Fill Out Your Head Toe Assessment Form
The Head to Toe Assessment form serves as a structured guideline for performing a comprehensive evaluation of a patient's physical and mental health status. This form facilitates a systematic approach, ensuring that healthcare practitioners assess critical elements like consciousness level, vital signs, and physical attributes of the patient, including their hair, skin, and nails. Acknowledging the importance of proper identification procedures, practitioners must confirm the patient’s identity using two forms of ID, along with reviewing any pertinent allergies. Gathering the necessary equipment before entering the patient’s space, such as stethoscopes, thermometers, and gloves, is essential. The assessment process itself not only involves checking for vital signs—blood pressure, pulse, respiratory rate—but also includes a detailed examination of various body systems, ensuring that all aspects are covered. The evaluator's signature reflects the practitioner's competency over multiple attempts and provides a framework for feedback and improvement. Through careful observation and documentation, the Head to Toe Assessment form validates nursing skills, promotes patient safety, and ensures that all critical behaviors are executed correctly. This careful structure empowers practitioners, enhances patient care, and ultimately supports the delivery of quality healthcare.
Head Toe Assessment Example
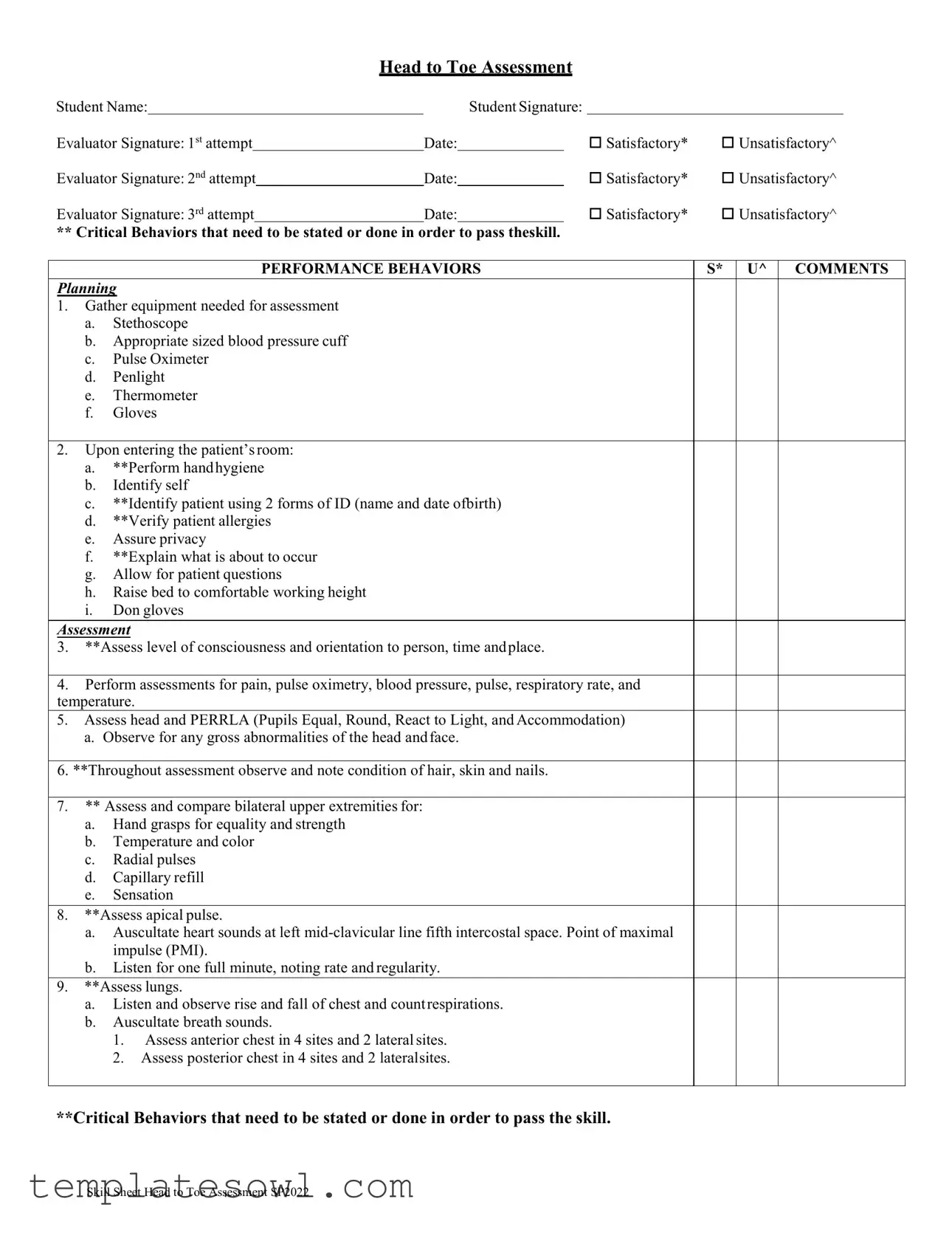
Head to Toe Assessment
Student Name: |
|
|
|
Student Signature: |
|
|
|
||
Evaluator Signature: 1st attempt |
|
|
Date: |
Satisfactory* |
Unsatisfactory^ |
||||
|
|
|
|
|
|
|
|
||
Evaluator Signature: 2nd attempt |
|
Date: |
Satisfactory* |
Unsatisfactory^ |
|||||
|
|
|
|
|
|
Satisfactory* |
Unsatisfactory^ |
||
Evaluator Signature: 3rd attempt |
|
|
Date: |
||||||
|
|
order |
|
|
|
|
|
||
** Critical Behaviors that need to be stated or done in |
to pass theskill. |
|
|
|
|||||
|
|
|
|
|
|
||||
|
|
|
PERFORMANCE BEHAVIORS |
|
S* U^ COMMENTS |
||||
Planning
1.Gather equipment needed for assessment
a.Stethoscope
