Fill Out Your Icf Checklist Form
The ICF Checklist is a vital tool designed to help clinicians and professionals assess an individual's functioning and disability. This checklist follows the International Classification of Functioning, Disability and Health (ICF) framework established by the World Health Organization. It provides a structured way to gather and document essential information, orienting the evaluation around various aspects of an individual's health and capabilities. The form prompts users to collect details regarding demographic information, medical history, and current health conditions, which are crucial for understanding each person's unique needs. The checklist prioritizes accurate data collection by encouraging the use of multiple sources, such as written records, primary respondents, and direct observations. Moreover, it outlines specific impairment categories related to body functions and structures, allowing users to describe the extent and nature of any identified issues clearly. With its systematic approach, the ICF Checklist serves as a comprehensive resource, aiding in better treatment planning and outcome measurement in clinical and social work contexts.
Icf Checklist Example
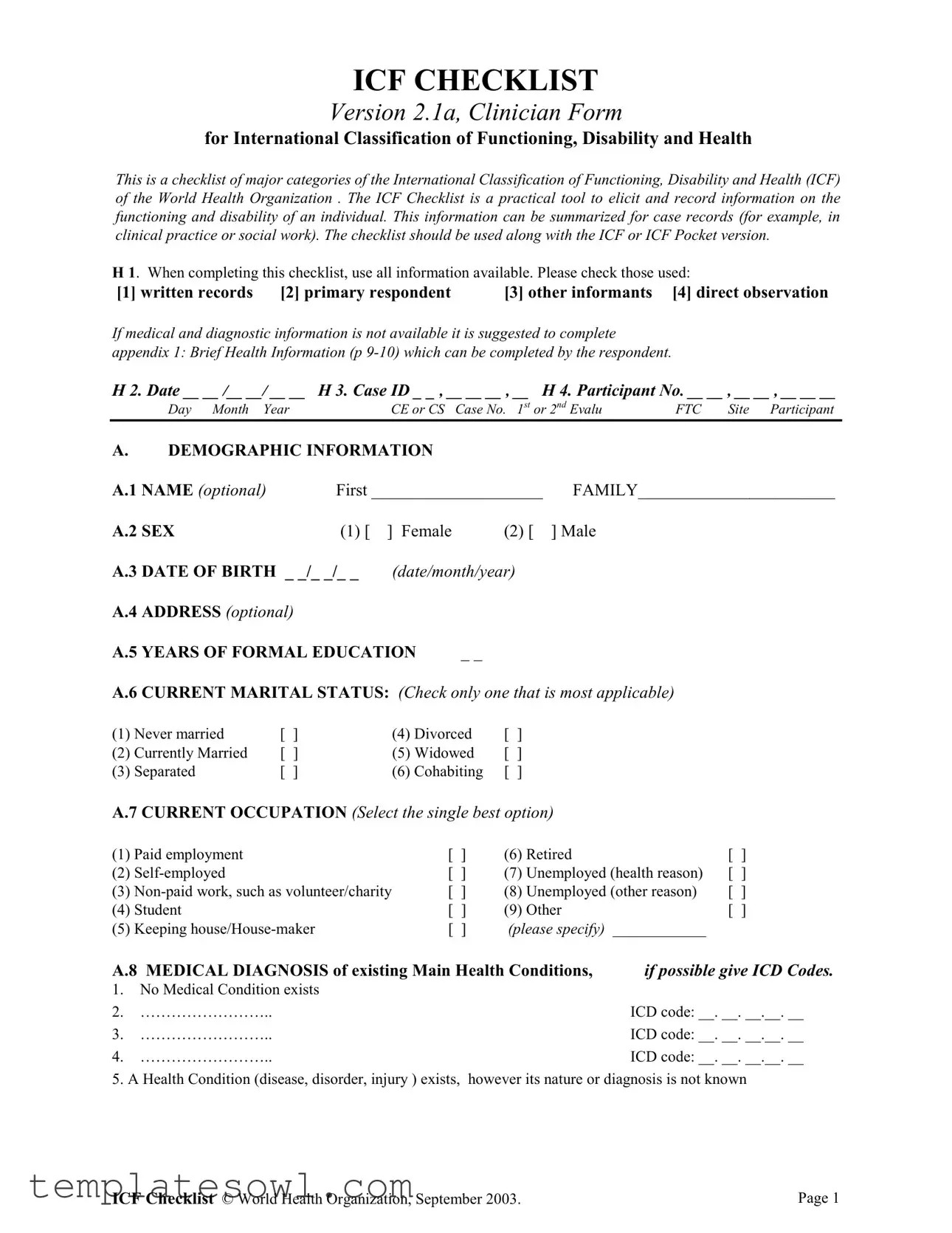
ICF CHECKLIST
Version 2.1a, Clinician Form
for International Classification of Functioning, Disability and Health
This is a checklist of major categories of the International Classification of Functioning, Disability and Health (ICF) of the World Health Organization . The ICF Checklist is a practical tool to elicit and record information on the functioning and disability of an individual. This information can be summarized for case records (for example, in clinical practice or social work). The checklist should be used along with the ICF or ICF Pocket version.
