Fill Out Your H1836 A Form
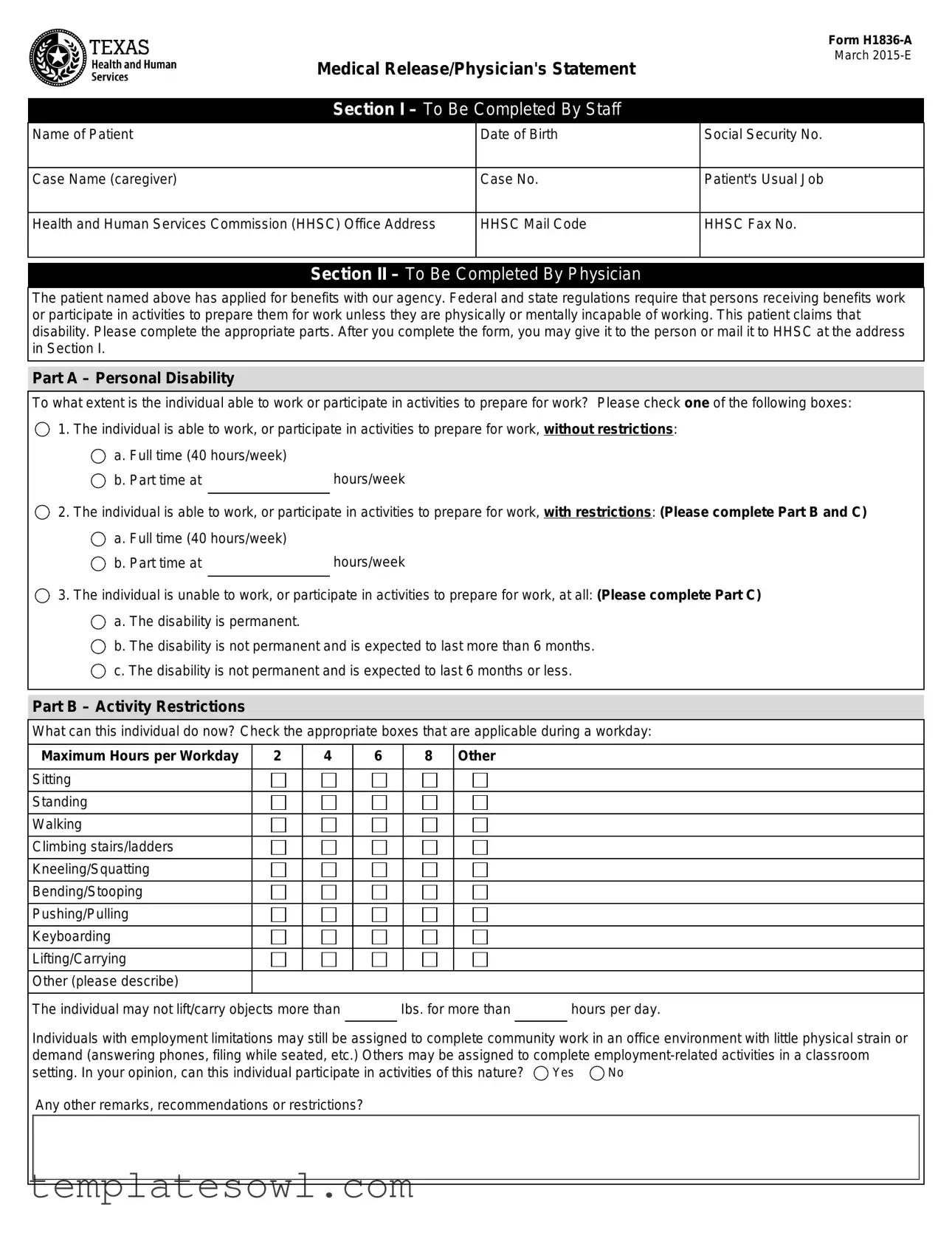
The H1836 A form, known as the Medical Release/Physician's Statement, serves a vital purpose in the assessment of an individual's eligibility for various state benefits, particularly for those unable to work due to medical conditions. This form, designed to gather essential medical information, includes sections that must be completed by both agency staff and the individual's physician. The first section requires details such as the patient's name, date of birth, and case information, which help to identify the applicant and their specific case within the Health and Human Services Commission (HHSC). In the subsequent section, the physician evaluates the individual's ability to work or engage in preparatory activities, providing critical information about any personal disabilities the individual may claim. Physicians are tasked with checking relevant restrictions and outlining the patient's capability in a structured format that includes specific limitations on work activities. Finally, the patient or their representative must provide authorization for the release of medical information, allowing HHSC to verify the stated conditions with healthcare providers. Importantly, signing this form is necessary for those seeking exemptions from the employment services program, ensuring that individual health details remain protected under privacy regulations while facilitating access to essential benefits.
