Fill Out Your Hospital Admit Form
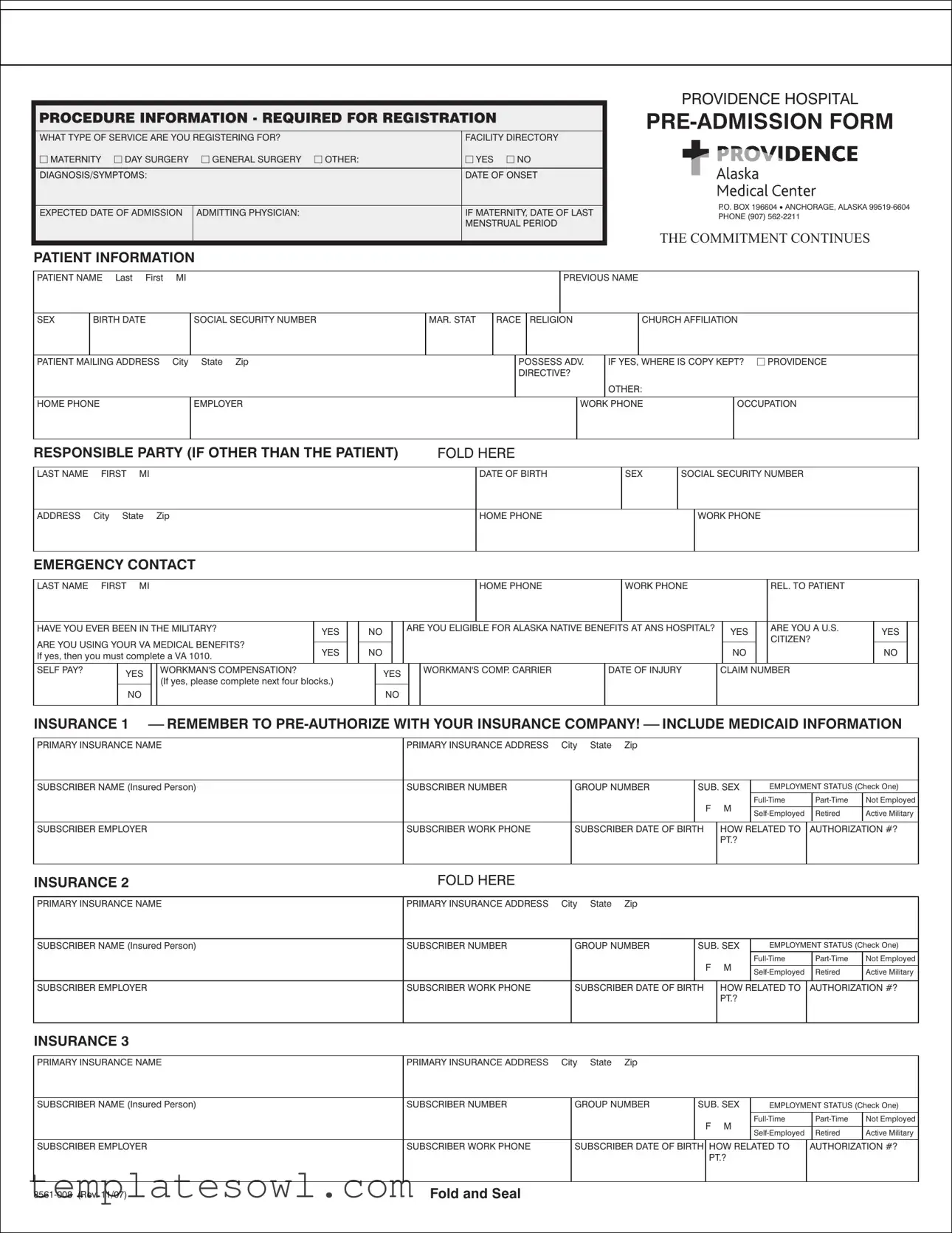
Understanding the Hospital Admit form is essential for anyone preparing for a medical procedure or hospitalization. This document serves as a critical step in the registration process, gathering necessary information to facilitate a smooth admission. It incorporates multiple sections, including details about the type of service required, such as maternity care or general surgery. The form also requires specific patient information, including personal identifiers like name, date of birth, and contact details, alongside medical history and insurance coverage. The admitting physician’s name, diagnosis, and symptoms are included to ensure that healthcare providers have a comprehensive understanding of the patient's medical background. Additionally, it addresses the patient's eligibility for various benefits, such as military or native health programs, and requires emergency contact details. The accurate completion of this form can streamline the admission process and ensure that all pre-admission requirements are met, helping healthcare providers deliver the best possible care.