H 1. When completing this checklist, use all information available. Please check those used:
[1] written records |
[2] primary respondent |
[3] other informants |
[4] direct observation |
||
If medical and diagnostic information is not available it is suggested to complete |
|
|
|||
appendix 1: Brief Health Information (p |
|
|
|||
H 2. Date __ __ /__ __/ __ __ |
H 3. Case ID _ _ , __ __ __ , __ H 4. Participant No. __ __ , __ __ , __ __ __ |
||||
Day Month |
Year |
CE or CS |
Case No. 1st or 2nd Evalu |
FTC |
Site Participant |
A.DEMOGRAPHIC INFORMATION
A.1 NAME (optional) |
|
First ____________________ |
FAMILY_______________________ |
||||||||
A.2 SEX |
|
(1) [ |
] Female |
(2) [ |
] Male |
|
|
||||
A.3 DATE OF BIRTH _ _/_ _/_ _ |
(date/month/year) |
|
|
|
|
|
|||||
A.4 ADDRESS (optional) |
|
|
|
|
|
|
|
|
|
||
A.5 YEARS OF FORMAL EDUCATION |
_ _ |
|
|
|
|
|
|
||||
A.6 CURRENT MARITAL STATUS: (Check only one that is most applicable) |
|
||||||||||
(1) |
Never married |
[ ] |
|
(4) Divorced |
[ |
] |
|
|
|
|
|
(2) |
Currently Married |
[ ] |
|
(5) Widowed |
[ |
] |
|
|
|
|
|
(3) |
Separated |
[ ] |
|
(6) Cohabiting |
[ |
] |
|
|
|
|
|
A.7 CURRENT OCCUPATION (Select the single best option) |
|
|
|||||||||
(1) Paid employment |
|
|
|
[ ] |
(6) |
Retired |
|
[ ] |
|||
(2) |
|
|
|
[ ] |
(7) |
Unemployed (health reason) |
[ ] |
||||
(3) |
[ ] |
(8) |
Unemployed (other reason) |
[ ] |
|||||||
(4) |
Student |
|
|
|
[ ] |
(9) |
Other |
|
[ ] |
||
(5) |
Keeping |
|
|
[ ] |
(please specify) ____________ |
|
|||||
A.8 MEDICAL DIAGNOSIS of existing Main Health Conditions, |
if possible give ICD Codes. |
||||||||||
1.No Medical Condition exists
2. |
…………………….. |
ICD code: __. __. __.__. __ |
3. |
…………………….. |
ICD code: __. __. __.__. __ |
4. |
…………………….. |
ICD code: __. __. __.__. __ |
5. A Health Condition (disease, disorder, injury ) exists, however its nature or diagnosis is not known
ICF Checklist © World Health Organization, September 2003. |
Page 1 |
PART 1a: IMPAIRMENTS of BODY FUNCTIONS
•Body functions are the physiological functions of body systems (including psychological functions).
•Impairments are problems in body function as a significant deviation or loss.
First Qualifier: Extent of impairments
0 No impairment means the person has no problem
1 Mild impairment means a problem that is present less than 25% of the time, with an intensity a person can tolerate and which happens rarely over the last 30 days.
2 Moderate impairment means that a problem that is present less than 50% of the time, with an intensity, which is interfering in the persons day to day life and which happens occasionally over the last 30 days.
3 Severe impairment means that a problem that is present more than 50% of the time, with an intensity, which is partially disrupting the persons day to day life and which happens frequently over the last 30 days.
