Fill Out Your Gn 80124 Cg Form
The Gn 80124 Cg form, commonly referred to as the Humana Employee Change Form, plays a crucial role in managing employee benefits in a structured manner. It provides a user-friendly interface where employees can easily indicate necessary changes to their medical, dental, life, and vision benefits. Utilizing the form ensures that all relevant employee information, including Social Security numbers and benefit classes, is captured clearly and systematically. In addition to updating personal details, the form allows users to handle changes for dependents, making it a vital tool for families navigating their benefits. Following a qualifying event, such as marriage or the birth of a child, employees can specify the necessary updates, ensuring that their benefits reflect their current situation. With a straightforward compilation of sections dedicated to personal information, dependent changes, and beneficiary designations, the Gn 80124 Cg form streamlines what could otherwise be a complex process. Overall, this form is an essential resource that promotes clarity and efficiency in managing employee benefits, ultimately enhancing the overall employee experience.
Gn 80124 Cg Example
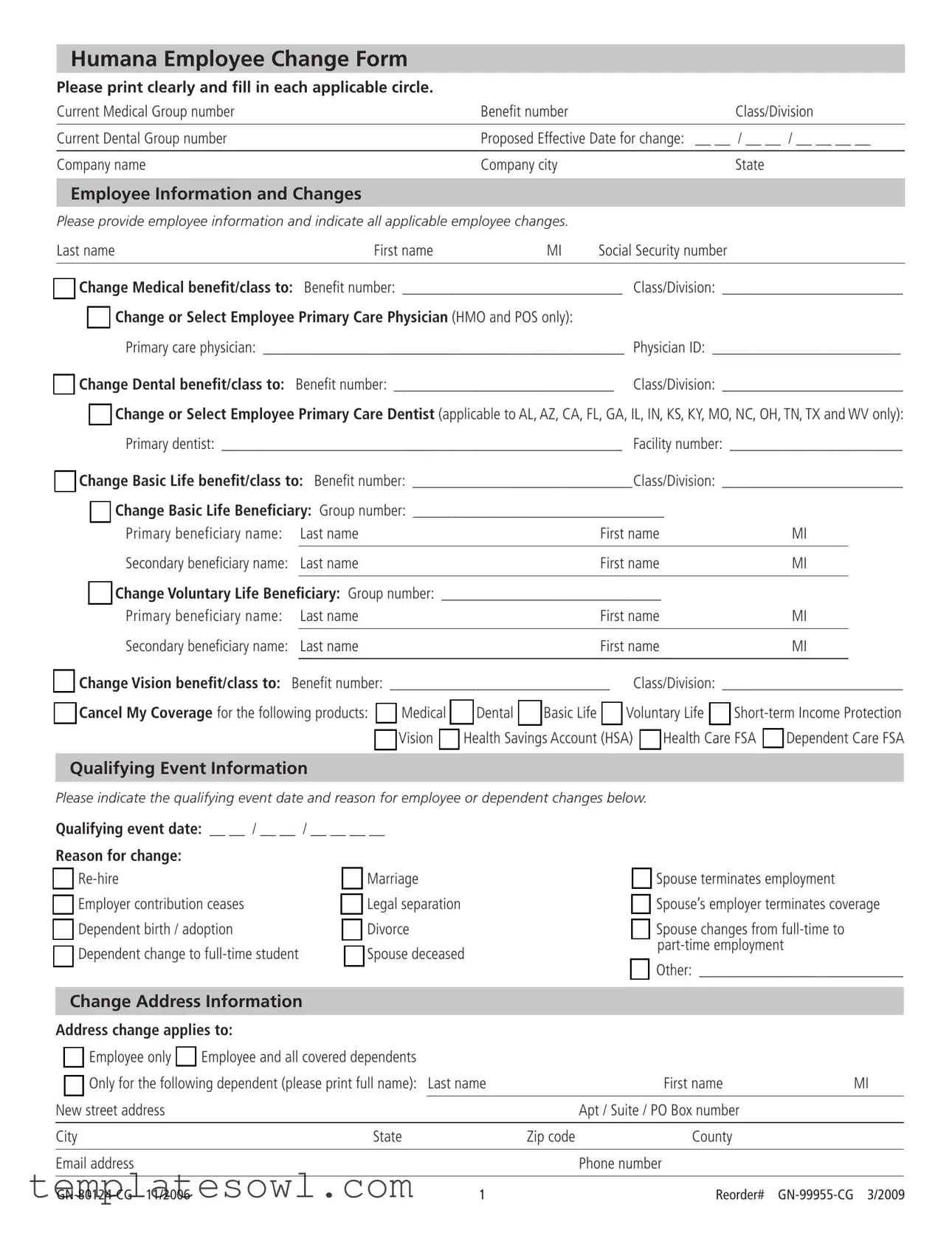
Humana Employee Change Form
Please print clearly and fill in each applicable circle. |
|
|
Current Medical Group number |
Benefit number |
Class/Division |
|
|
|
Current Dental Group number |
Proposed Effective Date for change: |
__ __ / __ __ / __ __ __ __ |
|
|
|
Company name |
Company city |
State |
Employee Information and Changes
Please provide employee information and indicate all applicable employee changes.
Last name |
First name |
MI |
Social Security number |
|
|
|
|
mChange Medical benefit/class to: Benefit number: ____________________________ Class/Division: _______________________
m Change or Select Employee Primary Care Physician (HMO and POS only):
Primary care physician: ______________________________________________ Physician ID: ________________________
