Fill Out Your Hospital Bill Form
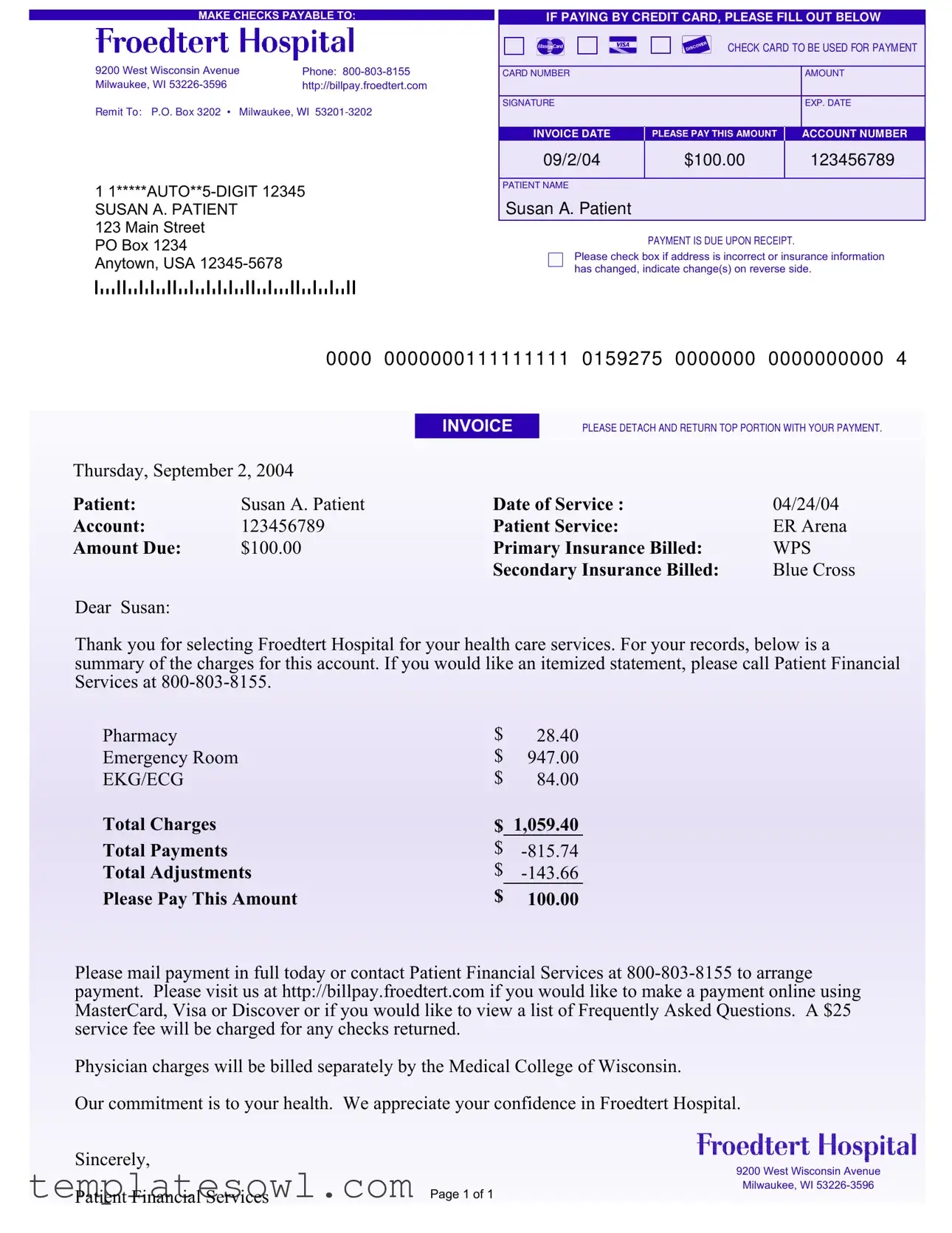
The Hospital Bill form plays a critical role in the healthcare billing process, ensuring transparency and clarity for patients regarding their medical expenses. This form provides essential details such as the patient's name, account number, date of service, and the total amount due—elements crucial for understanding one’s financial obligations. For example, in the case of Susan A. Patient, the bill summarizes charges for various services, including emergency room visits and pharmacy costs, leading to a total charge of $1,059.40. Importantly, it outlines payments and adjustments, thereby indicating a final amount of $100.00 that needs to be settled upon receipt. The form also includes directions for payment methods, specifying that checks should be made payable to Froedtert Hospital and providing an online payment option for added convenience. Patients are reminded to update any changes in their personal or insurance information, underscoring the importance of accurate and current records. Given that timely payment is required, it becomes essential for patients to understand the implications of this form not just for their health services but for their overall financial management as well. Having access to this information allows individuals to navigate their healthcare expenses more effectively and stay informed about their financial responsibilities.