4 Complete impairment means that a problem that is present more than 95% of the time, with an intensity, which is totally disrupting the persons day to day life and which happens every day over the last 30 days.
8 Not specified means there is insufficient information to specify the severity of the impairment.
9 Not applicable means it is inappropriate to apply a particular code (e.g. b650 Menstruation functions for woman in
Short List of Body Functions |
Qualifier |
||
b1. MENTAL FUNCTIONS |
|
||
b110 |
Consciousness |
|
|
b114 |
Orientation |
(time, place, person) |
|
b117 |
Intellectual |
( incl. Retardation, dementia) |
|
|
|
|
|
b130 |
Energy and drive functions |
|
|
b134 Sleep |
|
|
|
|
|
|
|
b140 |
Attention |
|
|
|
|
|
|
b144 Memory |
|
|
|
b152 |
Emotional functions |
|
|
b156 Perceptual functions |
|
||
|
|
|
|
b164 |
Higher level cognitive functions |
|
|
b167 |
Language |
|
|
b2. SENSORY FUNCTIONS AND PAIN |
|
||
b210 Seeing |
|
|
|
b230 |
Hearing |
|
|
b235 Vestibular (incl. Balance functions) |
|
||
|
|
|
|
b280 Pain |
|
|
|
b3. VOICE AND SPEECH FUNCTIONS |
|
||
b310 Voice |
|
|
|
|
|
||
b4. FUNCTIONS OF THE CARDIOVASCULAR, HAEMATOLOGICAL, |
|
||
IMMUNOLOGICAL AND RESPIRATORY SYSTEMS |
|
||
b410 Heart |
|
|
|
b420 Blood pressure |
|
||
|
|
||
b430 Haematological (blood) |
|
||
|
|
||
b435 Immunological (allergies, hypersensitivity) |
|
||
b440 Respiration (breathing) |
|
||
b5. FUNCTIONS OF THE DIGESTIVE, METABOLIC AND ENDOCRINE SYSTEMS |
|
||
b515 |
Digestive |
|
|
b525 |
Defecation |
|
|
b530 |
Weight maintenance |
|
|
|
|
|
|
b555 |
Endocrine glands (hormonal changes) |
|
|
b6. GENITOURINARY AND REPRODUCTIVE FUNCTIONS |
|
||
b620 |
Urination functions |
|
|
|
|
|
|
b640 Sexual functions
b7. NEUROMUSCULOSKELETAL AND MOVEMENT RELATED FUNCTIONS
b710 Mobility of joint
b730 Muscle power
b735 Muscle tone
b765 Involuntary movements
b8. FUNCTIONS OF THE SKIN AND RELATED STRUCTURES
ANY OTHER BODY FUNCTIONS
Part 1 b: IMPAIRMENTS of BODY STRUCTURES
•Body structures are anatomical parts of the body such as organs, limbs and their components.
•Impairments are problems in structure as a significant deviation or loss.
|
First Qualifier: Extent of impairment |
Second Qualifier: Nature of the change |
||
|
0 No impairment means the person has no problem |
0 |
No change in structure |
|
|
1 Mild impairment means a problem that is present less than 25% |
1 Total absence |
|
|
|
of the time, with an intensity a person can tolerate and which |
2 |
Partial absence |
|
|
happens rarely over the last 30 days. |
3 |
Additional part |
|
|
2 Moderate impairment means that a problem that is present less |
4 |
Aberrant dimensions |
|
|
than 50% of the time, with an intensity, which is interfering in the |
5 |
Discontinuity |
|
|
persons day to day life and which happens occasionally over the |
6 |
Deviating position |
|
|
last 30 days. |
7 |
Qualitative changes in structure, including |
|
|
3 Severe impairment means that a problem that is present more |
accumulation of fluid |
|
|
|
than 50% of the time, with an intensity, which is partially |
8 |
Not specified |
|
|
disrupting the persons day to day life and which happens frequently |
9 |
Not applicable |
|
|
over the last 30 days. |
|
|
|
|
4 Complete impairment means that a problem that is present more |
|
|
|
|
than 95% of the time, with an intensity, which is totally disrupting |
|
|
|
|
the persons day to day life and which happens every day over the |
|
|
|
|
last 30 days. |
|
|
|
|
8 Not specified means there is insufficient information to specify |
|
|
|
|
the severity of the impairment. |
|
|
|
|
9 Not applicable means it is inappropriate to apply a particular |
|
|
|
|
code (e.g. b650 Menstruation functions for woman in |
|
|
|
|
or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Short List of Body Structures |
|
First Qualifier: |
Second Qualifier: |