H1836 A Example
Medical Release/Physician's Statement
Form
March
Section I – To Be Completed By Staff
Name of Patient |
Date of Birth |
Social Security No. |
|
|
|
Case Name (caregiver) |
Case No. |
Patient's Usual Job |
|
|
|
Health and Human Services Commission (HHSC) Office Address |
HHSC Mail Code |
HHSC Fax No. |
|
|
|
Section II – To Be Completed By Physician
The patient named above has applied for benefits with our agency. Federal and state regulations require that persons receiving benefits work or participate in activities to prepare them for work unless they are physically or mentally incapable of working. This patient claims that disability. Please complete the appropriate parts. After you complete the form, you may give it to the person or mail it to HHSC at the address in Section I.
Part A – Personal Disability
To what extent is the individual able to work or participate in activities to prepare for work? Please check one of the following boxes:
1. The individual is able to work, or participate in activities to prepare for work, without restrictions:
a. Full time (40 hours/week) |
|
b. Part time at |
hours/week |
2. The individual is able to work, or participate in activities to prepare for work, with restrictions: (Please complete Part B and C)
a. Full time (40 hours/week) |
|
b. Part time at |
hours/week |
3. The individual is unable to work, or participate in activities to prepare for work, at all: (Please complete Part C)
a. The disability is permanent.
b. The disability is not permanent and is expected to last more than 6 months.
c. The disability is not permanent and is expected to last 6 months or less.
Part B – Activity Restrictions
What can this individual do now? Check the appropriate boxes that are applicable during a workday:
Maximum Hours per Workday |
2 |
4 |
6 |
8 Other |
Sitting
Standing
Walking
Climbing stairs/ladders
Kneeling/Squatting
Bending/Stooping
Pushing/Pulling
Keyboarding
Lifting/Carrying
Other (please describe)
The individual may not lift/carry objects more than Ibs. for more than hours per day.
Individuals with employment limitations may still be assigned to complete community work in an office environment with little physical strain or demand (answering phones, filing while seated, etc.) Others may be assigned to complete
setting. In your opinion, can this individual participate in activities of this nature? |
Yes |
No |
Any other remarks, recommendations or restrictions?
Form
|
|
|
|
Page 2 / |
|
|
|
|
|
Part C – Diagnosis |
|
|
|
|
Primary Disabling Diagnosis |
|
|
Secondary Disabling Diagnosis |
|
|
|
|
|
|
Comments |
|
|
|
|
|
|
|
|
|
Name of Physician (please type or print) |
Signature – Physician |
Date |
||
|
|
|
|
|
Physicians License No. |
Office Address (Street or P.O. Box, City, State and ZIP) |
Area Code and Phone No. |
||
|
|
|
|
|
Section III – To Be Completed By Patient or Patient's Personal Representative
Authorization to Release Medical Information
Patient's Name:
HHSC is requesting verification of the medical condition that prevents you from participating in the employment services program. When you sign this authorization, you are giving HHSC permission to contact your doctors, medical facilities or other health care providers to request copies of your health information as indicated below. You do not have to sign this form to be eligible for TANF, SNAP, or Medicaid. However, you must sign this form if you want to be eligible for an exemption from the employment services program.
I authorize |
|
to complete Form |
|
|
|
|
Doctor, Medical Facilities or other Health Care Providers |
release the information to HHSC and the Texas Workforce Commission for purposes of verifying the medical condition that prevents me from
participating fully in the employment services program. This authorization expires on |
. |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Client or Personal Representative's Signature |
|
|
|
Date |
If you are signing for the client, please describe your authority to act for the client: |
|
|
|
|
|
Note: If the person requesting the release of case information cannot sign his/her name, two witnesses to his/her mark (X) must sign below:
Witness |
Date |
Witness |
Date |
Notice to Client
HHSC, as receiver of this information, will protect your personal health information in accordance with federal and state privacy regulations. If you authorize release of your health information to other parties, it may no longer be protected by privacy regulations.