Hospital Bill Example
MAKE CHECKS PAYABLE TO:
9200 West Wisconsin Avenue |
Phone: |
Milwaukee, WI |
http://billpay.froedtert.com |
Remit To: P.O. Box 3202 • Milwaukee, WI
1
SUSAN A. PATIENT
123 Main Street
PO Box 1234
Anytown, USA
IF PAYING BY CREDIT CARD, PLEASE FILL OUT BELOW
CHECK CARD TO BE USED FOR PAYM ENT
CARD NUMBER |
AMOUNT |
|
|
SIGNATURE |
EXP. DATE |
|
|
INVOICE DATE |
PLEASE PAY THIS AMOUNT |
ACCOUNT NUMBER |
09/2/04 |
$100.00 |
123456789 |
|
|
|
PATIENT NAME
Susan A. Patient
PAYMENT IS DUE UPON RECEIPT.
Please check box if address is incorrect or insurance information has changed, indicate change(s) on reverse side.
|
0000 |
0000000111111111 |
0159275 |
0000000 |
0000000000 |
4 |
|
|
INVOICE |
PLEASE DETACH AND RETURN TOP PORTION WITH YOUR PAYMENT. |
|
||
Thursday, September 2, 2004 |
|
|
|
|
|
|
Patient: |
Susan A. Patient |
Date of Service : |
|
04/24/04 |
|
|
Account: |
123456789 |
Patient Service: |
|
ER Arena |
|
|
Amount Due: |
$100.00 |
Primary Insurance Billed: |
WPS |
|
||
|
|
Secondary Insurance Billed: |
Blue Cross |
|
||
Dear Susan:
Thank you for selecting Froedtert Hospital for your health care services. For your records, below is a summary of the charges for this account. If you would like an itemized statement, please call Patient Financial Services at
Pharmacy |
$ |
28.40 |
Emergency Room |
$ |
947.00 |
EKG/ECG |
$ |
84.00 |
Total Charges |
$ |
1,059.40 |
Total Payments |
$ |
|
Total Adjustments |
$ |
|
Please Pay This Amount |
$ |
100.00 |
Please mail payment in full today or contact Patient Financial Services at
Physician charges will be billed separately by the Medical College of Wisconsin.
Our commitment is to your health. We appreciate your confidence in Froedtert Hospital.