Hospital Admit Example
PROCEDURE INFORMATION - REQUIRED FOR REGISTRATION
WHAT TYPE OF SERVICE ARE YOU REGISTERING FOR? |
FACILITY DIRECTORY |
|
MATERNITY DAY SURGERY |
GENERAL SURGERY OTHER: |
YES NO |
|
|
|
DIAGNOSIS/SYMPTOMS: |
|
DATE OF ONSET |
|
|
|
EXPECTED DATE OF ADMISSION |
ADMITTING PHYSICIAN: |
IF MATERNITY, DATE OF LAST |
|
|
MENSTRUAL PERIOD |
|
|
|
PATIENT INFORMATION
PROVIDENCE HOSPITAL
P.O. BOX 196604 • ANCHORAGE, ALASKA
PHONE (907)
THE COMMITMENT CONTINUES
PATIENT NAME Last First |
MI |
|
|
|
|
PREVIOUS NAME |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
SEX |
BIRTH DATE |
|
SOCIAL SECURITY NUMBER |
MAR. STAT |
RACE |
RELIGION |
|
CHURCH AFFILIATION |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT MAILING ADDRESS |
City State Zip |
|
|
POSSESS ADV. |
IF YES, WHERE IS COPY KEPT? PROVIDENCE |
|||||||
|
|
|
|
|
|
DIRECTIVE? |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
OTHER: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HOME PHONE |
|
EMPLOYER |
|
|
|
|
|
WORK PHONE |
OCCUPATION |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
RESPONSIBLE PARTY (IF OTHER THAN THE PATIENT) |
FOLD HERE |
LAST NAME FIRST MI
ADDRESS City State Zip
DATE OF BIRTH |
SEX |
SOCIAL SECURITY NUMBER |
|
HOME PHONE |
|
|
WORK PHONE |
|
|
||
|
|
|
|
EMERGENCY CONTACT
LAST NAME FIRST |
MI |
|
|
|
|
|
|
|
|
|
|
HOME PHONE |
|
|
|
|
WORK PHONE |
|
|
|
|
|
|
REL. TO PATIENT |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
HAVE YOU EVER BEEN IN THE MILITARY? |
YES |
|
NO |
|
|
ARE YOU ELIGIBLE FOR ALASKA NATIVE BENEFITS AT ANS HOSPITAL? |
|
YES |
|
|
ARE YOU A U.S. |
|
YES |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITIZEN? |
|
|
|||||||
ARE YOU USING YOUR VA MEDICAL BENEFITS? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
YES |
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NO |
|
|
|
|
|
|
NO |
|
||||||
If yes, then you must complete a VA 1010. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SELF PAY? |
YES |
|
WORKMAN'S COMPENSATION? |
|
|
|
|
YES |
|
|
WORKMAN'S COMP. CARRIER |
|
|
|
DATE OF INJURY |
|
|
CLAIM NUMBER |
|
|
|
|
|
||||||||
|
|
(If yes, please complete next four blocks.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
NO |
|
|
|
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
INSURANCE 1 ⎯ REMEMBER TO |
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRIMARY INSURANCE NAME |
|
|
|
|
|
|
PRIMARY INSURANCE ADDRESS |
City |
State |
Zip |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
SUBSCRIBER NAME (Insured Person) |
|
|
|
|
|
|
SUBSCRIBER NUMBER |
|
GROUP NUMBER |
SUB. SEX |
|
|
EMPLOYMENT STATUS (Check One) |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Not Employed |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F |
|
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Retired |
Active Military |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
SUBSCRIBER EMPLOYER |
|
|
|
|
|
|
|
SUBSCRIBER WORK PHONE |
|
SUBSCRIBER DATE OF BIRTH |
HOW RELATED TO |
AUTHORIZATION #? |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PT.? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INSURANCE 2 |
|
|
|
|
|
|
|
|
|
|
|
FOLD HERE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRIMARY INSURANCE NAME |
|
|
|
|
|
|
PRIMARY INSURANCE ADDRESS |
City |
State |
Zip |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
SUBSCRIBER NAME (Insured Person) |
|
|
|
|
|
|
SUBSCRIBER NUMBER |
|
GROUP NUMBER |
SUB. SEX |
|
|
EMPLOYMENT STATUS (Check One) |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Not Employed |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F |
|
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Retired |
Active Military |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
SUBSCRIBER EMPLOYER |
|
|
|
|
|
|
|
SUBSCRIBER WORK PHONE |
|
SUBSCRIBER DATE OF BIRTH |
HOW RELATED TO |
AUTHORIZATION #? |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PT.? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INSURANCE 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRIMARY INSURANCE NAME |
|
|
|
|
|
|
PRIMARY INSURANCE ADDRESS |
City |
State |
Zip |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
SUBSCRIBER NAME (Insured Person) |
|
|
|
|
|
|
SUBSCRIBER NUMBER |
|
GROUP NUMBER |
SUB. SEX |
|
|
EMPLOYMENT STATUS (Check One) |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F |
|
M |
|
Not Employed |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Retired |
Active Military |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
SUBSCRIBER EMPLOYER |
|
|
|
|
|
|
|
SUBSCRIBER WORK PHONE |
|
SUBSCRIBER DATE OF BIRTH |
HOW RELATED TO |
