Fill Out Your Hcfa 1500 Form
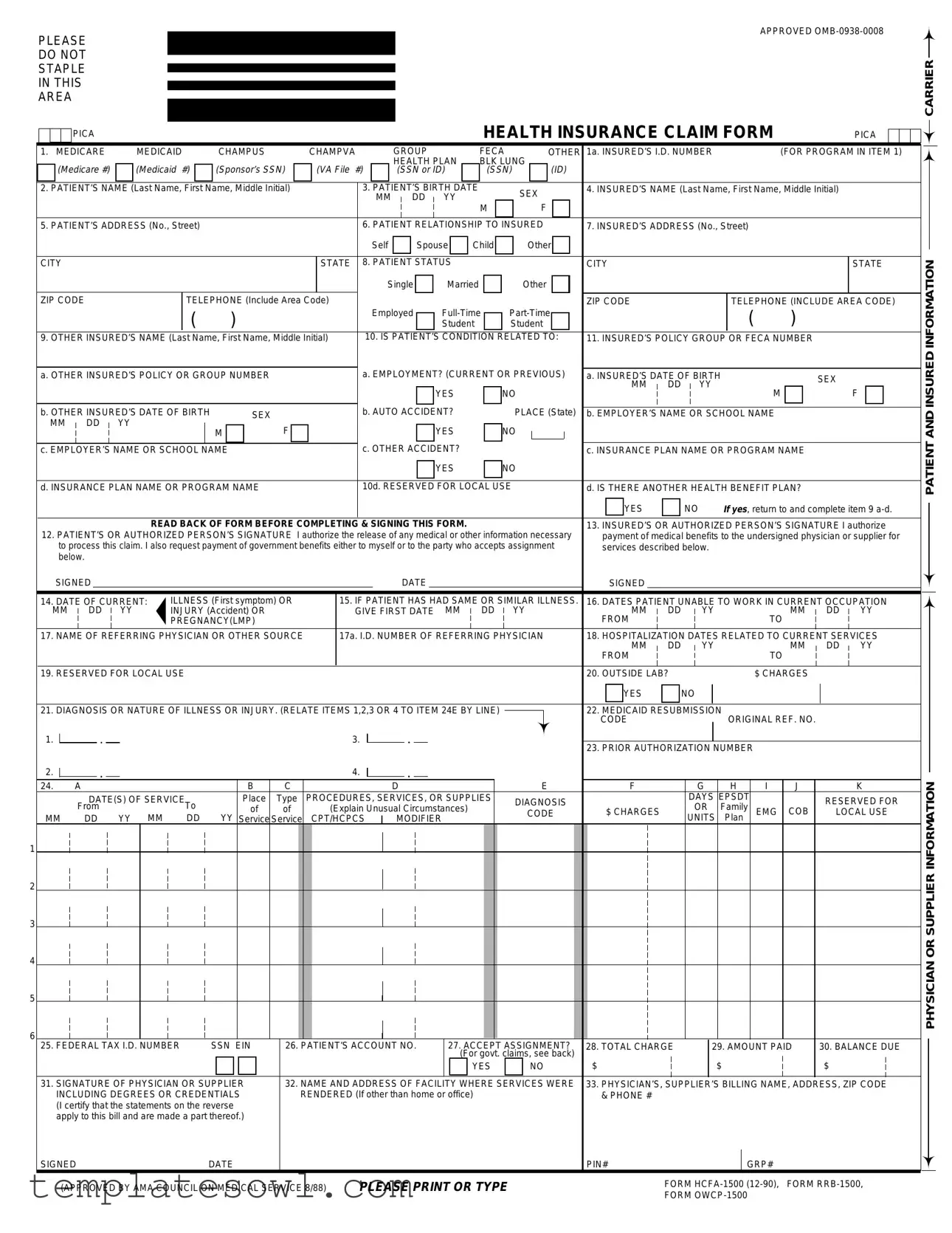
The HCFA 1500 form serves as a crucial tool in the healthcare system, providing a standardized way for healthcare providers to submit claims for reimbursement to insurance companies and government programs such as Medicare and Medicaid. It is designed to capture a wide range of information essential for processing medical claims, ensuring that both patients and providers navigate the often complex world of health insurance with relative ease. This form includes details such as the patient's identification, the insured person's information, the nature of the illness or injury, and the services rendered, all of which help in determining eligibility for benefits. Additionally, sections of the form address other insurance coverage that might relate to the claim, ensuring that all avenues for payment are explored. With clear instructions and structured data fields, the HCFA 1500 form facilitates a smoother claims process, while also serving as a legal document, as both the patient and the provider must certify the accuracy of the information provided. By understanding the components and function of the HCFA 1500 form, patients and providers can ensure accurate claims submission and timely reimbursement, ultimately contributing to better healthcare delivery and financial management within the medical field.
