitting it to the relevant department within three months of the service provided.
- Gather all necessary information. Ensure you have the patient’s name, birth date, address, and Social Security number handy, along with the transportation details and certifications needed.
- Print or type clearly. This ensures that all information is legible and correctly understood.
- Complete the patient identification section. Fill in the patient’s last name, first name, middle name, birth date, address, and Social Security number.
- Document the transportation details. Include information about the facility code, town code, and times of dispatch and arrival.
- Indicate the reason for transportation. Choose the appropriate reason from the options provided: psychiatrically disabled, voluntary psychiatrically disabled, emergency substance abuse treatment, or voluntary substance abuse treatment.
- Authorize the type of transportation. The examining physician needs to check the appropriate box for whether the transportation authorized is via commercial invalid coach, ambulance, or other means.
- Get the physician’s signature. Ensure the examining physician signs the form and includes their medical license number and the date.
- Have the treatment provider sign. The authorized treatment provider must also certify the transportation request and sign the form.
- Fill out the receiving facility certification section. Certify that the patient was successfully transported to the designated facility and fill in all corresponding details, including the name of the ambulance company and the time of transport.
- Obtain the receiving facility representative's signature. Ensure that the date and printed name of the authorized official are also included.
- Complete the ambulance company certification section. Include the authorized official's signature and date, certifying that payment attempts were made.
- Review and submit the form. Double-check all the entries for accuracy before submitting within the given timeframe.
What You Should Know About This Form
What is the purpose of the MHCC 15 form?
The MHCC 15 form serves as an authorization certificate for transportation to state-operated inpatient facilities in Connecticut for individuals with psychiatric or substance use disorders. It ensures that the necessary protocols are followed during the transport of patients and verifies that the transportation options used are the least expensive and most appropriate for the patient's needs.
Who needs to complete the MHCC 15 form?
The form requires completion by various parties involved in the patient’s transportation process. This includes the examining physician, the treatment provider, and representatives from the receiving facility. Each party plays a crucial role in ensuring that the patient's transportation is appropriately authorized and documented.
When must the MHCC 15 form be submitted?
The form must be submitted within three months following the transportation service. Timely submission is important to ensure compliance with state regulations and to support any necessary billing processes.
What types of transportation can be authorized on the MHCC 15 form?
The form allows for several types of transportation to be indicated by the physician. Options include commercial invalid coach, ambulance services, or other types of transport deemed appropriate. The selected mode should be the least expensive alternative while still ensuring adequate patient safety and care.
Does the receiver certification indicate patient admission?
No, the receiver certification included in the MHCC 15 form does not indicate that the patient has been admitted to the facility. It simply signifies that the patient was transported to the facility for assessment or treatment. Acceptance of the patient into the facility is a separate process.
What is required from the ambulance company for the completion of the form?
The ambulance company must certify that they made reasonable attempts to obtain payment from the patient and confirm that no third party is liable for transportation expenses. This certification must include a signature from an authorized official of the company. Documentation of efforts made to ascertain payment will need to be provided to the Department of Mental Health and Addiction Services if requested.
Common mistakes
Filling out the MHCC-15 form can appear straightforward, but it's easy to make mistakes that could cause delays in processing. One common error is failing to print or type the information clearly. This form requires legibility to ensure that all details can be read without confusion. Illegible handwriting or unclear typing may lead to incorrect assumptions or the rejection of the form altogether.
Another frequent mistake occurs when individuals do not confirm that they are using the least expensive transportation option. The form specifically states that transportation must be the least costly alternative that still meets necessary safety standards. Ignoring this requirement might not only lead to increased costs but also impact the approval of the transportation authorization.
Timeliness is also crucial when submitting the MHCC-15 form. It must be filed within three months of the service being provided. Many apply late and are surprised to find their request rejected because they missed the deadline. Planning ahead and understanding this timeline can prevent unnecessary frustration.