Sincerely,
9200 West Wisconsin Avenue
|
Milwaukee, WI |
Patient Financial Services |
Page 1 of 1 |
|
PLEASE UPDATE ANY INFORM ATION THAT HAS CHANGED SINCE YOUR LAST STATEM ENT
ABOUT YOU:
YOUR NAME (Last, First, Middle Initial)
ADDRESS
CITY |
|
|
|
|
|
|
|
|
|
|
STATE |
|
|
|
|
ZIP |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
|
|
|
|
|
|
|
|
|
MARITAL STATUS |
|
|
|
|
Separated |
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Single |
|
|
|
|
Divorced |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Married |
|
|
|
|
Widowed |
|
||||||
EMPLOYER'S NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYER'S ADDRESS |
|
|
|
|
|
|
|
CITY |
STATE |
|
|
|
|
ZIP |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ABOUT YOUR INSURANCE:
YOUR PRIMARY INSURANCE COMPANY'S NAME
PRIMARY INSURANCE COMPANY'S ADDRESS
CITY |
STATE |
ZIP |
||
|
|
|
|
|
POLICYHOLDER'S ID NUMBER |
GROUP PLAN NUMBER |
|
|
|
|
|
|
|
|
YOUR SECONDARY INSURANCE COMPANY'S NAME |
|
|
|
|
|
|
|
|
|
SECONDARY INSURANCE COMPANY'S ADDRESS |
|
|
|
|
|
|
|
|
|
CITY |
STATE |
ZIP |
||
|
|
|
|
|
POLICYHOLDER'S ID NUMBER |
GROUP PLAN NUMBER |
|
|
|
|
|
|
|
|
Form Characteristics
| Fact Name | Description |
|---|---|
| Payment Information | The bill includes instructions to make checks payable to Froedtert Hospital and provides a phone number for assistance with payment inquiries. |
| Invoice Details | The invoice lists charges, payments, and adjustments. It shows a total of $1,059.40 in charges with a balance due of $100.00. |
| Insurance Billing | Both primary and secondary insurance providers are noted on the bill, which are WPS and Blue Cross, respectively. |
| State-Specific Law | This billing process is governed by Wisconsin Statutes Chapter 646 regarding health care payments. |
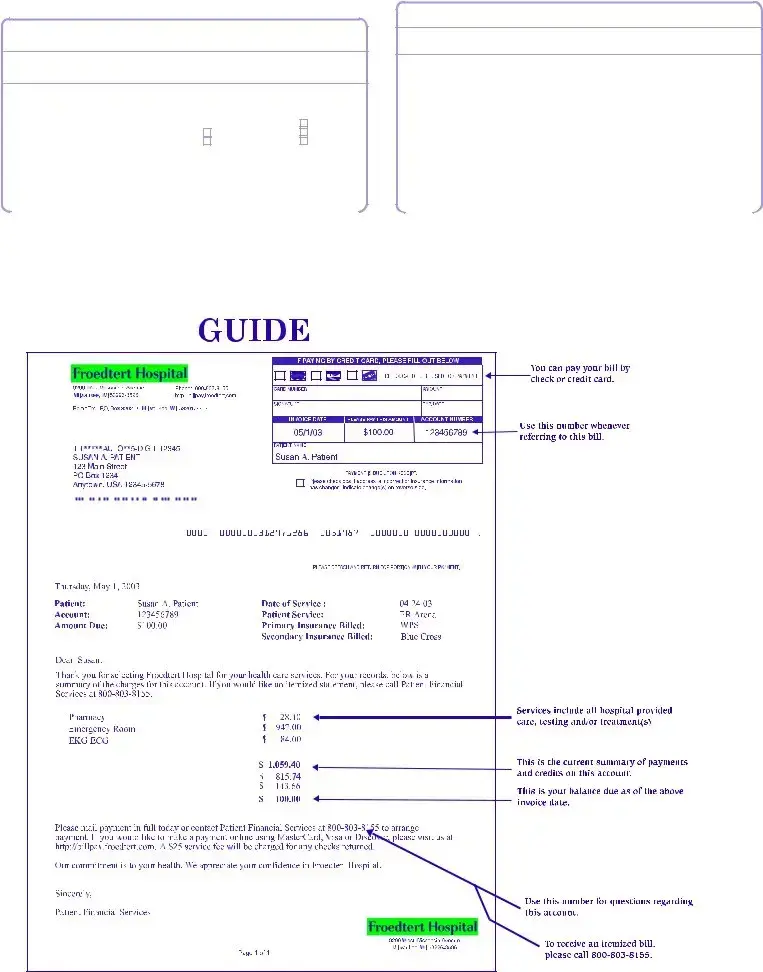
Guidelines on Utilizing Hospital Bill
Please follow these instructions carefully to ensure your Hospital Bill form is completed accurately. Providing the correct information is vital for processing your payment and addressing any disputes or queries that may arise. Once the form is filled out, it should be mailed promptly to the address indicated to avoid any delays.