You can withdraw permission you have given your doctor or health care provider to use or disclose health information that identifies you, unless they have already taken action based on your permission. You must withdraw your permission in writing.
Form Characteristics
| Fact Name | Details |
|---|---|
| Form Title | The official title of the form is "Medical Release/Physician's Statement Form H1836-A." |
| Creation Date | This form was created in March 2015, indicating its relevance for that period and beyond. |
| Section Allocation | The form is divided into three main sections: staff completion, physician completion, and patient or representative completion. |
| Patient Information | Section I requires the patient's name, date of birth, and social security number to identify the individual. |
| Physician's Role | In Section II, the physician evaluates the patient's work capacity and any disabilities that may limit their ability to work. |
| Disability Assessment | The form outlines categories for disability: able to work without restrictions, able to work with restrictions, and unable to work at all. |
| Authorization for Information Release | In Section III, patients must authorize the release of their medical information to the Health and Human Services Commission (HHSC). |
| Privacy Protection | The HHSC ensures that personal health information is protected according to federal and state privacy regulations. |
Guidelines on Utilizing H1836 A
The H1836 A form is a critical document necessary for medical verification when applying for certain benefits. Filling it out accurately ensures that the necessary parties have the information required to process your application. The following steps outline the process of completing this form efficiently and correctly.
- Section I - Staff Information:
- Enter the Name of Patient.
- Provide the Date of Birth.
- Input the Social Security Number.
- List the Case Name (caregiver).
- Complete the Case Number.
- Detail Patient's Usual Job.
- Fill in the Health and Human Services Commission (HHSC) Office Address.
- Include the HHSC Mail Code.
- Provide the HHSC Fax Number.
- Section II - Physician's Information:
- Indicate the extent to which the individual is able to work or participate in activities.
- If applicable, complete Part A with the individual’s work capability.
- For individuals with restrictions, proceed to Part B, detailing Activity Restrictions.
- In Part B, check all applicable activities and maximum hours per workday allowed.
- In Part C, specify the primary and secondary disabling diagnoses.
- Provide your name and signature.
- Complete the date, license number, office address, and contact information.
- Section III - Patient Information:
- Write the Patient's Name at the top of the section for authorization.
- Fill in who is authorized to release the medical information.
- State the expiration date for the authorization.
- Obtain the signature of the client or personal representative, along with the date.
- If needed, provide details about the authority to act for the client.
- If applicable, two witnesses must sign if the client cannot sign their name.
After completing the above steps, review all entered information for accuracy and clarity. The form can then be submitted directly by handing it to the individual responsible or mailed to the specified HHSC address in Section I. Timely submission will facilitate the processing of your application and any necessary evaluations regarding medical conditions as they relate to eligibility for services.
What You Should Know About This Form
What is the purpose of the H1836 A form?
The H1836 A form serves as a Medical Release and Physician's Statement required by the Health and Human Services Commission (HHSC) for individuals applying for benefits. Its primary purpose is to gather necessary medical information that determines an individual's capability to work or participate in employment-related activities. This information is crucial for assessing eligibility for various assistance programs.
Who is responsible for completing the H1836 A form?
The form has specific sections designated for completion by staff, physicians, and patients or their personal representatives. Staff members fill out the initial patient information. Physicians provide a detailed assessment of the individual's disability, including their ability to work and any restrictions. Finally, the patient or their representative must authorize the release of medical information.
What types of disabilities are addressed in the H1836 A form?
The H1836 A form inquires about personal disabilities and categorizes them into three main areas: individuals who can work without restrictions, those who can work with restrictions, and those who are unable to work at all. Specific details regarding the nature of the disability, whether it is primary or secondary, must also be provided by the physician. This thorough documentation assists in accurately determining the applicant's eligibility for assistance programs.
Is it mandatory to sign the H1836 A form?
Signing the H1836 A form is not mandatory for eligibility for TANF, SNAP, or Medicaid. However, individuals must sign the form if they wish to be considered for an exemption from the employment services program. This signature authorizes HHSC to verify medical conditions by contacting healthcare providers, which is critical for the exemption process.