m Change Dental benefit/class to: Benefit number: ____________________________ Class/Division: _______________________
mChange or Select Employee Primary Care Dentist (applicable to AL, AZ, CA, FL, GA, IL, IN, KS, KY, MO, NC, OH, TN, TX and WV only): Primary dentist: ___________________________________________________ Facility number: ______________________
mChange Basic Life benefit/class to: Benefit number: ____________________________Class/Division: _______________________
mChange Basic Life Beneficiary: Group number: ________________________________
Primary beneficiary name: |
Last name |
First name |
MI |
|
|
|
|
Secondary beneficiary name: |
Last name |
First name |
MI |
|
|
|
|
mChange Voluntary Life Beneficiary: Group number: ____________________________
Primary beneficiary name: |
|
Last name |
First name |
MI |
|
|
|
|
|
|
|
Secondary beneficiary name: |
|
Last name |
First name |
MI |
|
m Change Vision benefit/class to: |
|
|
|
||
Benefit number: ____________________________ Class/Division: _______________________ |
|||||
mCancel My Coverage for the following products: m Medical m Dental m Basic Life m Voluntary Life m
Qualifying Event Information
Please indicate the qualifying event date and reason for employee or dependent changes below.
Qualifying event date: __ __ / __ __ / __ __ __ __
Reason for change: |
|
m |
m Marriage |
m Employer contribution ceases |
m Legal separation |
m Dependent birth / adoption |
m Divorce |
m Dependent change to |
m Spouse deceased |
mSpouse terminates employment
mSpouse’s employer terminates coverage
mSpouse changes from
mOther: __________________________
Change Address Information
Address change applies to:
mEmployee only m Employee and all covered dependents
m Only for the following dependent (please print full name): Last name |
|
First name |
MI |
||
|
|
|
|
|
|
New street address |
|
|
|
Apt / Suite / PO Box number |
|
|
|
|
|
|
|
City |
State |
Zip code |
County |
|
|
|
|
|
|
|
|
Email address |
|
|
|
Phone number |
|
|
|
|
|
|
|
1 |
Reorder# |
Group Number
Dependent Changes
Please complete this section for all dependent changes.