b.Appropriate sized blood pressure cuff
c.Pulse Oximeter
d.Penlight
e.Thermometer
f.Gloves
2.Upon entering the patient’s room:
a.**Perform hand hygiene
b.Identify self
c.**Identify patient using 2 forms of ID (name and date ofbirth)
d.**Verify patient allergies
e.Assure privacy
f.**Explain what is about to occur
g.Allow for patient questions
h.Raise bed to comfortable working height
i.Don gloves
Assessment
3.**Assess level of consciousness and orientation to person, time and place.
4.Perform assessments for pain, pulse oximetry, blood pressure, pulse, respiratory rate, and temperature.
5.Assess head and PERRLA (Pupils Equal, Round, React to Light, and Accommodation)
a.Observe for any gross abnormalities of the head and face.
6.**Throughout assessment observe and note condition of hair, skin and nails.
7.** Assess and compare bilateral upper extremities for:
a.Hand grasps for equality and strength
b.Temperature and color
c.Radial pulses
d.Capillary refill
e.Sensation
8.**Assess apical pulse.
a.Auscultate heart sounds at left
b.Listen for one full minute, noting rate and regularity.
9.**Assess lungs.
a.Listen and observe rise and fall of chest and count respirations.
b.Auscultate breath sounds.
1.Assess anterior chest in 4 sites and 2 lateral sites.
2.Assess posterior chest in 4 sites and 2 lateralsites.
**Critical Behaviors that need to be stated or done in order to pass the skill.
Skill Sheet Head to Toe Assessment SP2022
PERFORMANCE BEHAVIORS |
*S *U COMMENTS |
10.**Assess abdomen (Inspection, Auscultation, Palpation)
a.Auscultate for bowel sounds in all four quadrants
b.Palpate abdomen for firmness, tenderness, and lower abdomen for bladderdistention.
11.**Assess and compare bilateral lower extremities for
a.Movement and strength
b.Temperature and color
c.Dorsalis pedis and posterior tibial pulses
d.Capillary refill
e.Sensation
12.Assess posterior lung sounds (if not done previously) and skin
13.**Check equipment related to the patient
a.IV? Solution, rate, site.
b.O2? Setting/type
c.Drains (including urinary catheter).
14.Survey the environment for safety concerns.
