Fill Out Your Hs 215A Form
The HS 215A form plays a crucial role in the licensing process for health facilities in California, serving as a necessary component of the application package submitted to the California Department of Public Health. This form collects essential information from individuals associated with the applicant facility, such as owners, administrators, and directors. It requires them to disclose identifying information, including names, titles, and business addresses, as well as details about any previous or current involvement in health or community care facilities. The HS 215A form not only seeks this background information for licensure purposes, but it also addresses important matters like criminal records and professional licenses. Individuals must provide a summary of their employment history over the last ten years, highlighting experiences relevant to the health facility in question. Furthermore, the form includes a section focused on any adverse actions associated with past involvements, ensuring transparency in the applicants’ professional history. With its emphasis on disclosure and comprehensive evaluation, the HS 215A is essential for maintaining the standards of care within California’s health services landscape.
Hs 215A Example
State of California – Health and Human Services Agency |
California Department of Public Health |
|
Licensing and Certification |
|
FOR DEPARTMENTAL USE ONLY |
District: |
ELMS Facility Number: |
Proposed name of facility/agency/clinic: |
|
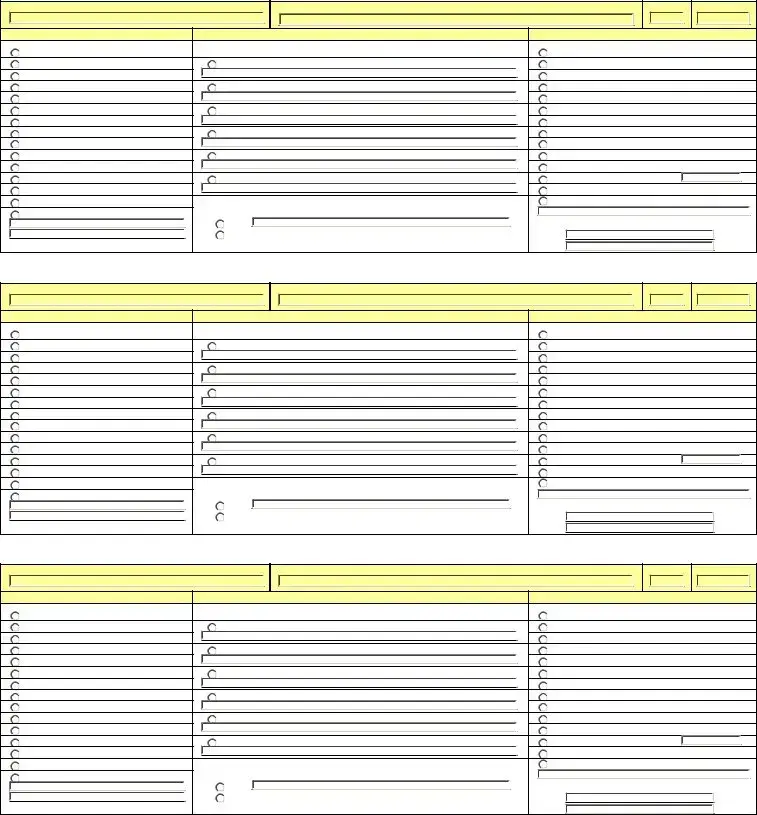
APPLICANT INDIVIDUAL INFORMATION
This form is intended for any individual owning the applicant facility or for any individual involved (now or in the past) with any health or community care facility. Refer to the INSTRUCTION SHEET to see who needs to complete this form.
This HS 215A form needs to be completed as part of an application package plus it needs to be completed for disclosure purposes when changes are reported in officers, directors, purchase of stock, etc., as required by law, even though no change in legal ownership is occurring.
A. Identifying Information
Name
Business address (number, street, apartment/suite number or letter if applicable)
Title in relation to this facility
Date of Birth
City, State, & Zip
Have you applied for ANY license for a health facility or community care facility using any name other than your true full name? If yes, list all other names.
If an Administrator for proposed clinic, list hours that will be spent at the clinic each week. If an Administrator at more than one licensed clinic, list the name of each clinic and the number of hours spent in each licensed clinic per week.