Social Security Number
1 Last name |
First name |
MI |
Date of birth |
_ _ / _ _ / _ _ _ _ |
|
|
Social Security number |
Gender: m Female m Male |
Relationship: m Spouse |
m Child m Other: |
|
|
|
|
|
|
|
|
Dependent status (if applicable): |
m |
If disabled, indicate reason: |
|
|
|
|
|
|
||
m Add or m Delete dependent to/from my current plan for the following products: m Medical |
m Dental |
m Basic Life |
|||
|
|
|
m Voluntary Life |
m Vision |
|
mChange or Select Primary Care Physician (HMO and POS only):
Primary care physician: __________________________________________________ Physician ID: ________________________
mChange or Select DHMO (applicable to AL, AZ, CA, FL, GA, IL, IN, KS, KY, MO, NC, OH, TN, TX and WV only):
Primary dentist: _______________________________________________________ Facility number: ______________________
|
|
|
|
|
|
|
2 Last name |
First name |
MI |
Date of birth |
_ _ / _ _ / _ _ _ _ |
||
|
|
Social Security number |
Gender: m Female m Male |
Relationship: m Spouse |
m Child m Other: |
|
|
|
|
|
|
|
|
|
|
Dependent status (if applicable): |
m |
If disabled, indicate reason: |
|
|
|
|
|
|
|
||
|
m Add or m Delete dependent to/from my current plan for the following products: m Medical |
m Dental |
m Basic Life |
|||
|
|
|
|
m Voluntary Life |
m Vision |
|
mChange or Select Primary Care Physician (HMO and POS only):
Primary care physician: __________________________________________________ Physician ID: ________________________
mChange or Select DHMO (applicable to AL, AZ, CA, FL, GA, IL, IN, KS, KY, MO, NC, OH, TN, TX and WV only):
Primary dentist: _______________________________________________________ Facility number: ______________________
3 Last name |
First name |
MI |
Date of birth |
_ _ / _ _ / _ _ _ _ |
|
|
Social Security number |
Gender: m Female m Male |
Relationship: m Spouse |
m Child m Other: |
|
|
|
|
|
|
|
|
Dependent status (if applicable): |
m |
If disabled, indicate reason: |
|
|
|
|
|
|
||
m Add or m Delete dependent to/from my current plan for the following products: m Medical |
m Dental |
m Basic Life |
|||
|
|
|
m Voluntary Life |
m Vision |
|
mChange or Select Primary Care Physician (HMO and POS only):
Primary care physician: __________________________________________________ Physician ID: ________________________
mChange or Select DHMO (applicable to AL, AZ, CA, FL, GA, IL, IN, KS, KY, MO, NC, OH, TN, TX and WV only):
Primary dentist: _______________________________________________________ Facility number: ______________________
4 Last name |
First name |
MI |
Date of birth |
_ _ / _ _ / _ _ _ _ |
|
|
Social Security number |
Gender: m Female m Male |
Relationship: m Spouse |
m Child m Other: |
|
|
|
|
|
|
|
|
Dependent status (if applicable): |
m |
If disabled, indicate reason: |
|
|
|
|
|
|
||
m Add or m Delete dependent to/from my current plan for the following products: m Medical |
m Dental |
m Basic Life |
|||
|
|
|
m Voluntary Life |
m Vision |
|
mChange or Select Primary Care Physician (HMO and POS only):
Primary care physician: __________________________________________________ Physician ID: ________________________
mChange or Select DHMO (applicable to AL, AZ, CA, FL, GA, IL, IN, KS, KY, MO, NC, OH, TN, TX and WV only):
Primary dentist: _______________________________________________________ Facility number: ______________________
Signature - please sign below if requesting changes
Employee or legal representative signature: ______________________________________________ Date: ______________________
Name and relationship of legal representative: _________________________________________________________________________
2 |
Reorder# |
Print&Submit
Reset
Form Characteristics
| Fact Name | Details |
|---|---|
| Form Purpose | The GN 80124 Cg form is used by employees to request changes to their health benefits, including medical, dental, and life insurance. |
| Governing Laws | This form is governed by state-specific insurance laws and regulations applicable in states such as AL, AZ, CA, FL, GA, IL, IN, KS, KY, MO, NC, OH, TN, TX, and WV where certain benefits are applicable. |
| Qualifying Events | Employees must indicate qualifying events such as marriage, divorce, or birth/adoption of a dependent that prompt changes in benefit coverage. |
| Dependent Changes | The form allows for changes relating to dependents, including adding or deleting dependents from the health plan. |
| Effective Date | Employees can specify a proposed effective date for the requested changes, ensuring clarity on when changes should take effect. |
| Signature Requirement | The form must be signed by the employee or a legal representative to validate the requested changes, capturing consent. |
Guidelines on Utilizing Gn 80124 Cg
Completing the Gn 80124 Cg form is an essential step when you need to make changes to your employee benefits. It's important to fill out this form carefully to ensure your changes are processed accurately and quickly. Take your time as you gather the necessary information and follow the steps outlined below.