Hcfa 1500 Example
APPROVED
PLEASE
DO NOT
STAPLE
IN THIS
AREA
|
|
|
|
|
PICA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HEALTH INSURANCE CLAIM FORM |
|
|
|
PICA |
|
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
|
1. MEDICARE |
|
|
|
MEDICAID |
|
CHAMPUS |
|
|
CHAMPVA |
GROUP |
|
|
|
|
|
|
|
FECA |
OTHER |
1a. INSURED’S I.D. NUMBER |
|
|
|
|
(FOR PROGRAM IN ITEM 1) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HEALTH PLAN |
|
|
|
BLK LUNG |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
(Medicare #) |
|
|
|
(Medicaid |
#) |
|
|
(Sponsor’s SSN) |
|
(VA File |
#) |
|
|
|
|
(SSN or ID) |
|
|
|
|
(SSN) |
|
(ID) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
2. PATIENT’S NAME (Last Name, First Name, Middle Initial) |
|
|
|
|
3. PATIENT’S BIRTH DATE |
|
|
SEX |
|
|
|
|
|
4. INSURED’S NAME (Last Name, First Name, Middle Initial) |
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MM |
|
|
|
DD |
|
|
YY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. PATIENT’S ADDRESS (No., Street) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. PATIENT RELATIONSHIP TO INSURED |
|
|
|
|
|
7. INSURED’S ADDRESS (No., Street) |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Self |
|
|
|
|
Spouse |
|
|
Child |
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE |
|
8. PATIENT STATUS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Single |
|
|
|
Married |
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
ZIP CODE |
|
|
|
|
|
|
|
TELEPHONE (Include Area Code) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ZIP CODE |
|
|
|
|
|
|
|
|
|
TELEPHONE (INCLUDE AREA CODE) |
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
Employed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
|
) |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Student |
|
|
Student |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
9. OTHER INSURED’S NAME (Last Name, First Name, Middle Initial) |
|
10. IS PATIENT’S CONDITION RELATED TO: |
11. INSURED’S POLICY GROUP OR FECA NUMBER |
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. EMPLOYMENT? (CURRENT OR PREVIOUS) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
a. OTHER INSURED’S POLICY OR GROUP NUMBER |
|
|
|
|
|
|
a. INSURED’S DATE OF BIRTH |
|
|
|
SEX |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MM |
DD |
|
|
|
YY |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
F |
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. OTHER INSURED’S DATE OF BIRTH |
|
|
|
|
|
SEX |
|
|
|
|
|
|
b. AUTO ACCIDENT? |
|
|
|
|
|
PLACE (State) |
b. EMPLOYER’S NAME OR SCHOOL NAME |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
MM |
|
DD |
|
YY |
|
|
|
|
|
M |
|
|
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. EMPLOYER’S NAME OR SCHOOL NAME |
|
|
|
|
|
|
c. OTHER ACCIDENT? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. INSURANCE PLAN NAME OR PROGRAM NAME |
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
d. INSURANCE PLAN NAME OR PROGRAM NAME |
|
|
|
|
|
|
10d. RESERVED FOR LOCAL USE |
|
|
|
|
|
d. IS THERE ANOTHER HEALTH BENEFIT PLAN? |
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
|
NO |
If yes, return to and complete item 9 |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
READ BACK OF FORM BEFORE COMPLETING & SIGNING THIS FORM. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. INSURED’S OR AUTHORIZED PERSON’S SIGNATURE I authorize |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
12. PATIENT’S OR AUTHORIZED PERSON’S SIGNATURE I authorize the release of any medical or other information necessary |
payment of medical benefits to the undersigned physician or supplier for |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
to process this claim. I also request payment of government benefits either to myself or to the party who accepts assignment |
services described below. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
below. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