- Make Payment: Determine if you will be paying by check or credit card. If using a credit card, have your card information ready.
- Fill Out Personal Information: Write your full name at the top of the form, including your last name, first name, and middle initial.
- Complete Address: List your complete address, including street name, city, state, and ZIP code.
- Add Contact Information: Fill in your telephone number so the hospital can contact you if needed.
- Marital Status: Check the applicable box to indicate your marital status: separated, single, divorced, married, or widowed.
- Employer Details: Enter your employer’s name, address, and telephone number. Ensure all fields are filled out correctly.
- Insurance Information: Provide details for your primary insurance, including the company name, address, ID number, and group plan number. Repeat this for your secondary insurance if applicable.
- Enter Payment Details: If paying by credit card, fill out your card number, expiration date, and the amount you are paying. Sign where indicated.
- Invoice Date: Record the date on the invoice provided for your reference.
- Review: Double-check all entries for accuracy before mailing the form. Incorrect information can lead to payment issues.
- Submit: Tear off and return the top portion of the bill with your payment. For checks, make them payable to "Froedtert Hospital" and send them to the provided address.
What You Should Know About This Form
What should I do if I believe that my hospital bill is incorrect?
If you think there is an error on your hospital bill, it is important to address it as soon as possible. Start by reviewing the details carefully. Compare the charges listed on the bill with your insurance coverage and any statements you may have received. If you still find discrepancies, you may contact Patient Financial Services at 800-803-8155. They can assist you in resolving any issues and ensuring that you receive accurate billing information.
How can I make a payment for my hospital bill?
You have several options for making a payment. You can mail a check, made payable to Froedtert Hospital, to the address provided on your bill. If you prefer to pay by credit card, fill out the designated section on the form included with your bill. Additionally, payments can be made online at http://billpay.froedtert.com using MasterCard, Visa, or Discover. It is recommended to make your payment as soon as possible to avoid any late fees or service charges.
What happens if I miss the payment due date?
Payment is due upon receipt of the bill. If you miss the payment due date, late fees may be incurred, and a $25 service fee will be charged for any returned checks. To prevent further complications, it is best to reach out to Patient Financial Services to discuss payment arrangements. They are there to help and can provide guidance on how to best address your situation.
Can I receive an itemized statement of my charges?
Yes, if you would like a detailed breakdown of the charges on your hospital bill, you can request an itemized statement. Simply call Patient Financial Services at 800-803-8155, and they will assist you in obtaining the information you need. Having an itemized statement can help you further understand your charges and answer any questions you might have regarding your bill.
Common mistakes
Filling out a hospital bill form can seem straightforward, but many people make errors that can lead to delays in payment or complications in their medical records. Here are ten common mistakes to avoid.
One frequent error occurs when individuals forget to provide their full name. For instance, simply writing "Susan" or "Patient" instead of Susan A. Patient can create confusion and mismatches in the hospital's records. Always ensure that your name matches what is on your identification documents.
Another mistake is neglecting to update contact information. Many patients will leave their address as it was previously listed, even if they have moved. If you have a new address, it is essential to update it on the form to ensure the hospital can reach you regarding any follow-up matters.
Many people also overlook the insurance details. Failing to fill in both the primary and secondary insurance company information can lead to billing issues. Be detailed with the names and addresses of both insurers and ensure that all ID and group plan numbers are accurate. Miscommunication can cause unnecessary delays in processing your bill.
Not signing the form is another common mistake. Payment forms are legal documents, and without your signature, they are considered incomplete. Always double-check that you have signed the form and written the date correctly.
Additionally, individuals sometimes forget to indicate their method of payment. When paying by credit card, it's crucial that the card number is filled out correctly. If in doubt, double-check your card against the information you are providing on the form.