B.Criminal Record
1.Have you ever been convicted of an offense that is still on your record, whether misdemeanor or felony? Yes
Yes  No
No
2. Has there been a judgment against you for Medicare or Medicaid |
Yes |
No |
professional/technical licensing entity? |
If yes to questions 1 or 2 above, please explain and provide dates and conviction information (attach additional pages if necessary):
C.Professional Licenses/Certificates – This requirement is mandatory for Primary Care Clinics and optional for Health facilities.
TYPE |
|
PERIOD HELD |
|
ISSUING AGENCY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HS 215A (2/08) |
1 |
State of California – Health and Human Services Agency |
California Department of Public Health |
|
Licensing and Certification |
D.Employment/Business Summary (for last 10 years). Please list any additional experience
that qualifies you to operate this type of facility. Begin with your most recent job. Attach additional pages if necessary.
Name and address of employer |
Job title |
From: 
To:
From: 
To:
From: 
To:
From: 
To:
E. Facility, Agency, Clinic Involvement (in or out of California)
The questions below are for “individuals” and do not pertain to the facility that is applying for licensure.
1.Have you ever been involved with a business entity that operated a health facility or community care facility?
Yes |
No |
If YES, complete Section F (below) and the “Facility Information Sheet” (attached). |
2.Have you ever operated or managed (including management agreements) any of the following facility types?
Yes |
No |
If YES, complete Section F (below) and the “Facility Information Sheet” (attached). |
||
|
|
|
|
|
|
|
Adult Day Health Care Center |
ICF/DD |
|
|
|
Clinics |
|
|
|
|
COMMUNITY CARE FACILITY |
|
|
|
|
General Acute Care Hospital |
Intermediate Care Facility |
|
|
|
Health Facility |
Pediatric Day Health & Respite Care |
|
|
|
Home Health Agency |
Residential Care Facility for the Elderly |
|
|
|
Hospice |
Skilled Nursing Facility |
|
|
|
|
Other |
|
3.Have you ever held a 5 percent or more beneficial ownership interest in any of the facility types above?
Yes |
No If YES, complete Section F (below) and the “Facility Information Sheet” (attached). |
F. Adverse Actions
Have you been affiliated with any facility, either past or present, that has been identified as having one or more of the
following adverse actions? |
Yes |
No |
If YES, check all applicable: |
|
|
Had a final |
|
Placed on probation |
Receiver appointed |
||
Resolved by settlement |
Revocation action filed |
Revoked (whether stayed or not) |
Suspension |
||
If yes, please explain (including facility name and address). Attach additional pages if necessary:
I declare under penalty of perjury that the statements on this form and any accompanying attachments are correct to the best of my knowledge.
Signature: |
Date: |
|
RELEASE OF INFORMATION STATEMENT
The information provided on this form is mandatory and is necessary for licensure approval. It will be used to determine individual applicant’s or applicant facility’s ability to provide health services. The information is requested by the California Department of Public Health, Licensing and Certification, in accordance with the Health and Safety Code. Failure to provide the information as requested may result in nonissuance of a license or license revocation. The information is considered public information and will be made available to the public upon request. The information shall be included and maintained in the individual facility’s public files located in Licensing and Certification district offices.
HS 215A (2/08) |
2 |
State of California – Health and Human Services Agency |
California Department of Public Health |
|
Licensing and Certification |
FACILITY INFORMATION SHEET
You are required to complete the following for each facility (including all facilities in all business entities) with which you have a current relationship or have had a past relationship (going back 3 years). Refer to the INSTRUCTION SHEET.