SIGNED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIGNED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14. DATE OF CURRENT: |
|
ILLNESS (First symptom) OR |
|
|
15. IF PATIENT HAS HAD SAME OR SIMILAR ILLNESS. |
16. DATES PATIENT UNABLE TO WORK IN CURRENT OCCUPATION |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
MM |
|
DD |
|
|
YY |
|
INJURY (Accident) OR |
|
|
|
|
|
GIVE FIRST DATE |
|
|
MM |
|
DD |
|
|
YY |
|
|
|
|
|
|
|
MM |
DD |
|
|
|
YY |
|
|
|
|
|
MM |
DD |
YY |
||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PREGNANCY(LMP) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM |
|
|
|
|
|
|
|
|
|
|
|
|
TO |
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
17. NAME OF REFERRING PHYSICIAN OR OTHER SOURCE |
|
|
17a. I.D. NUMBER OF REFERRING PHYSICIAN |
|
|
|
|
|
18. HOSPITALIZATION DATES RELATED TO CURRENT SERVICES |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MM |
DD |
|
|
|
YY |
|
|
|
|
|
MM |
DD |
YY |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM |
|
|
|
|
|
|
|
|
|
|
|
|
TO |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19. RESERVED FOR LOCAL USE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. OUTSIDE LAB? |
|
|
|
|
|
|
|
|
|
|
$ CHARGES |
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. DIAGNOSIS OR NATURE OF ILLNESS OR INJURY. (RELATE ITEMS 1,2,3 OR 4 TO ITEM 24E BY LINE) |
|
|
|
|
|
|
|
|
|
|
|
|
|
22. MEDICAID RESUBMISSION |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CODE |
|
|
|
|
|
|
|
|
|
ORIGINAL REF. NO. |
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
23. PRIOR AUTHORIZATION NUMBER |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
24. |
|
|
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
C |
|
|
|
|
|
|
|
|
|
D |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
F |
|
|
|
|
|
G |
|
H |
|
I |
J |
|
K |
||||||||||||||||||||
|
|
|
|
|
|
DATE(S) OF SERVICE |
|
|
|
|
Place |
|
Type |
PROCEDURES, SERVICES, OR SUPPLIES |
|
|
DIAGNOSIS |
|
|
|
|
|
|
|
DAYS |
EPSDT |
|
|
|
|
RESERVED FOR |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
MM |
|
From |
|
YY |
MM |
To |
|
YY |
|
of |
|
|
of |
|
(Explain Unusual Circumstances) |
|
|
|
|
|
|
CODE |
|
$ CHARGES |
|
|
|
|
|
OR |
Family |
|
EMG |
COB |
LOCAL USE |
||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
DD |
|
DD |
|
Service |
Service |
CPT/HCPCS |
|
|
MODIFIER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UNITS |
Plan |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
25. FEDERAL TAX I.D. NUMBER |
|
|
|
SSN EIN |
|
26. PATIENT’S ACCOUNT NO. |
|
|
27. ACCEPT ASSIGNMENT? |
28. TOTAL CHARGE |
|
|
|
|
29. AMOUNT PAID |
30. BALANCE DUE |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(For govt. claims, see back) |
$ |
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
$ |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31. SIGNATURE OF PHYSICIAN OR SUPPLIER |
|
32. NAME AND ADDRESS OF FACILITY WHERE SERVICES WERE |
33. PHYSICIAN’S, SUPPLIER’S BILLING NAME, ADDRESS, ZIP CODE |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
INCLUDING DEGREES OR CREDENTIALS |
|
|
RENDERED (If other than home or office) |
|
|
|
|
|
|
|
|
|
|
|
|
|
& PHONE # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
(I certify that the statements on the reverse |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
apply to this bill and are made a part thereof.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
SIGNED |
|
|
|
|
|
|
|
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PIN# |
|
|
|
|
|
|
|
|
|
|
GRP# |
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
(APPROVED BY AMA COUNCIL ON MEDICAL SERVICE 8/88) |
|
PLEASE PRINT OR TYPE |
|
|
|
|
|
|
|
|
|
FORM |
FORM |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FORM |
|
|
|
|
|
|
|
|
|
|||||||||||
CARRIER
PATIENT AND INSURED INFORMATION
PHYSICIAN OR SUPPLIER INFORMATION
BECAUSE THIS FORM IS USED BY VARIOUS GOVERNMENT AND PRIVATE HEALTH PROGRAMS, SEE SEPARATE INSTRUCTIONS ISSUED BY APPLICABLE PROGRAMS.