Some patients ignore the instructions regarding balance payment. Even when instructed to pay the amount due upon receipt, some may assume they have more time. Paying promptly is essential to avoid late fees or other financial penalties.
It's also important to be cautious about the format of the dates. Errors like reversing day and month can cause confusion. Instead of writing 09/2/04, the correct format should be consistently applied throughout your documentation to avoid ambiguity.
Another easy mistake is the failure to check for discrepancies. Patients often assume the amounts on the form are accurate without reviewing them closely. Before submitting, ensure that your total payments and adjustments are correct. If in doubt, request an itemized statement for clarity.
Finally, individuals sometimes forget to keep a copy of the filled-out form for their records. Documenting what you send can be crucial if there are questions or disputes in the future. Having proof of what information you provided can aid in resolving such issues.
By avoiding these common pitfalls, patients can ensure that their interactions with hospital billing processes are smoother and more efficient. Proper attention to detail saves time, money, and frustration in the long run.
Documents used along the form
When navigating the complexities of healthcare billing, it is essential to recognize various forms and documents that accompany the Hospital Bill form. Having a clear understanding of these documents can help ensure timely payments and prevent any unexpected issues with your healthcare bills. Below is a list of common forms that are often associated with your hospital billing process.
- Insurance Claim Form: This document is submitted to your health insurance provider to request payment for the healthcare services you received. It includes details such as your personal information, treatment received, and costs incurred. This form initiates the reimbursement process for both primary and secondary insurance claims.
- Itemized Statement: Should you need a more detailed breakdown of charges than what is provided in the hospital bill, an itemized statement can be requested. This form lists all services rendered, including individual charges for each service or procedure, helping you understand what you are being billed for.
- Patient Registration Form: This is typically filled out when you first arrive at the hospital or healthcare facility. This document collects essential personal information, including your contact details, emergency contacts, and insurance information. Accurate completion is vital for the processing of your hospital billing.
- Payment Plan Agreement: If you cannot pay your bill in full upon receipt, you may wish to discuss a payment plan with the hospital's financial services. This agreement outlines the terms of your payment arrangement, including the total amount owed, payment frequency, and duration of the plan.
- Financial Assistance Application: Many hospitals offer financial assistance programs to help patients who struggle to pay their bills. This application assesses your financial situation to determine your eligibility for discounts or charity care, which can significantly reduce your out-of-pocket expenses.
Understanding these documents not only assists in resolving any billing issues effectively but also empowers you as a patient. Ensuring that each form is correctly filled out and submitted can facilitate smoother interactions with healthcare providers and insurance companies, allowing you to focus more on your health and wellbeing.
Similar forms
- Invoice: Like a hospital bill, an invoice outlines the services provided along with the total amount due. Both documents serve as a request for payment and detail the specific charges.
- Receipt: After payment is processed, a receipt is provided, confirming the transaction. Both the hospital bill and the receipt document financial exchanges, although the former requests payment, while the latter confirms it.
- Insurance Explanation of Benefits (EOB): This document explains what costs an insurance provider will cover for medical services. Similar to a hospital bill, it details services rendered and can include amounts owed by the patient after insurance payments.
- Credit Card Statement: A credit card statement summarizes transactions made within a billing cycle. Like a hospital bill, it displays amounts owed; however, it encompasses all purchases rather than focusing solely on medical services.
- Payment Plan Agreement: If a patient opts for a payment plan, this document outlines the terms and amounts to be paid over time. Both documents address financial responsibilities relating to medical care, but the agreement frames the repayment structure.
- Billing Statement for Utilities: This statement lists services provided, the amount due, and payment instructions, much like a hospital bill. Both documents aim to collect payment for services rendered.
- Property Tax Bill: A property tax bill details the taxes owed on real estate. It functions similarly to a hospital bill in that it establishes a clear amount owed for services—here, municipal services rather than health services.
- Subscription Renewal Notice: This notice informs subscribers of their next payment due date and amount for services they receive, drawing parallels to a hospital bill informing patients of amounts owed after receiving care.