How does the H1836 A form protect an individual's privacy?
The form includes a notice to clients that HHSC will protect personal health information in accordance with federal and state privacy regulations. Although the form allows for the release of medical information to HHSC and the Texas Workforce Commission, clients are informed that their data will be safeguarded. Additionally, individuals have the right to withdraw their authorization for the release of information at any time, although this must be done in writing.
Common mistakes
Filling out the H1836 A form can be challenging, and mistakes can delay your application process. Understanding common pitfalls can help ensure you complete the form correctly. Here are five mistakes often made when filling out this important document.
One common error is failing to provide complete and accurate patient information in Section I. This includes the patient's name, date of birth, and social security number. Omitting or incorrectly entering this information can lead to significant delays since the information is crucial for identifying the patient and processing the request. It's best to double-check this section to ensure all details are correct before submitting the form.
Another frequent mistake occurs in Section II, where physicians must assess the patient’s ability to work or participate in activities. Some physicians either check the wrong box or leave this section incomplete. It’s important to provide specific details about the patient's capability. If the doctor indicates that the patient is unable to work, it is critical to specify the nature and duration of the disability. Not doing so can result in the application being returned for additional information.
Many individuals fail to accurately complete Part B, which details activity restrictions. The instructions ask for specific types of physical capabilities, such as sitting, standing, or lifting. A common mistake is either overestimating what the patient can do or providing vague responses, such as "some" or "a little." Instead, be as precise as possible to provide a clear understanding of the patient's limitations during a workday.
Section III is often where people overlook the importance of the authorization to release medical information. Some patients forget to sign the authorization portion or fill in the expiration date. This section is crucial as it allows HHSC to verify the patient's medical condition and determine eligibility for benefits. Without a proper signature and date, the application may not be processed.
Lastly, individuals sometimes neglect to check whether the form has been signed by the physician. Incomplete signatures can lead to a significant lag in processing as HHSC will likely require further validation. It's always a good idea to ensure that all necessary signatures are present and legible before submitting the form. Taking these simple steps can facilitate a smoother application process and help avoid unnecessary complications.
Documents used along the form
The H1836 A form, or Medical Release/Physician's Statement Form, serves a crucial role in determining an individual’s capacity to work and participate in employment services. When applying for benefits, several accompanying forms and documents may be necessary to ensure a comprehensive evaluation of the applicant's medical condition. Below is a list of common documents often used in conjunction with the H1836 A form.
- Authorization for Release of Medical Information: This document grants health care providers permission to share relevant medical history with the agency to assess the extent of the applicant’s disability.
- Disability Verification Form: Often required by agencies, this form certifies that a medical professional has evaluated the individual’s disability and supports their application for benefits.
- Employment History Verification: This form provides a record of the applicant’s previous employment, including job descriptions and duties, to evaluate abilities in the context of their alleged disability.
- Client Service Plan: Created by social services, this document outlines the support and services needed for the individual based on their unique circumstances, including recommendations for vocational training or assistance.
- Psycho-social Evaluation Report: A report completed by a mental health professional assessing the psychological aspects of a client’s disability can assist in understanding the total impact on their capacity to work.
- Work Capacity Assessment: This evaluation determines an individual’s functional abilities related to job tasks, helping to identify any limitations due to their medical condition.
Understanding these accompanying forms is important for applicants navigating the benefits application process. Each document plays a specific role in providing evidence and context regarding the individual’s capacity to work, ultimately aiding in a fair assessment of their situation.
Similar forms
- Medical History Form: Like the H1836-A form, a Medical History Form gathers essential information about a patient’s health status. Both documents serve to inform medical professionals about a patient's past conditions and limiting factors that might affect their ability to participate in work or training programs.
- Physician's Assessment Form: The Physician's Assessment Form, similar to H1836-A, is completed by a physician and provides an evaluation of a patient's health abilities. Each form requires the physician's insights on the patient’s capability to work or prepare for work and includes disability classifications.
- Disability Certification Form: This document certifies an individual’s disability status for various programs, much like the H1836-A form. It details the nature of the disability and verifies if the individual is eligible for support due to their inability to work.