NOTICE: Any person who knowingly files a statement of claim containing any misrepresentation or any false, incomplete or misleading information may be guilty of a criminal act punishable under law and may be subject to civil penalties.
REFERS TO GOVERNMENT PROGRAMS ONLY
MEDICARE AND CHAMPUS PAYMENTS: A patient’s signature requests that payment be made and authorizes release of any information necessary to process the claim and certifies that the information provided in Blocks 1 through 12 is true, accurate and complete. In the case of a Medicare claim, the patient’s signature authorizes any entity to release to Medicare medical and nonmedical information, including employment status, and whether the person has employer group health insurance, liability,
BLACK LUNG AND FECA CLAIMS
The provider agrees to accept the amount paid by the Government as payment in full. See Black Lung and FECA instructions regarding required procedure and diagnosis coding systems.
SIGNATURE OF PHYSICIAN OR SUPPLIER (MEDICARE, CHAMPUS, FECA AND BLACK LUNG)
I certify that the services shown on this form were medically indicated and necessary for the health of the patient and were personally furnished by me or were furnished incident to my professional service by my employee under my immediate personal supervision, except as otherwise expressly permitted by Medicare or CHAMPUS regulations.
For services to be considered as “incident” to a physician’s professional service, 1) they must be rendered under the physician’s immediate personal supervision by his/her employee, 2) they must be an integral, although incidental part of a covered physician’s service, 3) they must be of kinds commonly furnished in physician’s offices, and 4) the services of nonphysicians must be included on the physician’s bills.
For CHAMPUS claims, I further certify that I (or any employee) who rendered services am not an active duty member of the Uniformed Services or a civilian employee of the United States Government or a contract employee of the United States Government, either civilian or military (refer to 5 USC 5536). For
No Part B Medicare benefits may be paid unless this form is received as required by existing law and regulations (42 CFR 424.32).
NOTICE: Any one who misrepresents or falsifies essential information to receive payment from Federal funds requested by this form may upon conviction be subject to fine and imprisonment under applicable Federal laws.
NOTICE TO PATIENT ABOUT THE COLLECTION AND USE OF MEDICARE, CHAMPUS, FECA, AND BLACK LUNG INFORMATION
(PRIVACY ACT STATEMENT)
We are authorized by HCFA, CHAMPUS and OWCP to ask you for information needed in the administration of the Medicare, CHAMPUS, FECA, and Black Lung programs. Authority to collect information is in section 205(a), 1862, 1872 and 1874 of the Social Security Act as amended, 42 CFR 411.24(a) and 424.5(a) (6), and 44 USC 3101;41 CFR 101 et seq and 10 USC 1079 and 1086; 5 USC 8101 et seq; and 30 USC 901 et seq; 38 USC 613; E.O. 9397.
The information we obtain to complete claims under these programs is used to identify you and to determine your eligibility. It is also used to decide if the services and supplies you received are covered by these programs and to insure that proper payment is made.
The information may also be given to other providers of services, carriers, intermediaries, medical review boards, health plans, and other organizations or Federal agencies, for the effective administration of Federal provisions that require other third parties payers to pay primary to Federal program, and as otherwise necessary to administer these programs. For example, it may be necessary to disclose information about the benefits you have used to a hospital or doctor. Additional disclosures are made through routine uses for information contained in systems of records.