Facility name: |
Facility address (number, street, city): |
State: |
Zip code: |
Type of Facility |
“Type” of Business Entity |
Individual’s “Nature” of Involvement |
|
Adult Day Health Care Center |
For EACH business entity, identify the name & EIN of the entity: |
Administrator of Clinic, SNF or ICF |
|
Clinic |
Corporation: |
Agent |
|
COMMUNITY CARE FACILITY |
|
Director |
|
General Acute Care Hospital |
Individual: |
Licensee |
|
Health Facility |
|
Manager of “parent” organization |
|
HHA |
LLC: |
Managing employee of a HHA |
|
Hospice |
|
Member |
|
ICF |
Management Company: |
Officer of corporation |
|
ICF/DD |
|
Owner |
|
Partnership: |
Partner |
|
|
|
Sole Proprietorship |
|
|
ICF |
OTHER Business Entity (explain): |
Stockholder |
|
Residential Care for the Elderly |
Are any of the above Business Entities a “PARENT” organization to the |
Trustee |
|
SNF |
OTHER Nature of Involvement (explain): |
||
OTHER FACILITY TYPE (explain): |
applicant facility? If Yes, explain. |
|
|
|
Yes |
Dates of involvement: |
|
|
No |
From: |
|
|
|
To: |
|
Facility name: |
Facility address (number, street, city): |
State: |
Zip code: |
Type of Facility |
“Type” of Business Entity |
Individual’s “Nature” of Involvement |
|
Adult Day Health Care Center |
For EACH business entity, identify the name & EIN of the entity: |
Administrator of Clinic, SNF or ICF |
|
Clinic |
Corporation: |
Agent |
|
COMMUNITY CARE FACILITY |
|
Director |
|
General Acute Care Hospital |
Individual: |
Licensee |
|
Health Facility |
|
Manager of “parent” organization |
|
HHA |
LLC: |
Managing employee of a HHA |
|
Hospice |
|
Member |
|
ICF |
Management Company: |
Officer of corporation |
|
ICF/DD |
|
Owner |
|
Partnership: |
Partner |
|
|
|
Sole Proprietorship |
|
|
ICF |
OTHER Business Entity (explain): |
Stockholder |
|
Residential Care for the Elderly |
Are any of the above Business Entities a “PARENT” organization to the |
Trustee |
|
SNF |
OTHER Nature of Involvement (explain): |
||
OTHER FACILITY TYPE (explain): |
applicant facility? If Yes, explain. |
|
|
|
Yes |
Dates of involvement: |
|
|
No |
From: |
|
|
|
To: |
|
Facility name: |
Facility address (number, street, city): |
State: |
Zip code: |
Type of Facility |
“Type” of Business Entity |
Individual’s “Nature” of Involvement |
|
Adult Day Health Care Center |
For EACH business entity, identify the name & EIN of the entity: |
Administrator of Clinic, SNF or ICF |
|
Clinic |
Corporation: |
Agent |
|
COMMUNITY CARE FACILITY |
|
Director |
|
General Acute Care Hospital |
Individual: |
Licensee |
|
Health Facility |
|
Manager of “parent” organization |
|
HHA |
LLC: |
Managing employee of a HHA |
|
Hospice |
|
Member |
|
ICF |
Management Company: |
Officer of corporation |
|
ICF/DD |
|
Owner |
|
Partnership: |
Partner |
|
|
|
Sole Proprietorship |
|
|
ICF |
OTHER Business Entity (explain): |
Stockholder |
|
Residential Care for the Elderly |
Are any of the above Business Entities a “PARENT” organization to the |
Trustee |
|
SNF |
OTHER Nature of Involvement (explain): |
||
OTHER FACILITY TYPE (explain): |
applicant facility? If Yes, explain. |
|
|
|
Yes |
Dates of involvement: |
|
|
No |
From: |
|
|
|
To: |
|
HS 215A (2/08) |
3 |
State of California – Health and Human Services Agency |
California Department of Public Health |
|
Licensing and Certification |
Facility name: |
Facility address (number, street, city): |
State: |
Zip code: |
Type of Facility |
“Type” of Business Entity |
Individual’s “Nature” of Involvement |
|
Adult Day Health Care Center |
For EACH business entity, identify the name & EIN of the entity: |
Administrator of Clinic, SNF or ICF |
|
Clinic |
Corporation: |
Agent |
|
COMMUNITY CARE FACILITY |
|
Director |
|
General Acute Care Hospital |
Individual: |
Licensee |
|
Health Facility |
|
Manager of “parent” organization |
|
HHA |
LLC: |
Managing employee of a HHA |
|
Hospice |
|
Member |
|
ICF |
Management Company: |
Officer of corporation |
|
ICF/DD |
|
Owner |
|
Partnership: |
Partner |
|
|
|
Sole Proprietorship |
|
|
ICF |
OTHER Business Entity (explain): |
Stockholder |
|
Residential Care for the Elderly |
Are any of the above Business Entities a “PARENT” organization to the |
Trustee |
|
SNF |
OTHER Nature of Involvement (explain): |
||
OTHER FACILITY TYPE (explain): |
applicant facility? If Yes, explain. |
|
|
|
Yes |
Dates of involvement: |
|
|
No |
From: |
|
|
|
To: |
|
Facility name: |
Facility address (number, street, city): |
State: |
Zip code: |
Type of Facility |
“Type” of Business Entity |
Individual’s “Nature” of Involvement |
|