AUTHORIZATION #? |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PT.? |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fold and Seal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
HERE
STAMP
POSTAGE
PLACE
|
.Association Hospital Catholic the of member a is Center Medical Alaska Providence |
.programs assistance other for applying in you assist to or arrangement payment equitable an |
|
establish to you with work to happy be will We .know us let please hardship, financial a is bill hospital your If |
|
|
.1902 since Alaska throughout people servicing been have Providence of |
Sisters The .pay to ability their of regardless individuals all to available services care health necessary make |
|
to ⎯ mission their fulfill to work Sisters the which, through agencies, giving care profit for not of network |
|
a of part a is It |
.Providence of Sisters the by operated and owned is Center Medical Alaska Providence |
|
Providence of Sisters the of Mission The |
.insurance after remaining balance expected the be will registration of point at due balance the registration, to prior obtained is authorization payment a and service covered a is this that determined has insurance your If .registration of time at full in payment require surgeries cosmetic outpatient and inpatient Elective
Surgeries Cosmetic
Form Characteristics
| Fact Name | Description |
|---|---|
| Required Information | The Hospital Admit form requires essential details about the patient's medical condition, including diagnosis and symptoms. |
| Patient Identification | Personal information such as name, date of birth, and social security number must be provided for proper identification. This aids in record accuracy. |
| Insurance Details | Patients need to furnish information about their health insurance, including primary and secondary coverage, to facilitate billing. |
| Emergency Contact Requirement | An emergency contact must be listed. This ensures that a designated individual can be reached in case of immediate need. |
| Military Status | The form asks whether the patient has previously served in the military or if they are eligible for specific benefits. |
| Maternity Information | For maternity patients, additional information such as the date of the last menstrual period is required to provide appropriate care. |
| Contact Information | Both home and work phone numbers are mandatory. This allows for communication regarding the patient’s care and any billing inquiries. |
| Governing Laws | In Alaska, forms are governed by Title 47 of the Alaska Statutes, particularly regarding patient rights and healthcare documentation. |
Guidelines on Utilizing Hospital Admit
The Hospital Admit form is crucial for registering a patient for their upcoming medical service. It's important to complete this form accurately to ensure all necessary information is communicated properly to the healthcare providers. Here’s a straightforward guide on how to fill it out.
- Identify the Service: Begin by selecting the type of service you are registering for by checking the appropriate box (Maternity, Day Surgery, General Surgery, or Other).
- Complete Procedure Information: Fill in the diagnosis/symptoms, date of onset, expected date of admission, and the name of the admitting physician. If applicable for maternity, include the date of the last menstrual period.
- Patient Information: Provide the patient's full name (Last, First, MI), previous name, sex, birth date, social security number, marital status, race, religion, and church affiliation.
- Mailing Address: Enter the patient's complete mailing address (City, State, Zip). Note if the patient has an advance directive and where a copy is kept.
- Contact Details: List the home phone number, employer, work phone, and occupation of the patient.
- Responsible Party: If someone other than the patient is responsible for medical bills, fill out their information (Name, Address, Date of Birth, Sex, Social Security Number, Home and Work Phone).
- Emergency Contact: Provide details for an emergency contact (Name, Home Phone, Work Phone, and their relation to the patient).
- Military and Benefits Information: Indicate if the patient has ever been in the military, if eligible for Alaska Native benefits, if they are a U.S. citizen, or if they are using VA medical benefits.
- Insurance Information: Fill out details for the primary insurance provider, including the insurance name and address, subscriber name, subscriber number, group number, sex, employment status, employer, work phone, and date of birth. Repeat this for secondary and tertiary insurance if applicable.