FOR MEDICARE CLAIMS: See the notice modifying system No.
FOR OWCP CLAIMS: Department of Labor, Privacy Act of 1974, “Republication of Notice of Systems of Records,” Federal Register Vol. 55 No. 40, Wed Feb. 28, 1990, See
FOR CHAMPUS CLAIMS: PRINCIPLE PURPOSE(S): To evaluate eligibility for medical care provided by civilian sources and to issue payment upon establishment of eligibility and determination that the services/supplies received are authorized by law.
ROUTINE USE(S): Information from claims and related documents may be given to the Dept. of Veterans Affairs, the Dept. of Health and Human Services and/or the Dept. of Transportation consistent with their statutory administrative responsibilities under CHAMPUS/CHAMPVA; to the Dept. of Justice for representation of the Secretary of Defense in civil actions; to the Internal Revenue Service, private collection agencies, and consumer reporting agencies in connection with recoupment claims; and to Congressional Offices in response to inquiries made at the request of the person to whom a record pertains. Appropriate disclosures may be made to other federal, state, local, foreign government agencies, private business entities, and individual providers of care, on matters relating to entitlement, claims adjudication, fraud, program abuse, utilization review, quality assurance, peer review, program integrity,
DISCLOSURES: Voluntary; however, failure to provide information will result in delay in payment or may result in denial of claim. With the one exception discussed below, there are no penalties under these programs for refusing to supply information. However, failure to furnish information regarding the medical services rendered or the amount charged would prevent payment of claims under these programs. Failure to furnish any other information, such as name or claim number, would delay payment of the claim. Failure to provide medical information under FECA could be deemed an obstruction.
It is mandatory that you tell us if you know that another party is responsible for paying for your treatment. Section 1128B of the Social Security Act and 31 USC 3801- 3812 provide penalties for withholding this information.
You should be aware that P.L.
MEDICAID PAYMENTS (PROVIDER CERTIFICATION)
I hereby agree to keep such records as are necessary to disclose fully the extent of services provided to individuals under the State’s Title XIX plan and to furnish information regarding any payments claimed for providing such services as the State Agency or Dept. of Health and Humans Services may request.
I further agree to accept, as payment in full, the amount paid by the Medicaid program for those claims submitted for payment under that program, with the exception of authorized deductible, coinsurance,
SIGNATURE OF PHYSICIAN (OR SUPPLIER): I certify that the services listed above were medically indicated and necessary to the health of this patient and were personally furnished by me or my employee under my personal direction.
NOTICE: This is to certify that the foregoing information is true, accurate and complete. I understand that payment and satisfaction of this claim will be from Federal and State funds, and that any false claims, statements, or documents, or concealment of a material fact, may be prosecuted under applicable Federal or State laws.
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including time for reviewing instructions, searching existing date sources, gathering and maintaining data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing the burden, to HCFA, Office of Financial Management, P.O. Box 26684, Baltimore, MD 21207; and to the Office of Management and Budget, Paperwork Reduction Project
Form Characteristics
| Fact Name | Details |
|---|---|
| Form Purpose | The HCFA 1500 form is used to submit health care claims for reimbursement from Medicare and other insurers. |
| Patient Information | The form requires detailed information about the patient, including name, address, and date of birth. |
| Insured Information | Details about the insured party must be included, such as relationship to the patient and insurance policy number. |
| Diagnosis Codes | Providers need to include diagnosis codes that relate to the services provided, ensuring accurate billing. |
| Signature Requirement | Both the patient and the physician must sign the form, authorizing the release of medical information for processing the claim. |
| State-Specific Forms | Each state may have variations of the HCFA 1500 form. Providers should refer to state-specific regulations for compliance. |
| Governing Laws | Claims submission must comply with federal laws, including regulations set forth in the Social Security Act and relevant state laws. |
Guidelines on Utilizing Hcfa 1500
Completing the HCFA 1500 form can seem overwhelming at first glance, but following a structured approach can simplify the process. This form is crucial for submitting health insurance claims, containing various sections that require specific information about patients, providers, and services rendered. Careful attention to accuracy and clarity is essential to ensure timely processing and payment.