a.**Reposition patient for comfort and safety
15.Prior to leaving room
a.**Lower bed
b.**Raise appropriate bed rails
c.**Place call light and patient belongings within reach
d.**Perform hand hygiene
e.Gather and remove equipment
Evaluation
16. **Document assessment per facility policy
*S = Satisfactory, ^U = Unsatisfactory
**Critical Behaviors that need to be stated or done in order to pass the skill.
17. Write a sample nursing note:
Skill Sheet Head to Toe Assessment SP2022
Form Characteristics
| Fact Name | Details |
|---|---|
| Purpose of the Assessment | The Head to Toe Assessment form is designed to guide healthcare providers in a systematic evaluation of a patient's overall health and well-being. |
| Patient Identification | It emphasizes the need to confirm the patient’s identity using two forms of ID, ensuring safety and accuracy during assessment. |
| Critical Behaviors | Several critical behaviors are highlighted throughout the assessment. These need to be performed to pass the skill evaluation, underscoring their importance. |
| Documentation Requirement | Documenting findings in accordance with facility policy is mandatory. Accurate documentation ensures continuity of care and legal protection. |
| Performance Evaluation | Each attempt during evaluation is marked as either satisfactory (S) or unsatisfactory (U), providing clear feedback for improvement. |
| Environment Safety | The assessment requires surveying the environment for safety concerns, which is critical for patient care and comfort. |
| Equipment Checks | Before leaving the room, healthcare providers must check equipment related to the patient, ensuring all is in order and safe for use. |
| State-Specific Regulations | Depending on the state, specific laws may govern the use of assessment forms. It is essential to be knowledgeable about these regulations to remain compliant. |
Guidelines on Utilizing Head Toe Assessment
To complete the Head Toe Assessment form, you will systematically document each step of the assessment process. Each section of the form prompts you to provide essential information about the assessment, your performance, and any additional comments. Following these steps will ensure you meet all requirements and maintain clarity for evaluators.
- Fill in your Student Name at the top of the form.
- Provide your Student Signature in the designated area.
- Have your evaluator sign their name next to Evaluator Signature.
- For the first attempt, write the Date and check either Satisfactory* or Unsatisfactory^ based on your assessment.
- Repeat step 4 for the second and third attempts, ensuring dates are noted and evaluations are completed.
- List the Critical Behaviors required for passing the skill as outlined in the form.
- For Planning, gather all necessary equipment, including:
- Stethoscope
- Appropriate sized blood pressure cuff
- Pulse Oximeter
- Penlight
- Thermometer
- Gloves
- Upon entering the patient’s room, perform the following actions:
- Hand hygiene
- Identify yourself
- Identify the patient using two forms of ID (name and date of birth)
- Verify patient allergies
- Assure privacy
- Explain the procedures to the patient
- Allow for patient questions
- Raise the bed to a comfortable working height
- Put on gloves
- Assess the patient's level of consciousness and orientation.
- Document pain, pulse oximetry, blood pressure, pulse, respiratory rate, and temperature readings.
- Examine the head using PERRLA (Pupils Equal, Round, React to Light and Accommodation). Check for any abnormalities.
- Throughout the assessment, observe and note the condition of hair, skin, and nails.
- Assess and compare bilateral upper extremities for:
- Hand grasps for equality and strength
- Temperature and color
- Radial pulses
- Capillary refill
- Sensation
- Check the apical pulse. Auscultate heart sounds and document the rate and regularity for one minute.
- Auscultate lung sounds and evaluate the rise and fall of the chest. Assess breath sounds across the appropriate sites.
- Inspect, auscultate, and palpate the abdomen. Note bowel sounds and assess for tenderness and distention.
- Examine and compare bilateral lower extremities for:
- Movement and strength
- Temperature and color
- Dorsalis pedis and posterior tibial pulses
- Capillary refill
- Sensation
- If not previously done, assess posterior lung sounds and inspect the skin.
- Check any equipment related to the patient, including IV settings and drains.
- Survey the environment for safety concerns, ensuring patient comfort.
- Before leaving the room, perform the following:
- Lower the bed
- Raise the appropriate bed rails
- Place call light and patient belongings within reach
- Perform hand hygiene
- Gather and remove equipment
- Document your assessment in compliance with facility policies.
- Write a sample nursing note as part of the assessment documentation.
What You Should Know About This Form
What is the purpose of the Head Toe Assessment form?
The Head Toe Assessment form is designed to guide healthcare professionals in performing a comprehensive physical assessment of a patient. It ensures that critical assessments are not overlooked and helps maintain a standard of care in clinical practice.
What does 'Satisfactory' and 'Unsatisfactory' mean on the assessment form?
'Satisfactory' indicates that the evaluator found the student's performance to meet the required standards for the assessment. Conversely, 'Unsatisfactory' means that the performance did not meet those standards, highlighting areas that need improvement and requiring further attempts.
How do I record my attempts on the assessment form?
Each attempt must be documented by an evaluator, who signs and dates the form. After each attempt, the evaluator will mark either 'Satisfactory' or 'Unsatisfactory' to reflect the performance level. Ensure that all necessary signatures are obtained promptly after each assessment.
What specific behaviors are considered critical in passing the assessment?
Critical behaviors include essential actions that must be performed correctly during the assessment. These behaviors are assessed throughout various components, such as patient identification using two forms of ID, performing hand hygiene, and ensuring privacy, among others. Attention to these critical behaviors is crucial for passing the skill assessment.