- Print the form clearly to avoid any confusion.
- Fill in the current group and benefit numbers at the top of the form.
- Enter the proposed effective date for the change in the specified format (MM/DD/YYYY).
- Provide the company name, city, and state.
- In the "Employee Information" section, fill in your last name, first name, middle initial, and social security number.
- Check the box to change your medical benefit/class and enter the new benefit number and class/division.
- Indicate if you want to change the primary care physician by writing their name and physician ID (if applicable).
- Repeat the same procedure for dental benefits, including the necessary benefit number and class/division.
- Follow the instructions for changing life insurance benefits, including naming the primary and secondary beneficiaries.
- Specify if you want to change or cancel other benefits, such as vision, short-term income protection, or HSAs.
- Complete the "Qualifying Event Information" section, including the event date and select the reason for your change.
- If you are changing your address, fill in the new street address and any apartment or box number, along with the city, state, zip code, and county.
- For dependent changes, provide the necessary information for each dependent, including their relationship to you and their date of birth.
- Finally, sign the form and date it. If a legal representative is signing, include their name and relationship as well.
After completing the form, be sure to submit it to the appropriate department or person in your organization. This will ensure that all your requested changes are processed without delay. It’s best to keep a copy for your records and confirm that the changes have been made.
What You Should Know About This Form
What is the Gn 80124 Cg form used for?
The Gn 80124 Cg form, often referred to as the Humana Employee Change Form, is designed for employees to initiate changes to their benefits. This might include medical, dental, life insurance, or vision coverages. The form provides a structured way for employees to communicate their desired modifications, such as changing their primary care physician or adding dependents, making it easier for the employer to process these requests accurately.
Who needs to fill out the Gn 80124 Cg form?
This form should be completed by employees who wish to make changes to their existing benefits or enroll in new benefits offered by their employer. It can also be used by employees who need to report life events that affect their coverage, such as marriage, divorce, or the birth of a child. Any legal representatives acting on behalf of the employee may also fill it out.
How do I accurately fill out the Gn 80124 Cg form?
What information is required on the Gn 80124 Cg form?
The form requires various pieces of information, including the employee's full name, Social Security number, current and proposed benefit details, and the effective date for the changes. It also asks for qualifying events that may justify the requested changes, such as marriage or dependent changes. Information about any dependents being added or removed from coverage must also be included, along with their details.
Are there specific events that justify changes on the Gn 80124 Cg form?
Yes, there are several qualifying events that allow employees to make changes to their benefits. These include events such as marriage, divorce, or the birth or adoption of a child. Other situations, like a spouse’s employment changes or when a dependent becomes a full-time student, may also warrant adjustments. It's crucial to select the appropriate reason on the form to support your request.
Where do I submit the completed Gn 80124 Cg form?
The completed form should typically be submitted to the human resources department or the designated benefits administrator within your company. It’s advisable to check with your employer for specific submission guidelines. Keeping a copy of the completed form for personal records is also recommended, in case any issues arise during processing.
What should I do if I make a mistake on the Gn 80124 Cg form?
If a mistake is made on the form, it’s important to correct it before submission. You can cross out the incorrect information and write the correct details clearly. If the error is substantial or if it might cause confusion, consider starting over with a new form. Always review the completed form for accuracy to prevent any delays in processing your benefits changes.