- Read the instructions: Before diving in, take a few minutes to read any instructions that accompany the form. These will guide you through specific requirements based on the insurance program.
- Identify the type of insurance: In the top section, check the box for the type of insurance that applies to the insured, such as Medicare, Medicaid, or others.
- Input the insured's ID number: In the first box, enter the insured's identification number relevant to the insurance type indicated.
- Fill in the patient's name: Provide the patient's full name in the format of last name, first name, and middle initial.
- Add the patient's birth date: Enter the patient's birth date in the specified MM/DD/YY format along with the patient's sex.
- Provide patient and insured addresses: Include the patient's address and, if different, the insured's address. Make sure to write clearly and complete all address fields.
- Define the patient's relationship to the insured: Choose from options like self, spouse, child, or other.
- State the patient’s status: Indicate whether the patient is single, married, employed, or a student.
- List any other insured individuals: If applicable, provide information for any additional insured parties, including names and birth dates.
- Check if the patient’s condition is related to employment: Answer yes or no to indicate if the patient’s condition is related to their employment, auto accidents, or other accidents.
- Complete the insurance plan and policy details: Fill in the group number, policy number, and other required insurance details as needed.
- Add dates of service: In the appropriate section, enter the dates services were provided, ensuring they fall within the specified format.
- Detail procedures and charges: List the procedures performed, service codes, and the associated charges. Include all necessary descriptions to avoid any confusion.
- Confirm total charges and payments: Sum up the total charge for the services rendered, alongside any payments already made.
- Signatures: The patient and/or authorized person must provide their signature and date. In addition, the billing provider must sign and date the form, certifying that the information is accurate.
- Review the form: Before submitting, double-check all information for accuracy. Ensure there are no blank fields and that everything is clearly printed.
Taking the time to carefully complete each section of the HCFA 1500 form will greatly enhance the likelihood of a smooth claims process. This attention to detail can help prevent delays and facilitate prompt reimbursement for services rendered.
What You Should Know About This Form
What is the HCFA 1500 form used for?
The HCFA 1500 form, now known as the CMS-1500 form, is primarily used for billing and claiming medical services and supplies provided by healthcare professionals. It enables providers to submit claims to Medicare and other health insurance programs. This form assists in the processing of various claims, ensuring that patients receive the benefits they are entitled to under their health insurance policies.
Who needs to fill out the HCFA 1500 form?
This form must be filled out by healthcare providers when they want to receive payment for the services they have rendered. Physicians, therapists, and suppliers of medical equipment are typical users of the HCFA 1500 form. In addition, patients may need to provide information to ensure accurate billing and claims processing.
What information must be included in the HCFA 1500 form?
The HCFA 1500 form requires a variety of patient and service-related details. Some key fields include patient name, date of birth, insurance information, the date of service, and diagnosis codes. Additionally, signatures from both the patient and the provider are essential to authorize the release of medical information and claim processing.
How do I submit the HCFA 1500 form?
The HCFA 1500 form can be submitted either electronically or in paper format. For electronic submissions, healthcare providers often use specialized billing software or health information exchange systems. When submitting by paper, the completed form should be sent directly to the relevant insurance company or Medicare carrier. It's important to follow specific submission guidelines provided by the insurance entity.
What should I do if my claim is denied?
If a claim is denied, it is important to review the reason for the denial provided by the insurer. Providers can often appeal the decision by submitting additional information or documentation that may support the claim. Patients should also remain informed and can contribute by ensuring that all necessary information is accurate and complete on the original form, which may prevent future denials.
Are there any common mistakes to avoid when filling out the HCFA 1500 form?
Some common mistakes include omitting required information, using incorrect codes for diagnoses or procedures, and failing to obtain necessary signatures. These errors can delay processing times or lead to claim denials. It's crucial to double-check the form before submission to ensure it is filled out completely and accurately.