|
|
Extent of impairment |
Nature of the change |
|
|
s1. STRUCTURE OF THE NERVOUS SYSTEM |
|
|
|
|
s110 Brain |
|
|
|
|
s120 Spinal cord and peripheral nerves |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
s2. THE EYE, EAR AND RELATED STRUCTURES |
|
|
|
|
|
|
|
|
|
s3. STRUCTURES INVOLVED IN VOICE AND SPEECH |
|
|
|
|
|
|
|
|
|
s4. STRUCTURE OF THE CARDIOVASCULAR, |
|
|
|
|
IMMUNOLOGICAL AND RESPIRATORY SYSTEMS |
|
|
|
|
s410 Cardiovascular system |
|
|
|
|
|
|
|
|
|
s430 Respiratory system |
|
|
|
|
|
|
|
|
|
s5. STRUCTURES RELATED TO THE DIGESTIVE, |
|
|
|
|
METABOLISM AND ENDOCRINE SYSTEMS |
|
|
|
|
|
|
|
|
ICF Checklist © World Health Organization, September 2003. |
Page 3 |
s6. STRUCTURE RELATED TO GENITOURINARY AND REPRODUCTIVE SYSTEM
s610 Urinary system
s630 Reproductive system
s7. STRUCTURE RELATED TO MOVEMENT
s710 Head and neck region
s720 Shoulder region
s730 Upper extremity (arm, hand)
s740 Pelvis
s750 Lower extremity (leg, foot)
s760 Trunk
s8. SKIN AND RELATED STRUCTURES
ANY OTHER BODY STRUCTURES
PART 2: ACTIVITY LIMITATIONS & PARTICIPATION RESTRICTION
•Activity is the execution of a task or action by an individual.. Participation is involvement in a life situation.
•Activity limitations are difficulties an individual may have in executing activities. Participation restrictions are problems an individual may have in involvement in life situations.
The Performance qualifier indicates the extent of Participation restriction by describing the persons actual performance of a task or action in his or her current environment. Because the current environment brings in the societal context, performance can also be understood as "involvement in a life situation" or "the lived experience" of people in the actual context in which they live. This context includes the environmental factors – all aspects of the physical, social and attitudinal world that can be coded using the Environmental. The Performance qualifier measures the difficulty the respondent experiences in doing things, assuming that they want to do them.
The Capacity qualifier indicates the extent of Activity limitation by describing the person ability to execute a task or an action. The Capacity qualifier focuses on limitations that are inherent or intrinsic features of the person themselves. These limitations should be direct manifestations of the respondent's health state, without the assistance. By assistance we mean the help of another person, or assistance provided by an adapted or specially designed tool or vehicle, or any form of environmental modification to a room, home, workplace etc.. The level of capacity should be judged relative to that normally expected of the person, or the person's capacity before they acquired their health condition.
Note: Use Appendix 2 if needed to elicit information on the Activities and Participation of the individual
First Qualifier: Performance
Extent of Participation Restriction
Second Qualifier: Capacity (without assistance) Extent of Activity limitation
0 No difficulty means the person has no problem
1 Mild difficulty means a problem that is present less than 25% of the time, with an intensity a person can tolerate and which happens rarely over the last 30 days.
2 Moderate difficulty means that a problem that is present less than 50% of the time, with an intensity, which is interfering in the persons day to day life and which happens occasionally over the last 30 days.
3 Severe difficulty means that a problem that is present more than 50% of the time, with an intensity, which is partially disrupting the persons day to day life and which happens frequently over the last 30 days.
4 Complete difficulty means that a problem that is present more than 95% of the time, with an intensity, which is totally disrupting the persons day to day life and which happens every day over the last 30 days.