Adult Day Health Care Center |
For EACH business entity, identify the name & EIN of the entity: |
Administrator of Clinic, SNF or ICF |
|
Clinic |
Corporation: |
Agent |
|
COMMUNITY CARE FACILITY |
|
Director |
|
General Acute Care Hospital |
Individual: |
Licensee |
|
Health Facility |
|
Manager of “parent” organization |
|
HHA |
LLC: |
Managing employee of a HHA |
|
Hospice |
|
Member |
|
ICF |
Management Company: |
Officer of corporation |
|
ICF/DD |
|
Owner |
|
Partnership: |
Partner |
|
|
|
Sole Proprietorship |
|
|
ICF |
OTHER Business Entity (explain): |
Stockholder |
|
Residential Care for the Elderly |
Are any of the above Business Entities a “PARENT” organization to the |
Trustee |
|
SNF |
OTHER Nature of Involvement (explain): |
||
OTHER FACILITY TYPE (explain): |
applicant facility? If Yes, explain. |
|
|
|
Yes |
Dates of involvement: |
|
|
No |
From: |
|
|
|
To: |
|
Facility name: |
Facility address (number, street, city): |
State: |
Zip code: |
Type of Facility |
“Type” of Business Entity |
Individual’s “Nature” of Involvement |
|
Adult Day Health Care Center |
For EACH business entity, identify the name & EIN of the entity: |
Administrator of Clinic, SNF or ICF |
|
Clinic |
Corporation: |
Agent |
|
COMMUNITY CARE FACILITY |
|
Director |
|
General Acute Care Hospital |
Individual: |
Licensee |
|
Health Facility |
|
Manager of “parent” organization |
|
HHA |
LLC: |
Managing employee of a HHA |
|
Hospice |
|
Member |
|
ICF |
Management Company: |
Officer of corporation |
|
ICF/DD |
|
Owner |
|
Partnership: |
Partner |
|
|
|
Sole Proprietorship |
|
|
ICF |
OTHER Business Entity (explain): |
Stockholder |
|
Residential Care for the Elderly |
Are any of the above Business Entities a “PARENT” organization to the |
Trustee |
|
SNF |
OTHER Nature of Involvement (explain): |
||
OTHER FACILITY TYPE (explain): |
applicant facility? If Yes, explain. |
|
|
|
Yes |
Dates of involvement: |
|
|
No |
From: |
|
|
|
To: |
|
HS 215A (2/08) |
4 |
State of California – Health and Human Services Agency |
California Department of Public Health |
|
Licensing and Certification |
INSTRUCTIONS FOR HS 215A
The HS 215A must contain an original signature and date. The date of this form should be within the last three months.
This form is intended for the following:
1. Any individual owning an applicant facility;
2. Each agent, each partner, each director, each member, each managing employee of a HHA, each officer of a corporation;
3. Each agent, each partner, each director, each officer, each member or manager of a parent organization of licensee applicant; Each manager, each member of a limited liability company;
Administrators;
Each person having a beneficial interest of 5 percent or more in the applicant corporation, applicant limited liability company, applicant partnership, applicant management company, applicant facility or private agency; and
7. Each officer and each director of the parent of the management company. |
||
|
District office and ELMS Number |
To be completed by the California Department of Public Health |
|
Proposed name of facility/agency/clinic |
Enter the name of your facility as it appears on your application (HS 200). |
A. IDENTIFYING INFORMATION |
|
|
|
Name |
Please enter your full legal name. |
|
Date of birth |
Day/Month/Year |
|
|
|
|
Business Address |
Location of your business; number, street, apartment/suite number or letter if applicable. |
|
|
|
|
City |
City where business is located. |
|
|
|
|
State |
State where business is located. |
|
|
|
|
Zip code |
Zip code where business is located |
|
|
|
|
Title in relation to this facility |
Your title in relation to this facility. |
|
If an Administrator for proposed clinic, list hours |
Please list hours spent at each clinic per week. If your title is not administrator, please list N/A. |
|
that will be spent at the clinic each week. If an |
|
|
Administrator at more than one licensed clinic, |
|
|
list the name of each clinic and the number of |
|
|
hours spent in each licensed clinic per week. |
|
|
Have you applied for any license for a health |
Please answer yes or no. If yes, list any other names you have used if you have ever applied for a |
|
facility or community care facility regardless of |
health facility or community care facility license. |
|
your role or title using any name other than your |
|
|
true full name? If yes, list all other names. |
|
B. CRIMINAL RECORD
Please check appropriate box. If you have checked ‘yes’, please provide dates and conviction information. If not applicable, please enter ‘N/A’.