Once completed, ensure the form is reviewed for accuracy before submitting it along with any other required documents. This will help facilitate a smoother admission process.
What You Should Know About This Form
What is the purpose of the Hospital Admit form?
The Hospital Admit form is designed to collect essential information needed for your registration and admission to the hospital. By filling this form, you provide vital details about your diagnosis, symptoms, and any specific medical history, ensuring that the healthcare team is well-informed. This helps them deliver the best possible care tailored to your needs.
What types of services can I register for using this form?
This form allows you to register for a variety of services, including maternity care, day surgery, general surgery, and more. If you have a specific type of service in mind that isn’t listed, you can indicate that on the form. It’s important to accurately select the service to streamline your admission process.
What personal information do I need to provide?
You'll need to provide personal details such as your name, date of birth, social security number, address, and contact information. Additionally, information about your insurance coverage and employment status is required. This information assists the hospital in verifying your identity and determining eligibility for services.
Is insurance information required for registration?
Yes, providing your insurance information is an important part of the registration process. You should include the details of your primary insurance company, along with any secondary or tertiary insurance if applicable. Remember to check if pre-authorization is needed from your insurance provider to avoid unexpected charges.
What if I do not have insurance?
If you do not have insurance, the form accommodates this by allowing you to indicate that you are a self-pay patient. Be aware that the hospital can assist you in discussing payment options or potential financial assistance programs tailored for your situation. Your health and well-being remain a priority, regardless of your insurance status.
What should I do if I have a financial hardship?
If you are experiencing financial hardship, don't hesitate to speak with the hospital’s financial assistance department. They can provide guidance and support in establishing equitable payment arrangements. It's essential to communicate your circumstances clearly to find a solution that works for you.
How do I ensure a smooth admission process?
To facilitate a smooth admission, make sure to complete the Hospital Admit form thoroughly and accurately. Bring all necessary documents, such as insurance cards and any medical records that may be relevant. Arriving early on your scheduled admission date can also help ease any last-minute concerns. Your preparedness will contribute greatly to a seamless experience.
Common mistakes
Filling out a Hospital Admit form can be a crucial step in receiving timely and appropriate medical care. However, many individuals make common mistakes that can lead to complications during their admission process. Understanding these errors can help ensure a smoother experience.
One frequent mistake is failing to provide complete and accurate patient information. Missing details such as a social security number, wrong birth date, or incorrect contact information can delay processing or lead to issues with insurance. It is essential to double-check all entries for accuracy before submitting the form.
Another mistake is neglecting to indicate proper insurance information. Many people forget to include details about their primary and any secondary insurances. Without this information, insurance claims may be denied, and patients could face unexpected financial burdens. It's important to have insurance cards accessible to ensure all relevant data is recorded.
Some individuals overlook the section regarding previous military service or eligibility for special benefits. This information is critical for patients who may qualify for services under the Veterans Administration or Alaska Native benefits. Omitting this could lead to a loss of potential support and services that could otherwise have been available.
Additionally, individuals often forget to specify the type of service they are registering for. The form includes options such as maternity, day surgery, or general surgery. Not selecting the appropriate service type can lead to confusion and delays in care. It is vital to understand the purpose of the visit and select the corresponding option accordingly.
Lastly, many people do not review the form before submission. This oversight can result in minor errors that could have easily been corrected. Taking a moment to read through the completed form helps catch any mistakes and ensures that all necessary information is provided. Making sure everything is accurately reported will facilitate a smoother admission process.
Documents used along the form
The Hospital Admit form is crucial for initiating patient care, but several other documents often accompany it to ensure a smooth admission process. Each document serves a specific purpose in facilitating patient registration and managing healthcare needs. Here’s a brief overview of the key forms typically used alongside the Hospital Admit form.
- Pre-Admission Form: This document collects essential personal information, including patient demographics and insurance details. It helps hospitals prepare resources and staff for the patient's arrival.
- Insurance Authorization Form: Required for patients with insurance, this form secures approval from the insurance provider for pre-admission services. Ensuring this is completed can prevent unexpected costs later.
- Advance Directive: This form indicates a patient's preferences for medical treatment in case they cannot communicate their wishes. It is crucial for guiding healthcare decisions in emergencies.
- Patient Medical History Form: Detailed information about a patient's past health conditions, medications, and allergies is gathered in this document. Accurate data assists healthcare providers in creating effective treatment plans.