8 Not specified means there is insufficient information to specify the severity of the difficulty.
9 Not applicable means it is inappropriate to apply a particular code (e.g. b650 Menstruation functions for woman in
Short List of A&P domains |
|
Performance |
Capacity Qualifier |
|
|
|
|
Qualifier |
|
|
|
|
||
d1. LEARNING AND APPLYING KNOWLEDGE |
|
|
||
d110 |
Watching |
|
|
|
d115 |
Listening |
|
|
|
d140 |
Learning to read |
|
|
|
|
|
|
|
|
d145 |
Learning to write |
|
|
|
d150 |
Learning to calculate (arithmetic) |
|
|
|
d175 Solving problems |
|
|
|
|
|
|
|
||
|
|
|
||
d2. GENERAL TASKS AND DEMANDS |
|
|
||
d210 |
Undertaking a single task |
|
|
|
|
|
|
|
|
d220 |
Undertaking multiple tasks |
|
|
|
|
|
|
|
|
d3. COMMUNICATION |
|
|
|
|
d310 |
Communicating with |
spoken messages |
|
|
d315 |
Communicating with |
|
|
|
d330 Speaking |
|
|
|
|
|
|
|
|
|
d335 Producing |
|
|
|
|
d350 |
Conversation |
|
|
|
|
|
|
|
|
d4. MOBILITY |
|
|
|
|
d430 |
Lifting and carrying objects |
|
|
|
|
|
|
|
|
d440 Fine hand use (picking up, grasping) |
|
|
|
|
d450 |
Walking |
|
|
|
d465 Moving around using equipment (wheelchair, skates, etc.) |
|
|
||
|
|
|
|
|
d470 |
Using transportation (car, bus, train, plane, etc.) |
|
|
|
d475 |
Driving (riding bicycle and motorbike, driving car, etc.) |
|
|
|
|
|
|
|
|
d5. SELF CARE |
|
|
|
|
d510 Washing oneself (bathing, drying, washing hands, etc) |
|
|
||
|
|
|
|
|
d520 |
Caring for body parts (brushing teeth, shaving, grooming, etc.) |
|
|
|
d530 |
Toileting |
|
|
|
d540 |
Dressing |
|
|
|
|
|
|
|
|
d550 |
Eating |
|
|
|
d560 |
Drinking |
|
|
|
|
|
|
|
|
d570 |
Looking after one`s health |
|
|
|
|
|
|
|
|
|
|
|
|
|
d6. DOMESTIC LIFE |
|
|
|
|
d620 |
Acquisition of goods and services (shopping, etc.) |
|
|
|
d630 Preparation of meals (cooking etc.) |
|
|
|
|
|
|
|
|
|
d640 |
Doing housework (cleaning house, washing dishes laundry, ironing, etc.) |
|
|
|
|
|
|
|
|
d660 |
Assisting others |
|
|
|
|
|
|
||
d7. INTERPERSONAL INTERACTIONS AND RELATIONSHIPS |
|
|
||
d710 |
Basic interpersonal interactions |
|
|
|
|
|
|
|
|
d720 |
Complex interpersonal interactions |
|
|
|
|
|
|
|
|
d730 |
Relating with strangers |
|
|
|
d740 Formal relationships |
|
|
|
|
d750 |
Informal social relationships |
|
|
|
|
|
|
|
|
d760 Family relationships |
|
|
|
|
d770 |
Intimate relationships |
|
|
|
|
|
|
|
|
d8. MAJOR LIFE AREAS |
|
|
|
|
ICF Checklist © World Health Organization, September 2003. |
Page 5 |
d810 Informal education
d820 School education
d830 Higher education
d850 Remunerative employment
d860 Basic economic transactions
d870 Economic
d9. COMMUNITY, SOCIAL AND CIVIC LIFE
d910 Community Life
d920 Recreation and leisure
d930 Religion and spirituality
d940 Human rights
d950 Political life and citizenship
ANY OTHER ACTIVITY AND PARTICIPATION
PART 3: ENVIRONMENTAL FACTORS
•Environmental factors make up the physical, social and attitudinal environment in which people live and conduct their lives.