C. PROFESSIONAL LICENSES/CERTIFICATES |
|
Type |
Type of licenses or certificate that you hold. |
Period held |
Dates that you held your license. |
Issuing Agency |
Agency that issued you a license and/or certificate. |
D.EMPLOYMENT/BUSINESS SUMMARY (FOR LAST 10 YEARS). Please list any additional experience that qualifies you to operate this type of facility. If self employed, never worked or now retired, indicate the ‘From’ and ‘To’ dates. Begin with your most recent job. Attach additional pages if necessary.
|
|
Dates (From/To) |
Dates that you were employed in position from the start to the end date. |
Name and Address of Employer(s) |
Name and street, city, state address of the employer. |
Job Title |
Title that you held within your company/place of employment. |
|
|
E. FACILITY, AGENCY, CLINIC INVOLVEMENT (IN OR OUT OF CALIFORNIA) |
|
Questions No. |
Please check appropriate box(es). If you have checked yes, you must fill out the attached “Facility |
|
Information Sheet” and complete Section F. |
F. ADVERSE ACTIONS |
|
Please check appropriate box. If box is checked yes, please explain and include facility information. |
|
FACILITY INFORMATION SHEET |
|
Facility Name |
Name of Facility that correlates to the checkboxes you have checked as ‘yes’ in Section E. |
Facility address |
Number and street address of the facility involved. |
City |
City where facility is located. |
State |
State where facility is located. |
ZIP code |
Zip code where facility is located. |
Type of Facility |
Check appropriate health facility. |
“Type” of Business Entity |
Check appropriate business entity and identify if this entity is a “parent” corporation to the applicant |
|
facility. |
Individual “Nature” of Involvement |
Check appropriate position held at that facility. |
HS 215A (2/08) |
5 |
Form Characteristics
| Fact Name | Details |
|---|---|
| Governing Authority | The HS 215A form is governed by California Health and Safety Code regulations. |
| Purpose | This form is used to gather essential information about individuals owning or involved with health facilities in California. |
| Required Signatures | Each applicant must provide an original signature along with a date on the form. |
| Application Context | The HS 215A form is part of the application package and is necessary for license approval. |
| Criminal History Disclosure | Applicants must disclose any convictions, including misdemeanors and felonies. |
| Facility Involvement | The form collects information regarding any past involvement with facilities, both in and out of California. |
| Professional Licensing Requirement | Providing the details of any professional licenses or certifications is mandatory for certain types of clinics. |
| Adverse Actions Disclosure | Applicants must report any adverse actions taken against them or facilities they have been associated with. |
| Public Information | Information provided on this form is considered public and may be disclosed upon request. |
| Updating Information | The form must be updated if any changes occur regarding individual circumstances, such as ownership stakes. |
Guidelines on Utilizing Hs 215A
Completing the HS 215A form is essential for individuals involved with a health or community care facility in California. This process requires detailed personal information, professional experience, and disclosures about any affiliations or adverse actions related to health facilities. Completing this form accurately aids in the assessment of an applicant’s qualifications for licensure.
- Begin with the DEPARTMENTAL USE ONLY section. Leave this part blank as it's for the California Department of Public Health.
- Enter the Proposed name of facility/agency/clinic as stated in your application (HS 200).
- Fulfill the APPLICANT INDIVIDUAL INFORMATION section:
- Provide your full Name.