Is there a deadline for submitting the HCFA 1500 form?
Yes, there are deadlines for submitting the HCFA 1500 form that vary depending on the payer. Generally, claims must be submitted within a certain timeframe after the service is provided, often ranging from 90 to 180 days. Healthcare providers should familiarize themselves with the specific policies of each insurance company to ensure compliance and timely payment.
Common mistakes
Filling out the HCFA 1500 form can feel overwhelming, especially if it’s your first time. However, many common mistakes can lead to claim denials or delays. Let's explore five of those missteps.
One of the most frequent errors occurs in the patient's identification section. Mistakes like misspelling the patient’s name or incorrect birthdate can cause significant issues. Always double-check this information. Even a small typo can mean the difference between a successful claim and a rejected one.
Another common oversight is the insurance details. Entering incorrect policy numbers or failing to provide the correct identification numbers for both the patient and the insured is a mistake that can set back claims processing. Make sure to pull these details directly from the insurance card and verify them for accuracy.
Failing to answer all the relevant questions is also a pitfall many people fall into. For example, if the patient has insurance through a spouse or another employer, it must be clearly indicated. Leaving out this information may lead to unnecessary delays while insurers figure out who is responsible for payment.
In addition, some individuals mistakenly omit signatures. The form critical requires the patient's signature to authorize the release of information and payment. Forgetting this piece can halt the entire claims process. It’s a simple step but often overlooked in the rush to submit the paperwork.
Lastly, disregarding the submission guidelines can result in rejection. This includes failing to ensure the form is not stapled, using incorrect dates, or submitting illegible copies. Adhering to submission guidelines is essential; even minor deviations can lead to delays in payment or further complications.
By being mindful of these common mistakes, you can make the claim submission process smoother and increase your chances of timely payment. Careful attention to detail will serve you well when filling out the HCFA 1500 form.
Documents used along the form
The HCFA 1500 form is essential for healthcare providers when submitting claims for reimbursement from Medicare, Medicaid, and other insurance programs. However, several other forms and documents often complement this form to streamline the billing process and ensure appropriate payments. Below is a list of commonly used documents that may accompany the HCFA 1500 form.
- Notice of Admission (NOA): This document is usually required for inpatient services. It provides details about the patient’s admission to a healthcare facility and confirms the necessity of the services rendered.
- Prior Authorization Requests: Many insurance companies require prior authorization before certain procedures or services. This request outlines the medical necessity for the treatment and ensures coverage before the claim is submitted.
- Superbill: A superbill is a detailed document used by healthcare providers that lists the services performed for a patient. It includes diagnosis codes and procedure codes that help in accurate billing and claim submission.
- Patient History and Physical Exam (H&P): This document includes a summary of the patient's medical history and the results of their physical examination. It is important for substantiating the medical necessity of the services provided.
- Patient Consent Forms: These forms are essential for obtaining consent from patients for specific treatments or procedures. They serve as legal documentation that a patient has been informed about and agreed to the course of treatment.
- Explanation of Benefits (EOB): An EOB is a statement from an insurance company detailing what services were billed, what the insurance paid, and what the patient owes. It is often necessary for reconciling claims and addressing any underpayments.
Being familiar with these additional documents can significantly aid in the claims submission process, reducing potential delays in reimbursement. Proper organization and completeness of these documents alongside the HCFA 1500 form can enhance efficiency and ensure that patient claims are processed promptly and accurately.
Similar forms
The HCFA 1500 form is commonly used in healthcare for submitting claims. Several other documents serve similar purposes in different contexts. Here’s a list of six documents that share similarities with the HCFA 1500 form:
- UB-04 (CMS-1450): This form is used by hospitals and other healthcare facilities to bill for services. Like the HCFA 1500, it captures patient demographics, insurance information, and detailed service descriptions.
- CMS-1500 (Original HCFA 1500): This is the predecessor of the HCFA 1500 form. They both serve to submit medical claims for reimbursement, containing similar patient and provider information.