In what order should I conduct the head-to-toe assessment?
The head-to-toe assessment follows a systematic approach, starting from the patient’s level of consciousness and orientation, to vital signs, and then moving through each system assessed. Each component builds upon the previous one, ensuring a thorough evaluation of the patient’s overall condition.
Why is it important to perform hand hygiene before the assessment?
Hand hygiene is critical to prevent the spread of infections. Performing hand hygiene before interacting with a patient minimizes the risk of transmitting pathogens and promotes a safer healthcare environment for both the patient and the healthcare provider.
What should I do if I receive an 'Unsatisfactory' rating?
If you receive an 'Unsatisfactory' rating, it's important to focus on the feedback provided by the evaluator. A second attempt is often available, so take the time to learn from the assessment, practice the necessary skills, and address any deficiencies highlighted in the evaluator's comments.
How should I document my assessment according to the facility policy?
Documentation should be clear, concise, and compliant with your facility's guidelines. Use the appropriate formats outlined in the policy, including relevant findings from the assessment. Proper documentation is vital for ensuring continuity of care and legal protection.
Common mistakes
When filling out the Head Toe Assessment form, individuals often encounter pitfalls that can lead to misunderstandings or evaluation delays. One crucial mistake is failing to properly identify the patient. The guidelines require two forms of identification, such as the patient's name and date of birth. Neglecting this step can not only compromise patient safety, but it may also result in immediate disqualification from passing the skill assessment.
Another frequent error stems from overlooking essential equipment. The form specifies the necessity to gather various tools such as a stethoscope, blood pressure cuff, and thermometers, among others. If any of these items are missing, it undermines the overall assessment process. Candidates must check their equipment thoroughly before proceeding, ensuring that a comprehensive evaluation can take place without interruptions or the need for retrials.
A third common mistake involves insufficient documentation. Proper evaluation means recording observations accurately during the assessment. Skipping the detailed notes on vital signs, such as pulse and respiratory rates, can lead evaluators to deem the assessment as unsatisfactory. It demonstrates a lack of thoroughness and attention to detail, both of which are critical in patient care scenarios.
Finally, neglecting the environment and patient comfort can severely affect the assessment results. This includes ensuring that the bed is at a comfortable working height and that safety concerns, such as clutter or improperly positioned equipment, are addressed. Candidates must remember that a well-organized environment not only facilitates a smooth assessment process but also contributes to the overall patient experience.
Documents used along the form
The Head to Toe Assessment form is a crucial tool used in patient evaluations. Several other forms and documents support this assessment, ensuring that all relevant facets of patient care are addressed comprehensively. Below is a brief overview of these accompanying documents.
- Nursing Care Plan: This document outlines the individual patient's needs and the interventions required to meet those needs. It serves as a guide for nurses to create tailored care strategies based on assessment outcomes.
- Patient History Form: Used to gather essential background information about the patient, this form includes medical history, allergies, medications, and previous treatments. It helps healthcare providers to understand the patient’s context better during assessments.
- Vital Signs Chart: This chart records the patient's vital signs—such as temperature, heart rate, and blood pressure—over time. It helps track any trends that may indicate improvements or deteriorations in the patient's condition.
- Medication Administration Record (MAR): This document logs all medications prescribed to the patient, including dosages and schedules. It's essential for preventing medication errors and ensuring the patient's treatment plan is executed correctly.
- Patient Consent Form: Before any treatment or assessment, this form is signed by the patient to confirm their understanding and agreement to proceed. It protects both the patient’s rights and the healthcare provider’s legal compliance.
These accompanying forms and documents are integral to providing thorough and effective patient care. They ensure clear communication among healthcare providers and enhance patient safety throughout the assessment process.
Similar forms
- Physical Assessment Form: This document provides a structured approach to evaluating a patient's overall health status. Similar to the Head Toe Assessment, it includes components like vital signs and observations of physical appearance.
- Admission Assessment Form: Typically completed during a patient's admission to a healthcare facility, this form gathers comprehensive health information. Like the Head Toe Assessment, it focuses on collecting data essential for creating a care plan.
- Nursing Care Plan: This document outlines the nursing interventions needed based on individual patient assessments. Both the care plan and the Head Toe Assessment serve as crucial tools in guiding patient care based on evaluated needs.
- Emergency Assessment Form: In emergent situations, healthcare providers use this document to rapidly gather critical information. It closely resembles the Head Toe Assessment in that it prioritizes key assessments and immediate interventions.