- Fill in your Business address (number, street, and any applicable apartment/suite number).
- State your Title in relation to the facility.
- Input your Date of Birth.
- Indicate your City, State, & Zip.
- Answer the question regarding any previous license applications using a different name. If applicable, list all other names used.
- If you are the Administrator, include the hours spent at the clinic weekly. If managing multiple clinics, list each clinic's name and the hours for each.
- Next, complete the CRIMINAL RECORD section:
- Check 'Yes' or 'No' for any convictions still on record.
- Answer whether you have faced any judgments regarding Medicare or Medicaid fraud. If 'Yes', provide details.
- Proceed to PROFESSIONAL LICENSES/ CERTIFICATES:
- List the type of licenses held, the period you held them, and the issuing agency.
- Provide your EMPLOYMENT/ BUSINESS SUMMARY for the last ten years:
- Start with your most recent job.
- Include your Name and address of employer, Job title, and Dates of employment.
- Fill out the FACILITY, AGENCY, CLINIC INVOLVEMENT section:
- Answer whether you have been involved with any health or community care facilities. If 'Yes', complete the attached Facility Information Sheet.
- Next, address the ADVERSE ACTIONS:
- Check applicable boxes if you have been affiliated with any facility that faced adverse actions. Provide explanations and facility information if necessary.
- Finally, include your signature and date at the bottom. Ensure the statement is dated within the last three months.
What You Should Know About This Form
What is the HS 215A form used for?
The HS 215A form is a mandatory document required by the California Department of Public Health. It is intended for individuals who own or have been involved with a health or community care facility. This form collects essential information about the applicant’s criminal background, professional licenses, and employment history. It's important to ensure that the form is completed accurately, as it must be submitted as part of an application package for licensure.
Who needs to fill out the HS 215A form?
The HS 215A form must be completed by various individuals tied to the applicant facility. This includes the owner, partners, directors, managing employees, and anyone who holds a significant interest (5% or more) in the facility. It is also required from individuals connected to a parent organization involved with the license application. In essence, anyone with a managerial or ownership role within the facility must provide their information.
What information do I need to provide on the HS 215A form?
When completing the HS 215A form, you'll need to provide personal identifying information like your name, business address, and title related to the facility. You are also required to disclose any previous names you have used in license applications. The section on criminal records asks about any convictions, including misdemeanors or felonies. Additionally, professional licenses held, employment history for the past decade, and details about any previous involvement with other facilities will need to be included.
Are there any consequences if I don’t fill out the HS 215A form?
Failing to complete the HS 215A form or providing inaccurate information can result in significant consequences. The California Department of Public Health requires this form for license approval, and missing or misleading information may lead to delays or denial of your application. In some cases, it may even result in revocation of an existing license. Therefore, it is vital to approach this form with care and ensure that all provided information is truthful and complete.
How does the criminal record section work?
The criminal record section of the HS 215A form requires you to respond to two key questions: if you have any convictions on your record and if you have faced judgments related to Medicare or Medicaid fraud. If you answer "yes" to either question, you must provide further details, including the nature of the offense and dates. This transparency is essential as it helps the Department assess your suitability for operating a healthcare facility.
What should I do if I need assistance with the HS 215A form?
If you find yourself needing assistance while filling out the HS 215A form, consider reaching out to a legal consultant or a compliance specialist familiar with health facility licensure in California. They can provide guidance on how to accurately complete the form and answer any questions you may have. Additionally, the California Department of Public Health often offers resources and instructions that can clarify any uncertainties you might encounter during the process.
Common mistakes
Completing the HS 215A form can be a straightforward process, but many applicants make common mistakes that can lead to delays or even denials in their application. One prevalent error is failing to use the full legal name. Individuals sometimes provide nicknames or shortened versions of their names instead of the complete legal name as it appears on official documents. This can confuse reviewers and complicate the verification process.
Another mistake involves incomplete contact information. List all relevant details accurately, including the complete business address, apartment or suite numbers, and ZIP code. Omitting any of this information can lead to delays in communication between the applicant and the California Department of Public Health.
Some applicants overlook the need to disclose any other names they may have used when applying for licenses. If someone has previously applied for a health facility license under a different name, failing to mention it can raise concerns about transparency. Always be forthcoming about past names to avoid complications.