Qualifier in environment: |
0 No barriers |
0 No facilitator |
||
Barriers or facilitator |
1 Mild barriers |
+1 Mild facilitator |
||
|
|
2 Moderate barriers |
+2 Moderate facilitator |
|
|
|
3 Severe barriers |
+3 Substantial facilitator |
|
|
|
4 Complete barriers |
+4 Complete facilitator |
|
|
|
|
|
|
Short List of Environment |
|
|
Qualifier |
|
|
|
barrier or facilitator |
||
e1. PRODUCTS AND TECHNOLOGY |
|
|
|
|
e110 |
For personal consumption (food, medicines) |
|
|
|
e115 |
For personal use in daily living |
|
|
|
e120 |
For personal indoor and outdoor mobility and transportation |
|
|
|
e125 Products for communication |
|
|
|
|
e150 |
Design, construction and building products and technology of buildings for public use |
|
||
e155 |
Design, construction and building products and technology of buildings for private use |
|
||
|
|
|||
e2. NATURAL ENVIRONMENT AND HUMAN MADE CHANGES TO |
|
|||
ENVIRONMENT |
|
|
|
|
e225 |
Climate |
|
|
|
e240 |
Light |
|
|
|
e250 |
Sound |
|
|
|
|
|
|
|
|
e3. SUPPORT AND RELATIONSHIPS |
|
|
|
|
e310 |
Immediate family |
|
|
|
e320 |
Friends |
|
|
|
e325 |
Acquaintances, peers, colleagues, neighbours and community members |
|
|
|
e330 People in position of authority |
|
|
|
|
e340 Personal care providers and personal assistants |
|
|
||
e355 |
Health professionals |
|
|
|
e360 |
Health related professionals |
|
|
|
|
|
|
|
|
e4. ATTITUDES |
|
|
|
|
e410 |
Individual attitudes of immediate family members |
|
|
|
e420 |
Individual attitudes of friends |
|
|
|
e440 |
Individual attitudes of personal care providers and personal assistants |
|
|
|
e450 |
Individual attitudes of health professionals |
|
|
|
e455 |
Individual attitudes of health related professionals |
|
|
|
e460 |
Societal attitudes |
|
|
|
e465 |
Social norms, practices and ideologies |
|
|
|
|
|
|
||
E5. SERVICES, SYSTEMS AND POLICIES |
|
|
||
e525 |
Housing services, systems and policies |
|
|
|
e535 |
Communication services, systems and policies |
|
|
|
e540 |
Transportation services, systems and policies |
|
|
|
e550 |
Legal services, systems and policies |
|
|
|
e570 |
Social security, services, systems and policies |
|
|
|
e575 |
General social support services, systems and policies |
|
|
|
e580 |
Health services, systems and policies |
|
|
|
e585 |
Education and training services, systems and policies |
|
|
|
e590 |
Labour and employment services, systems and policies |
|
|
|
|
|
|
||
ANY OTHER ENVIRONMENTAL FACTORS |
|
|
||
|
|
|
|
|
|
|
|
|
|
ICF Checklist © World Health Organization, September 2003. |
Page 7 |
Part 4: OTHER CONTEXTUAL INFORMATION
4.1 Give a thumbnail sketch of the individual and any other relevant information.
4.2Include any Personal Factors as they impact on functioning (e.g. lifestyle, habits, social background, education, life events, race/ethnicity, sexual orientation and assets of the individual).
Appendix 1:
BRIEF HEALTH INFORMATION
[ ] Self Report |
|
[ ] Clinician Administered |
|
|
||
X.1 |
Height : __/__/__ cm (or |
inches) |
|
|
|
|
X.2 |
Weight: __/__/__ kg |
(or |
pounds) |
|
|
|
X.3 |
Dominant Hand (prior to health condition): Left [ ] |
Right [ ] |
Both hands equally [ ] |
|||
X.4 |
How do you rate your physical health in the past month? |
|
|
|||
|
Very good [ ] |
Good [ ] |
Moderate [ ] |
Bad [ ] |
Very bad [ ] |
|
X.5 How do you rate your mental and emotional health in the past month?
Very good [ ] |
Good [ ] |
Moderate [ ] |
Bad [ ] |
Very bad [ ] |
X.6 Do you currently have any disease(s) or disorder(s) ?
[ |
] |
NO |
[ |
] YES |
|
|
If |
YES, please specify:_________________________________ |
|
|
|
|
|
_________________________________ |
X.7 Did you ever have any significant injuries that had an impact on your level of functioning? |
||||
[ |
] |
NO |
[ |
] YES |
|
|
If |
YES, please specify _________________________________ |
|
________________________________
X.8 Have you been hospitalized in the last year?
[ ] NO |
[ ] YES |
If YES, please specify reason(s) and for how long?