Checking the correct reason for transportation is another area where mistakes often occur. The form has several options for indicating why a patient requires transport, from psychiatric disabilities to substance abuse treatment. Omitting this information or selecting an incorrect option can cause significant delays, as the approval process relies heavily on accurate and complete information.
Additionally, some may overlook the certification sections that require signatures from various parties involved in the transportation process. Each section—the physician, the receiving facility, and the ambulance company—needs to be signed appropriately. A missing signature can halt the processing of the authorization and prolong care.
Lastly, awareness of whether third-party payment exists is essential. Failing to indicate any attempts to secure payment from the patient or a third party can also complicate matters. If the ambulance company does not clarify this information, it might lead to additional scrutiny or denial of the transportation claim.
Documents used along the form
The MHCC 15 form is a vital document for transportation authorization within the Connecticut Department of Mental Health and Addiction Services. It often accompanies several other forms and documents to ensure a complete and smooth process. Below is a list of related forms typically used alongside the MHCC 15.
- Patient Intake Form: This document collects essential information about the patient's medical history and current condition. It helps healthcare providers understand the needs of the patient better.
- Transportation Request Form: Used to formally request transportation services. This form outlines the details of the transport, including pickup and destination addresses, times, and the type of transport needed.
- Authorization for Release of Information: This form grants permission to share a patient’s medical information with the transportation provider and other relevant entities. It ensures compliance with privacy laws.
- Insurance Verification Form: This document confirms the patient's insurance coverage for transportation services. It helps identify responsible parties for payment ahead of the service.
- Patient Safety Checklist: A form that details any safety concerns or requirements specific to the patient's condition. It informs the transport team of necessary precautions during transit.
- Incident Report: If any issues arise during transportation, this document is used to record details about what happened. This can include accidents, medical emergencies, or other unexpected events.
- Facility Admission Record: This document is completed when the patient arrives at the receiving facility, confirming their admission and the reason for transport. It is crucial for maintaining accurate records.
- Emergency Contact Form: This form contains information about who to contact in case of an emergency during transportation. It ensures that the transport team has the necessary details to reach family or guardians quickly.
- Consent for Treatment Form: This authorizes healthcare providers to administer treatment to the patient upon arrival at the facility. It is an essential legal document that ensures informed consent.
Using these forms together with the MHCC 15 ensures that the transportation process is thorough and compliant with all necessary regulations. This approach supports the patient’s needs and aligns with legal requirements in healthcare services.
Similar forms
The MHCC 15 form is a specific document used for authorizing transportation for individuals needing mental health or addiction services in Connecticut. It has similarities with various other forms used in similar contexts. Below is a comparison of the MHCC 15 form with ten similar documents:
- CMS 1500 - This form is used for billing and certification of medical services. Like the MHCC 15, it requires detailed patient information and documentation of medical necessity for services rendered.
- Supplemental Security Income (SSI) Application - This application form collects information for individuals seeking financial assistance. Both documents require accurate personal details and validation of eligibility through medical documentation.
- Authorization for Release of Medical Information - This form allows health care providers to share patient information. Similar to the MHCC 15, it must be signed by the patient or an authorized representative, ensuring proper consent is obtained.
- Patient Transfer Authorization Form - Used when transferring patients between facilities, this document shares the same goal of ensuring safe transportation and needs detailed patient information and approval from providers.
- Informed Consent for Treatment Form - This verifies that patients understand their treatment options. Both forms focus on ensuring patient awareness and consent before proceeding with a form of service.
- Emergency Medical Services (EMS) Trip Ticket - EMS providers use this document to record details of ambulance transports. Like the MHCC 15, it captures transport details and requires signatures from medical personnel involved.
- Discharge Summary Form - This summarizes a patient's treatment upon leaving a facility. Both documents focus on patient care and record-keeping, providing essential information for continuity of care.
- Behavioral Health Care Authorization Form - Similar in purpose, this form authorizes specific mental health services and requires patient information and provider signatures, much like the MHCC 15.
- Transportation Request Form - Often used by hospitals, this form authorizes patient transport and collects similar data as the MHCC 15, including patient identification and transportation needs.