- Daily Nursing Progress Notes: Nurses utilize this document to record the patient’s ongoing condition and any changes in status. Like the Head Toe Assessment, it emphasizes the importance of continuous evaluation and documentation.
- Post-Operative Assessment Form: Following surgery, this form focuses on recovery and potential complications. The attention to detail in identifying key observations mirrors that found in the Head Toe Assessment.
- Patient Discharge Summary: This document summarizes the patient's condition at discharge and future care instructions. Both the discharge summary and the Head Toe Assessment highlight critical information needed for ongoing care.
Dos and Don'ts
Here is a list of things to do and not to do when filling out the Head Toe Assessment form:
- Do: Gather all necessary equipment before you start the assessment.
- Do: Perform hand hygiene upon entering the patient's room.
- Do: Identify the patient using at least two forms of identification.
- Do: Explain the procedure to the patient and allow them to ask questions.
- Do: Note the patient's condition during the assessment, including hair, skin, and nails.
- Do: Document your findings clearly per facility policy.
- Do: Ensure patient comfort by lowering the bed and adjusting bed rails as needed before leaving.
- Don't: Skip any critical behaviors listed in the assessment protocol.
- Don't: Forget to verify the patient's allergies before beginning the assessment.
- Don't: Neglect to auscultate the heart and lung sounds properly.
- Don't: Leave the room without ensuring the patient has call light within reach.
- Don't: Ignore safety concerns in the environment prior to conducting the assessment.
- Don't: Rush through the assessment; take the time to observe and compare findings.
- Don't: Forget to perform hand hygiene before and after the assessment.
Misconceptions
Many misconceptions surround the Head Toe Assessment form. Understanding these myths can improve how assessments are perceived and conducted.
- It is just a checklist. Some believe the form merely serves as a checklist, but it is a comprehensive guide that ensures essential assessments are not overlooked.
- Only new nurses need to use it. This form is not exclusively for new nurses. Experienced nurses also benefit from its structured approach, which can enhance thoroughness and consistency.
- All items must be done every time. While most assessments are critical, not every item requires completion in every situation, depending on the patient's specific needs and condition.
- Documentation is unnecessary if I pass the assessments. Documentation is vital, regardless of performance. It ensures continuity of care and serves as a legal record of the assessment process.
- It doesn’t account for patient preferences. The form does encourage nurses to explain procedures and allow for patient questions, promoting patient-centered care.
- The form is only for skills evaluation. Although it assesses skills, it also emphasizes critical thinking and clinical judgment during patient assessments.
- You can’t make notes on the form. In fact, notes and comments are encouraged. They provide valuable insights and rationale for the assessments performed.
Key takeaways
Completing the Head to Toe Assessment form is a critical skill necessary for effective patient assessment. Here are some key takeaways to keep in mind:
- Understand the Importance: This assessment helps form a comprehensive picture of the patient’s health and guides further care decisions.
- Gather Your Equipment: Before entering the patient's room, ensure you have all necessary equipment, like a stethoscope and blood pressure cuff.
- Prioritize Patient Interaction: Perform hand hygiene, introduce yourself, and establish rapport with the patient before starting the assessment.
- Confirm Patient Identity: Always identify the patient using two forms of ID, such as their name and date of birth, to ensure safety and accuracy.
- Evaluate Critical Behaviors: Pay attention to specific critical behaviors that are necessary to pass the assessment, such as ensuring patient privacy and explaining the procedure.
- Document Thoroughly: After the assessment, accurately document your findings in accordance with facility policy. This is essential for continuity of care.
- Adapt to the Patient's Needs: Be observant and allow for patient questions throughout the assessment, fostering a comfortable environment.
- Use a Systematic Approach: Follow the assessment steps methodically, such as checking vital signs, lung sounds, and abdominal assessments.
- Ensure Patient Comfort: Before leaving the room, lower the bed, raise appropriate bed rails, and place the call light within reach to ensure patient safety.
- Perform Each Skill Mindfully: Take your time when auscultating heart and lung sounds, and always assess for any abnormalities throughout the process.
By focusing on these principles, you can enhance your skills in performing comprehensive head-to-toe assessments, thereby providing better care for your patients.
Browse Other Templates
Can Manufactured Homes Be Remodeled - The HCD 433A will be referenced in any future assessments or property transactions.
Barro's Pizza Jobs - We appreciate your interest in Barro’s Pizza, and your application will be kept on file for six months.
Certificate of Membership - A fundamental document for companies with complex membership structures.