Can someone else submit the Gn 80124 Cg form on my behalf?
Yes, a legal representative can submit the form on an employee's behalf, provided they sign it as the employee’s representative. The representative must also include their name and relationship to the employee on the form. Consent from the employee is usually assumed in this case, but it is good practice for the employee to inform human resources of the representation.
Common mistakes
Filling out the Gn 80124 Cg form correctly is essential for ensuring that your employee benefits are accurately updated. One common mistake is failing to print clearly. When information is difficult to read, it can lead to delays or errors in processing your changes. Using all capital letters can significantly improve clarity, so consider this method when filling out your information.
Another frequent error occurs in the section where individuals indicate a qualifying event. Some people neglect to provide the qualifying event date or choose an incomplete reason for the change. This information is crucial for processing benefit changes. Always ensure that the date of the event and the specific reason are both clearly noted.
Many individuals also overlook the importance of checking all relevant boxes. When selecting benefits or indicating changes, it’s vital to mark all applicable circles. Omitting a selection can result in benefits that need updating not being changed, which can lead to confusion later on.
In the section for dependent changes, many people make the mistake of failing to include Social Security numbers of dependents. This information is often required to verify identities and ensure accurate enrollment. Skipping this step can delay the processing of dependent changes, so be diligent about including all necessary details.
A fifth mistake individuals often make is not providing comprehensive address information. When updating an address, ensure that you complete each section, including city, state, and zip code. Incomplete address details can lead to important documents or notifications being sent to the wrong location.
Lastly, people sometimes forget to complete the signature section of the form. A signature is a vital component of the submission process. The form will not be processed without an employee or legal representative signature and the date of signing. Always double-check to confirm that you have signed and dated the document before submission.
Documents used along the form
The GN 80124 CG form, known as the Humana Employee Change Form, is a vital document that facilitates updates to employee benefits. Along with this form, several other documents may be required to ensure a smooth transition. Below is a list of commonly associated documents that often accompany the GN 80124 CG form.
- Employee Benefits Enrollment Form: This form allows employees to enroll in or make changes to their benefits during the enrollment period. It typically includes options for medical, dental, and vision plans.
- Dependent Verification Documentation: This includes documents that confirm the eligibility of dependents for coverage, such as birth certificates or adoption papers. Verification ensures that only qualified dependents receive benefits.
- Qualifying Event Notice: This document details the qualifying event that triggers a change in benefits, such as marriage, divorce, or the birth of a child. It serves as a key piece of information for processing changes.
- Life Insurance Beneficiary Designation Form: This form designates primary and secondary beneficiaries for life insurance policies. It is crucial for confirming who will receive benefits in the event of the employee's passing.
- Address Change Form: A separate form may be necessary for updating an employee's address. This ensures that all communications and benefits information are sent to the correct location.
- Health Savings Account (HSA) Enrollment Form: When employees elect to participate in an HSA, this form must be completed to set up their account and start contributions.
These documents, in conjunction with the GN 80124 CG form, help ensure that benefit changes are processed accurately and efficiently. It’s important to gather all necessary paperwork to avoid delays and ensure your benefits are updated without issues.
Similar forms
When updating employee benefits through the GN 80124 CG form, it can be helpful to understand documents that have a similar purpose or structure. Here are eight documents that share similarities with the GN 80124 CG form:
- Employee Benefits Enrollment Form: This form is used for enrolling in or changing employee benefits. It captures personal details, selections for various benefits, and qualifying events, much like the GN 80124 CG.
- Dependent Change Form: Like the GN 80124 CG, this document allows employees to update information about their dependents, including name changes and qualifying events that affect benefits eligibility.
- Medical Coverage Change Form: This form facilitates changes to an employee's medical coverage. It requests similar information about benefit classifications and effective dates, paralleling the structure of the GN 80124 CG.
- Beneficiary Change Form: Much like the GN 80124 CG form, this document allows employees to update or specify beneficiaries for various benefits, ensuring that essential information is captured for financial protection.