- Patient Services Notification Form - Used to document and authorize patient services, it also requests patient details and service requirements, paralleling the structure of the MHCC 15.
The similarities among these documents highlight the importance of accurate information and proper authorization in health care and transportation situations, promoting safety and compliance across all services.
Dos and Don'ts
When filling out the MHCC 15 form, it’s important to get it right. Here are some suggestions and avoidances that can help guide you through the process.
- Do print or type clearly. Legibility is key to ensuring your application is processed smoothly.
- Don’t forget to submit the form within three months of service. Late submissions can lead to delays or denial of requests.
- Do confirm that the transportation is the least expensive option available while still providing necessary safety measures.
- Don’t assume that receiver certification means admittance. Clarify details with the facility if unsure.
- Do fill out all required fields, including patient identification and transportation details. Missing information can slow down processing.
- Don’t leave any sections incomplete. Each part of the form serves a purpose and needs to be filled out to avoid issues.
- Do obtain necessary signatures from the examining physician and receiving facility representatives. Their certifications are crucial.
- Don’t overlook the section for ambulance company certification. It’s vital for verifications and future reference.
- Do double-check all details before submission. This includes names, dates, and any other critical information.
- Don’t forget to keep a copy of the completed form for your records. It’s useful for tracking and follow-up purposes.
Following these guidelines can make the process of filling out the MHCC 15 form smoother and more efficient. Stay informed and pay attention to every detail to ensure successful completion.
Misconceptions
-
Misconception 1: The MHCC 15 form is only for emergency transport situations.
This form can be used for a variety of transportation needs, not just emergencies. It includes options for voluntary treatment for both psychiatric disabilities and substance abuse.
-
Misconception 2: It’s too late to submit the MHCC 15 form after three months.
This form must indeed be submitted within three months of the service. Delaying submission can affect transport reimbursement, so it’s crucial to submit on time.
-
Misconception 3: The receiver certification guarantees patient admission to the facility.
The receiver's certification only confirms the transport took place; it does not guarantee that the patient will be admitted to the receiving facility.
-
Misconception 4: Only specific types of transport are allowed.
The form allows for different types of transport, such as commercial invalid coaches and ambulances. Each situation may require a different form of transportation based on the patient's needs.
-
Misconception 5: The physician’s signature is optional for the MHCC 15 form.
The signature of the examining physician is mandatory. It authenticates the request for transportation and ensures that all necessary medical considerations have been addressed.
Key takeaways
Filling out and using the MHCC 15 form requires careful attention to detail. Here are key takeaways to consider:
- Print or Type Clearly: Clear and legible handwriting or typing is essential when completing the form.
- Cost-Effective Transportation: The form mandates that the transportation utilized must be the least expensive option that still ensures necessary safeguards are in place.
- Submission Timeline: Submit the MHCC 15 form within three months of the service date to ensure it is processed correctly.
- Receiver Certification: It is important to understand that the receiver certification does not confirm patient admission to a facility.
- Patient Information: Complete all patient identification fields accurately, including full name, date of birth, address, and social security number.
- Transportation Details: The form requires specific information regarding the transportation, including times dispatched and arrived.
- Authorized Physician Signature: An authorized physician must sign the form, confirming transport and providing their medical license number.
- Transport Provider’s Certification: The treatment provider must certify that the transportation was requested by the patient and sign the form accordingly.
Completing each section accurately and promptly will facilitate effective processing and compliance with guidelines regarding patient transportation.
Browse Other Templates
DACA Application Form,Deferred Action Consideration Application,Childhood Arrival Status Request,Form for Deferred Action for Childhood Arrivals,USCIS DACA Request Form,Form for Childhood Arrivals Deferred Action,Initial DACA and Renewal Application, - The I-821D form can be submitted for both initial requests and renewals of DACA status.
Equitable Withdrawal Form - To initiate your request, ensure you have read the hardship withdrawal requirements included at the end of the form.