- Employment Ability Assessment: Similar to the H1836-A, this assessment form examines an individual's readiness to work and outlines any restrictions. Both forms require information on the patient's daily activities and physical limitations, helping agencies determine appropriate placement.
- Informed Consent for Treatment: While primarily concerned with treatment, the Informed Consent form shares a common theme with the H1836-A by focusing on patient rights and the release of medical information. Both forms require patient approval for health care providers to share details necessary for evaluating eligibility for assistance or programs.
Dos and Don'ts
When filling out the H1836 A form, it’s essential to follow guidelines to ensure it’s completed correctly. Here’s a list of recommendations:
- Do provide accurate and complete information regarding the patient’s personal details, including the name, date of birth, and social security number.
- Do clearly describe the patient's disability, ensuring that all relevant sections are filled out according to the physician's assessment.
- Do sign and date the authorization section if you are the patient or the patient’s representative.
- Do provide the physician’s information, including their license number and office address, to facilitate verification of the medical condition.
- Don’t leave any section incomplete. Each part of the form is necessary for it to be processed correctly.
- Don’t forget to keep a copy of the completed form for your records before submitting it to HHSC.
Misconceptions
Misconceptions about the H1836-A form can lead to confusion when applying for benefits. Here are nine common misunderstandings explained:
- The form is only for those with permanent disabilities. Many believe the H1836-A is exclusive to individuals with permanent disabilities. In reality, it accommodates various conditions, including temporary disabilities lasting more than six months.
- Signing the form means automatic approval. Some assume that completing the H1836-A guarantees benefits. However, approval depends on the assessment of the provided medical information.
- There’s no need for physician input. A common myth is that the patient can fill out the form independently. A physician's assessment is essential to validate the patient's claimed disability.
- Once signed, the authorization cannot be revoked. This misconception might discourage patients. In fact, individuals can withdraw their permission to disclose health information at any time by providing written notice.
- The form is only necessary for TANF applicants. Some people think only Temporary Assistance for Needy Families (TANF) applicants need to complete this form. However, it's required for various assistance programs, including SNAP and Medicaid, if seeking exemptions from employment services.
- All medical information is automatically shared with other parties. There is a concern that signing the H1836-A allows unrestricted access to one's medical records. In truth, only information necessary to verify the medical condition is shared with specified agencies.'
- People can’t work at all if they fill out this form. Many assume that completing the H1836-A eliminates their ability to work. The form actually assesses varying degrees of capability, including part-time or modified work.
- There’s only one way to complete the form. Individuals believe there’s only one method for submitting the H1836-A. In fact, the form can be handed directly to the physician or mailed to the designated health services address.
- There are no limits on how long it takes to process the form. Some individuals believe there's no urgency in submitting the H1836-A. Timely submission is crucial as delays can impact benefit eligibility.
Key takeaways
Here are the key takeaways for filling out and using the H1836 A form:
- Accurate Information: Ensure all patient details, including the name, date of birth, and Social Security number, are filled out correctly in Section I.
- Physician's Input: Section II must be completed by the physician. Their assessment is crucial in determining the patient's ability to work or participate in work-related activities.
- Work Capability Assessment: The physician should check the appropriate boxes regarding the patient's ability to work, indicating whether they can work full-time, part-time, or not at all.
- Detail Activity Restrictions: Be specific in Part B about what the patient can and cannot do during a workday. Mention any limitations on physical activities such as lifting or standing.
- Diagnosis Documentation: The physician must provide information regarding the primary and any secondary disabling diagnoses in Part C.
- Patient's Authorization: The patient or their representative needs to provide authorization for release of medical information. This is necessary for HHSC to verify the patient's medical condition.
- Privacy Protection: Understand that personal health information is protected under federal and state regulations. If health information is shared with other parties, it may not remain protected.
Browse Other Templates
Asbestos License Application,Asbestos Handling Permit,New York State Asbestos Certification,Asbestos Management License,Asbestos Work Authorization,Asbestos Handling Registration,NYS Asbestos Handler Form,Asbestos Contractor License Application,Licen - Applicants need to give their Federal Employment Identification Number.
Hvcc Appraisal - This form provides a record of lender certification regarding appraisal compliance with established guidelines.
Af Imt 220 - The personal data provided must be accurate to avoid issues during processing.