- Life Insurance Change Form: This form specifically addresses modifications to life insurance coverage. It shares a similar layout and purpose, asking for beneficiary information and coverage adjustments.
- Address Change Form: Required for updating personal contact information, this document serves a purpose akin to that of the GN 80124 CG by ensuring that benefits-related communication is directed correctly.
- Flexible Spending Account (FSA) Enrollment Form: This form enables employees to enroll in or modify their FSA contributions. It requests pertinent personal details and benefits options, similar to the GN 80124 CG.
- COBRA Election Form: This document allows employees to elect continued health coverage under COBRA. It contains essential information about qualifying events and timelines, mirroring the detail provided in the GN 80124 CG.
Each of these documents plays a crucial role in managing employee benefits and ensuring that changes are handled appropriately. Understanding their similarities can streamline the process for employees as they navigate their options.
Dos and Don'ts
Do's:
- Carefully read the instructions before filling out the form.
- Print clearly in all sections to ensure legibility.
- Provide complete information for all required fields.
- Double-check that all applicable circles are filled in correctly.
Don'ts:
- Do not leave any required fields blank.
- Avoid using corrections fluid or tape; instead, cross out errors neatly.
- Do not submit the form without your signature.
- Do not forget to indicate the qualifying event, if applicable.
Misconceptions
Understanding the GN 80124 CG form can be complex. Here are seven common misconceptions to clarify its purpose and usage:
- Misconception 1: The form is only for cancelling coverage.
In reality, it serves multiple functions, including changes to medical, dental, and other benefits. - Misconception 2: It can only be filled out online.
This form can be printed and filled out manually as well, making it accessible for all employees. - Misconception 3: You can skip portions of the form if you don’t have changes.
Every section should be filled out as applicable, even if it means marking 'no change' where necessary. - Misconception 4: The signature requirement is optional.
Submitting the form without a signature may lead to delays in processing your requests. - Misconception 5: Only HR can submit this form.
Employees are empowered to submit the completed form themselves, ensuring their information is up-to-date. - Misconception 6: There are no deadlines for submission.
It is important to submit the form promptly to ensure changes coincide with qualifying events and deadlines outlined by the company. - Misconception 7: The form is only for employee changes.
It also allows for changes related to dependents, so families can be accounted for in the benefits plan.
By staying informed and addressing these misconceptions, you can better navigate the requirements of the GN 80124 CG form.
Key takeaways
Filling out the GN 80124 CG form correctly is essential to ensure that your employee benefits are updated promptly. Here are nine key takeaways regarding this form:
- Print Clearly: It is important to print all information clearly. This helps to avoid any confusion or errors in processing your changes.
- Fill Applicable Circles: Make sure to fill in all applicable circles next to the employee changes you are requesting.
- Effective Date: Specify the proposed effective date for the changes. This date is vital for initiating or updating coverage.
- Qualifying Events: Indicate the reason for your changes based on qualifying events, such as marriage or a dependent birth, as this might affect eligibility.
- Dependent Information: If changes apply to dependents, complete the dependent sections thoroughly. Include their full names and social security numbers.
- Beneficiaries: Update beneficiary information for life insurance benefits, ensuring you provide accurate names and relationships.
- Contact Information: Provide your current email address and phone number. This allows for better communication regarding your application status.
- Signature Requirement: Include your signature at the bottom of the form. This shows you verify the provided information is accurate and complete.
- Submission Process: After completing the form, ensure it is submitted via the appropriate channel to avoid any delays in processing your changes.
Taking the time to carefully fill out the GN 80124 CG form will help to ensure that any changes to your employee benefits are processed efficiently and effectively. Always double-check your information before submitting.
Browse Other Templates
School Function Assessment Pdf - The School Function Assessment form is designed to evaluate the functional performance of students in a school setting.
Colorado Sales Tax Refund 2024 - Service fees are calculated based on the net tax due and must be claimed correctly.
Veterans Driver's License - The application requires a signature from both the applicant and the county representative.