Additionally, many people forget to provide their title in relation to the facility. This is a critical part of the identification process. Without it, the reviewing agency may have difficulty understanding your role, potentially impacting the evaluation of your application.
When it comes to the criminal record section, applicants might fail to explore their history thoroughly. Forgetting past convictions, even minor ones, can lead to inconsistencies in your application. If there are any past issues, it is essential to provide accurate information and context. Ignoring this can be seen as misleading.
In the section regarding employment and business history, providing vague job descriptions also creates confusion. Instead of simply listing positions held, be specific about the roles and how they relate to the operation of a health facility. This context helps reviewers assess qualifications more effectively.
Another frequent oversight involves the Adverse Actions section. Some individuals may check "No" without thoroughly considering their past affiliations with health facilities. It’s important to provide accurate information in this section, as discrepancies can lead to serious implications for your application.
Lastly, failing to sign and date the form appropriately is a mistake that can be easily avoided. The application requires an original signature and the date must be within the last three months. Neglecting this requirement results in unnecessary back-and-forth with the reviewing agency, delaying the entire process.
By being aware of these common mistakes, applicants can prepare their HS 215A forms more effectively and increase their chances of a smooth application process.
Documents used along the form
The HS 215A form is a key component in the application process for licensing health and community care facilities in California. However, it's often accompanied by various other forms and documents that provide additional information about the applicant and their facilities. Below is a list of documents commonly used alongside the HS 215A form.
- Facility Information Sheet: This document outlines the details of each facility the individual has been affiliated with, including names, addresses, and the nature of their involvement.
- Application for Licensure (HS 200): This primary application form provides basic information about the facility, including its name, address, and type, and must be submitted for licensing consideration.
- Disclosure Statement: This statement contains information related to the ownership and management of the facility. It may include details about any related entities or partners and their respective roles.
- Background Check Authorization: Required for conducting a thorough background check on the applicant, this form ensures compliance with state regulations regarding criminal history and qualifications.
- Professional Licenses/Certificates: A list of relevant licenses or certifications must also be submitted, especially for administrators of health facilities, detailing the type, issuing agency, and validity periods.
- Resume or Curriculum Vitae: A current resume is often needed, showing the applicant’s employment history, educational background, and relevant experience in health care settings.
- Financial Disclosure Form: This form requires the applicant to provide financial information about the facility, including funding sources, financial support, and budgetary details.
- Evidence of Insurance: Proof of liability insurance is typically necessary, demonstrating that the facility has adequate coverage to operate safely and comply with state regulations.
- Policy and Procedure Manual: A comprehensive manual that outlines the facility’s operational policies and procedures, which is often reviewed during the licensing process.
- Patient Rights and Responsibilities Document: This form informs patients about their rights and responsibilities while receiving care at the facility, ensuring compliance with ethical and legal standards in patient care.
Submitting these forms and documents along with the HS 215A will help create a robust application package. It's crucial that they are completed accurately and submitted in a timely manner to avoid delays in the licensing process. Being thorough and transparent is key to establishing credibility with the licensing authorities.
Similar forms
- HS 200 Form: This form is used as part of the application package for licensing health facilities, similar to HS 215A. Both require comprehensive applicant information and details about the facility.
- HS 220 Form: Similar in intent, the HS 220 collects information on compliance with health and safety regulations, much like HS 215A’s requirements for reporting on ownership and management.
- HS 216 Form: While this document focuses on operational plans for facilities, it shares the objective of ensuring that applicants meet necessary legal standards, akin to the HS 215A.
- Facility Information Sheet: Directly related to HS 215A, this sheet gathers specific facility details for licensure. It requires owners and operators to disclose relevant history and affiliations.
- California Department of Public Health Application for License: Much like the HS 215A, this application gathers essential data from applicants to assess their qualifications and history in operating health facilities.
- HS 106 Form: This form documents changes in ownership or operations for existing facilities and has similar requirements to report changes in management as seen in HS 215A.
- Health Facility Licensing Application: Its purpose is to evaluate new applicants to ensure they adhere to state laws and regulations, paralleling the disclosures required in HS 215A.
- Application for Medicaid License: Medicaid licensing applications share the goal of verifying eligibility and background of facility operators, similar to the HS 215A form's focus on criminal background and business history.