- Loan Payment Statement: Like a hospital bill, this document outlines the amount due on a specific date. Both serve the purpose of detailing financial obligations, albeit for different types of services.
- Professional Service Invoice: Whether a graphic designer or a consultant issues it, this invoice demands payment for services provided. Similar to a hospital bill, it details services rendered and indicates a total amount due.
Dos and Don'ts
When filling out the Hospital Bill form, certain practices can help ensure a smoother process. Below are some do's and don'ts to consider:
- Do fill out the form accurately and completely to minimize processing errors.
- Don't leave any fields blank, unless they are clearly optional. Incomplete forms can delay payment.
- Do double-check your account number and personal information for accuracy.
- Don't forget to indicate any changes in your address or insurance information, as this could affect billing.
- Do sign the form if it requires a signature, particularly when making payments by credit card.
- Don't neglect to include the payment amount due; make sure this is clearly indicated.
- Do include the invoice date if it is specified on the form.
- Don't use any form of payment other than those specified; for instance, checks may need to be made payable to Froedtert Hospital.
- Do keep a copy of the completed bill form and payment for your records.
Following these guidelines can assist in a more efficient billing experience.
Misconceptions
Understanding hospital bills can be challenging. Many people hold misconceptions about what the Hospital Bill form represents and how it operates. Here are eight common misconceptions, along with clarifications for each:
- It represents the final amount owed. Many believe the amount on the bill is the total they owe after insurance has adjusted charges. However, this amount may change based on any further adjustments from insurers or payments made after the statement was issued.
- You must pay the entire amount immediately. Some people think they must pay the balance in full upon receipt. In fact, many hospitals offer payment plans for those who cannot pay the total amount right away.
- The hospital receives the entire payment. A common misconception is that hospitals keep the full payment made by patients. In reality, a portion generally goes to the healthcare providers and other associated entities.
- All charges are covered by insurance. Many assume their insurance will cover all expenses listed on the bill. Insurance policies may have exclusions or limits, meaning patients could be responsible for certain charges.
- You cannot dispute any charges. Some individuals mistakenly believe that the billed amount is fixed and cannot be contested. Patients have the right to ask for clarifications or appeal certain charges if they seem incorrect or unexpected.
- Emergencies always result in high bills. It is often thought that any emergency visit will incur exorbitant fees. While emergency care can be expensive, many factors influence costs, including the severity of the condition and insurance coverage.
- Your insurance company handles everything. Many believe that once they submit documents, their insurer will take care of all charges. Patients should monitor their insurance claims and ensure their providers are billing accurately.
- Hospital bills are straightforward and include itemized details. It is a common assumption that every hospital bill breaks down charges neatly. Often, itemized bills may require a separate request or call to Patient Financial Services for clarification.
By addressing these misconceptions, patients can engage more effectively with their healthcare providers and manage their finances better after receiving care.
Key takeaways
Completing and submitting a hospital bill form is an important task that ensures the timely processing of your payment. The following key takeaways provide essential information for effectively handling this document.
- Payment Due Upon Receipt: The total amount due, as specified in the form, is required immediately upon receipt. It is crucial to adhere to this timeline to avoid any late fees or interruptions in service.
- Correctly Filling Out Personal Information: Ensure all personal details on the form, such as name, address, and insurance information, are accurate. Any discrepancies can lead to delays in processing your payment.
- Choose Your Payment Method: If paying by credit card, fill out the credit card information section meticulously. Online payment options are also available via the provided website for added convenience.
- Keep Documentation: It is advisable to retain a copy of the completed bill form and any correspondence regarding your payment. This documentation may be necessary for any disputes or clarifications that arise in the future.
Following these guidelines will help streamline the payment process and ensure that your healthcare provider receives the necessary funds in a timely manner.
Browse Other Templates
I765ws Form - Each applicant must fill out their own I-765WS without relying on others.
How to Renew Perc Card - Having previous convictions does not automatically disqualify applicants; context and documentation are considered.
Ca Dmv Permit Test - Clear instructions on how to fill out the form are provided for students.