Carefully preparing these documents can streamline the admission process. Ensure that each is completed accurately to avoid delays in receiving essential medical care. Prioritize your health by addressing these requirements promptly.
Similar forms
The Hospital Admit form serves a crucial role in a patient's journey through healthcare. Similar documents help facilitate different processes in medical settings. Here are seven documents that closely align with the Hospital Admit form:
- Patient Registration Form: This form collects essential information about the patient, such as name, contact details, and insurance information, much like the Hospital Admit form.
- Medical History Form: Comprehensive details about a patient's past medical conditions, surgeries, and allergies are gathered here. It is akin to the Admit form by requesting crucial background information that informs treatment.
- Insurance Verification Form: This document is used to confirm a patient’s insurance coverage and benefits, paralleling the sections on the Admit form that deal with insurance details and pre-authorization.
- Consent for Treatment Form: Patients give their consent for medical procedures through this document. Similarly, the Hospital Admit form may include sections where patients acknowledge understanding of the services they are seeking.
- Emergency Contact Form: This form requests information about who to contact in case of an emergency. It mirrors the Hospital Admit form’s requirement for emergency contact details.
- Advance Directive Form: Patients express their healthcare preferences through this document. The Admit form may reference such directives to ensure patient wishes are recognized within the treatment plan.
- Discharge Instructions Form: This document lays out the care required after leaving the hospital. Similar to the Admit form, it focuses on patient well-being and necessary information regarding ongoing treatment post-admission.
Dos and Don'ts
When filling out the Hospital Admit form, it's important to follow certain guidelines to ensure the process runs smoothly. Here are some do's and don'ts to keep in mind:
- Do read the form thoroughly before starting to fill it out.
- Do provide accurate information about your medical history and current symptoms.
- Do check all insurance details for completeness.
- Do sign and date the form where required.
- Don't leave any mandatory fields blank.
- Don't forget to include your emergency contact information.
- Don't rush through the form; take your time to ensure accuracy.
- Don't hesitate to ask for assistance if you're unsure about any section.
Misconceptions
Understanding the Hospital Admit form can be daunting, and many misconceptions exist about its purpose and function. Here are nine common misconceptions regarding this important document:
- The form is only necessary for inpatient admissions. Many believe the form applies solely to those admitted for extended stays. In reality, it's required for all services, including outpatient procedures and day surgeries.
- You do not need to fill it out if you're using insurance. Regardless of insurance, you must complete the form to provide essential information for registration and billing.
- The form is the same for all hospitals. Each facility has a unique admit form tailored to its policies and requirements. Always use the specific form for the hospital where you will receive care.
- It only collects personal information. While the form does gather personal data, it also requires medical information crucial for admission, such as diagnosis and symptoms.
- Emergency patients do not need to fill it out. Even in emergencies, signing the admit form is important for documentation and processing care effectively.
- It's okay to skip questions you’re unsure about. Providing accurate answers is essential. If you're uncertain, it's best to ask hospital staff for assistance rather than leave sections incomplete.
- Once submitted, the information cannot be changed. If circumstances change or errors are found, you can update your information at any time during the admission process.
- The form does not require a signature if insurance is used. A signature is necessary regardless of payment method to confirm that the information provided is accurate and complete.
- There are no consequences for submitting incorrect information. Providing false or incomplete details can lead to complications in care and billing issues, making accuracy vital.
Being informed about these misconceptions can help streamline the hospital admission process and reduce unnecessary stress for patients and their families.
Key takeaways
Filling out the Hospital Admit form accurately is crucial for a smooth admission process. Below are key takeaways to keep in mind:
- All required information must be completed. Missing details can delay your admission.
- Specify the type of service you are registering for, whether it's maternity, general surgery, or another category.
- Diagnosis and symptoms should be clearly stated. Providing the date of onset helps the medical team understand your condition better.
- Ensure you list the admitting physician. This detail is necessary for coordination of care.
- Insurance details are crucial. Verify that you have pre-authorization with your insurance company, especially for surgical procedures.
- Emergency contact information should be up-to-date. This person should be someone who can make decisions on your behalf if needed.
- Indicate any special benefits. If you are eligible for Alaska Native benefits or using VA medical benefits, it is important to specify that on the form.
- Review the form multiple times. Double-checking ensures that all information is accurate and complete, which can avoid administrative hurdles upon admission.
Browse Other Templates
Fl-100 - It allows for the declaration of separate and community property in the dissolution process.
The Ssho as a Minimum Must Have Completed - The form assists in preventing accidents through comprehensive planning.