- Community Care Licensing Application: This document screens applicants for community care facilities and includes elements related to ownership and professional qualifications, much like the HS 215A.
Dos and Don'ts
When completing the HS 215A form, attention to detail is crucial. Here is a list of helpful practices and pitfalls to avoid:
- DO read the instruction sheet thoroughly before filling out the form.
- DON'T leave any sections blank if they are relevant to your situation.
- DO provide your full legal name as it appears on official documents.
- DON'T provide nicknames or abbreviated versions of your name.
- DO include all relevant employment history for the last ten years.
- DON'T exaggerate or falsify your work experience; accuracy is essential.
- DO answer all questions regarding your criminal record honestly.
- DON'T think that past offenses can be omitted; full disclosure is important.
- DO check that your form has been signed and dated within the last three months.
- DON'T submit the form without ensuring that all information is correct and complete.
Following these guidelines will help you avoid common mistakes and ensure a smoother application process.
Misconceptions
Misconceptions about the HS 215A form can create confusion for those navigating the application process for health or community care facilities. Here are nine common myths along with clarifications:
- The HS 215A is only for new applicants. Many believe this form is solely for those applying for a new facility license. In reality, it must be completed for various situations, including reporting changes in ownership or management, even if no new application is involved.
- Only the facility owner needs to fill out the form. It's a common assumption that only the principal owner is required to provide information. However, anyone involved with the facility, such as partners, directors, and key employees, must also complete the form as per the instructions.
- If I have a clean criminal record, I don’t need to worry about this form. Some people think that having no criminal record means the HS 215A is irrelevant for them. However, all required parties must still disclose their past affiliations with health facilities, regardless of convictions.
- Filling out the HS 215A is optional. There is a misconception that this form is optional. This is not true. The information provided is mandatory and necessary for licensure approval by the California Department of Public Health.
- I can submit the form whenever I want. This form must be signed and dated within three months prior to submission. Some mistakenly think there is more flexibility with timing. Adherence to this timeframe is crucial for processing.
- Providing false information is okay as long as it’s not discovered. Some believe they can withhold or alter information without consequence. However, submitting false information can have serious repercussions, including nonissuance or revocation of a license.
- The HS 215A is strictly confidential. Many think that the information disclosed remains private. In fact, the data on this form is part of public records, available to the public upon request.
- All questions on the form are optional. There’s a belief that completing every question isn’t necessary. However, all sections are relevant to the application process and must be answered thoroughly to avoid delays.
- Changes in management don’t need to be reported. Some applicants think that as long as there isn't a change in ownership, they do not need to fill out the HS 215A. This is incorrect. Reporting changes in officers or directors, even without ownership changes, is part of the legal requirements.
Understanding the truths behind these misconceptions is essential for anyone involved in the health and community care sector. Accurate completion of the HS 215A can ensure a smoother licensure process and compliance with all regulations.
Key takeaways
- Understand the Purpose: The HS 215A form is used for individuals involved with health or community care facilities. This includes owners, administrators, and certain key employees.
- Follow the Instructions: Carefully read the instruction sheet to determine who needs to complete the form, as it requires specific information and disclosures.
- Provide Accurate Information: Ensure that all personal details, including your full legal name, business address, and title, are correct, as inaccuracies may delay your application.
- Disclose Criminal Records: If you have any past convictions, truthfully disclose them. This section is crucial for your application's integrity.
- Detail Employment History: List your employment for the last ten years, starting with the most recent position. This demonstrates your qualifications to operate the facility.
- Involvement with Other Facilities: If you have been involved with other health facilities in the past, be sure to indicate this on the form and complete the Facility Information Sheet.
- Adverse Actions: If you have faced any adverse actions against previous facilities, it is essential to disclose these situations. Transparency is key.
- Signature and Date: Remember that the form must be signed and dated. Ideally, this should be done within the last three months to ensure relevancy.
- Public Information: Understand that the information provided is considered public and will be available upon request, so only include information you are comfortable sharing.
Browse Other Templates
Tax Waiver Form Nj - Multiple assets at a single institution may require separate forms.
What Is Va Form 21-4138 Used for - Incomplete information regarding employment or education can lead to complications.