- Form RI-14 (Medicaid Claim Form): Specific to Medicaid billing, this form mimics the HCFA 1500 in that it requires similar details about patient eligibility and services provided for reimbursement purposes.
- Claim Form for Direct Pay (for Non-Participating Providers): Similar to the HCFA 1500, this form allows non-participating providers to submit claims directly to insurance companies, collecting essential patient and service information.
- Medicare Advantage Claim Form: This document is tailored for Medicare Advantage plans and shares the same structure as the HCFA 1500, requiring comprehensive patient information and service details for claims processing.
- Workers' Compensation Claim Form: Used for injuries sustained in the workplace, this form also collects details on the injured party and the medical services provided, much like the HCFA 1500 does for general medical claims.
Each of these forms plays a vital role in processing healthcare claims, ensuring consistent information is gathered to facilitate reimbursement from insurers.
Dos and Don'ts
When filling out the HCFA 1500 form, there are important best practices and common mistakes to avoid. The following lists include both:
- Do ensure that all fields are completed accurately.
- Do use clear and legible handwriting or type the information.
- Do double-check patient and insured details for correctness.
- Do sign and date the form where indicated.
- Don't leave any required fields blank.
- Don't use correction fluid on the form.
- Don't attach any additional documents unless instructed.
- Don't forget to check the specific requirements for the payer involved.
Misconceptions
Misconceptions about the HCFA 1500 form can lead to unnecessary confusion. Here are ten common misunderstandings, along with clarifications:
- Only doctors can submit the HCFA 1500 form. Many providers, such as hospitals and therapists, can also submit this form for reimbursement.
- The form is only for Medicare claims. In fact, the HCFA 1500 form is used for various private and government health programs, not solely Medicare.
- There is no need for patient information. Accurate patient information is essential for processing a claim effectively, including details such as date of birth and relationship to the insured.
- If a claim is denied, resubmitting the same form will work. It's often necessary to understand the reason for denial and make adjustments before resubmitting the claim.
- Only one signature is required. Both the patient and the provider (or authorized person) must sign the form to authorize release of information and payment.
- Completing the entire form is not necessary. Some items require completion based on the specific claim. Failing to provide necessary details can lead to delays.
- The form looks the same for everyone. Different health plans may have specific requirements or variations in how the form should be completed.
- Claim processing is immediate. In reality, it often takes several days for claims to be reviewed and processed by insurers.
- Additional documentation is never needed. Supporting documents such as diagnosis or procedure codes may be requested alongside the form to validate the claim.
- Submitting the form guarantees payment. Approval is contingent upon meeting all deadlines and criteria set by the insurance provider.
Understanding these misconceptions will help ensure a smoother process when using the HCFA 1500 form. Taking the time to accurately fill it out will facilitate prompt claims processing and payment.
Key takeaways
Filling out and utilizing the HCFA 1500 form is essential for healthcare providers to ensure proper billing and reimbursement from health plans. Here are key takeaways to consider when using this form:
- Accurate Patient Information: Provide complete and correct patient details, including name, address, and relationship to the insured. This information is critical for processing the claim efficiently.
- Identify the Insured: Clearly specify the insured individual’s name and details, particularly if the patient is not the insured. The relationship between the patient and the insured must also be stated.
- Condition Related Information: Indicate whether the patient’s condition is related to employment, accidents, or other circumstances. This determines how the claim is processed and the type of coverage applicable.
- Signatures Matter: Both the patient and the provider must sign the form. These signatures authorize the release of medical information required for claim processing, and they certify the accuracy of the provided information.
- Diagnosis Codes: Use appropriate diagnosis codes that reflect the patient’s condition. This helps the insurance provider determine the necessity of the services rendered.
- Keep Copies: Always retain a copy of the completed HCFA 1500 form for your records. This can be crucial for follow-up inquiries or disputes regarding the claim.
Browse Other Templates
Free Printable Daycare Receipt - This form is vital for dependent care tax credits.
Rosebud Sioux Tribe - The Oglala Sioux Tribe emphasizes the importance of accurate historical representation in requests.
How to Change Your Name in Pa - Specify the date the form is filled out and submitted.