1._____________________________; ___. ___. ___ days
2._____________________________; ___. ___. ___ days
3._____________________________; ___. ___. ___ days
X.9 Are you taking any medication ( either prescribed or over the counter)?
[ ] NO |
[ ] YES |
If YES, please specify major medications
1._____________________________
2._____________________________
3._____________________________
ICF Checklist © World Health Organization, September 2003. |
Page 9 |
X.10 Do you smoke?
[ ] NO |
[ ] YES |
X.11 Do you consume alcohol or drugs?
[ ] NO |
[ ] YES |
If YES, please specify average daily quantity
Tobacco: |
__________________________ |
Alcohol: |
__________________________ |
Drugs: |
__________________________ |
X.12 Do you use any assistive device such as glasses, hearing aid, wheelchair, etc.?
[ ] NO |
[ ] YES |
If YES, please specify
_________________________________________
X.13 Do you have any person assisting you with your self care, shopping or other daily activities?
[ ] NO |
[ ] YES |
If YES, please specify person and assistance they provide
____________________________________________________
X.14 Are you receiving any kind of treatment for your health?
[ ] NO |
[ ] YES |
|
If YES, please specify: |
|
____________________________________________________ |
X.15 Additional significant information on your past and present health:
________________________________________________________________________
________________________________________________________________________
X.16 IN THE PAST MONTH, have you cut back (i.e. reduced) your usual activities or work because of your health condition? (a disease, injury, emotional reasons or alcohol or drug use)
[ ] NO |
[ ] YES |
If yes, how many days? _____ |
X.17 IN THE PAST MONTH, have you been totally unable to carry out your usual activities or work because of your health condition? (a disease, injury, emotional reasons or alcohol or drug use)
[ ] NO |
[ ] YES |
If yes, how many days? _____ |
Form Characteristics
| Fact Name | Description |
|---|---|
| Version | The ICF Checklist is currently at version 2.1a. |
| Purpose | This checklist serves as a practical tool for gathering and recording information on an individual's functioning and disability. |
| Usage | It is recommended to use the checklist alongside the ICF or ICF Pocket version. |
| Sources of Information | When completing the checklist, various information sources should be employed, including written records and direct observations. |
| Demographic Section | The checklist includes a demographic section for collecting optional data such as name, date of birth, and marital status. |
| Impairment Categories | Impairments are categorized into body functions and body structures, with specific qualifiers indicating the extent of impairment. |
| Assessment Scale | The checklist includes a scale from 0 (no impairment) to 4 (complete impairment) to evaluate the degree of impairment. |
| Regulatory Reference | This checklist is anchored in guidelines established by the World Health Organization. |
Guidelines on Utilizing Icf Checklist
The ICF Checklist Form is a systematic method for gathering information on an individual's functioning and disabilities. Accurate completion is essential for effective case documentation. Follow these straightforward steps to fill out the form correctly.
- Gather all necessary information regarding the individual. Sources may include written records, respondents, other informants, and direct observation.
- Enter the Date in the format Day/Month/Year.
- Fill in the Case ID and Participant No. as required.
- Complete the Demographic Information section with details such as name (optional), sex, date of birth, address (optional), years of formal education, current marital status, and current occupation. Check only one option under marital status and occupation that best fits the individual.
- In the Medical Diagnosis section, indicate if existing health conditions are present. Provide ICD codes if available. Mark if no medical condition exists.
- Proceed to Part 1a: Impairments of Body Functions. Identify the impairment level for each body function listed by selecting the appropriate qualifier (0-4, 8, or 9).
- Move on to Part 1b: Impairments of Body Structures. Similar to the previous part, identify the impairment level for body structures, selecting the correct qualifier.
- Ensure that all fields are filled out completely before submitting the form.
What You Should Know About This Form
1. What is the purpose of the ICF Checklist form?
The ICF Checklist form is designed to gather and log information about an individual's functioning and disability. It serves as a practical tool for clinicians and social workers to summarize findings in case records, aiding in better understanding and documentation of an individual's health condition.
2. How should the ICF Checklist be used?
The checklist should be used in conjunction with the ICF or ICF Pocket version. When completing it, all available information should be utilized. This includes written records, the primary respondent's insight, input from other informants, and direct observation of the individual. Additionally, filling out the Brief Health Information section is recommended if medical data is lacking.
3. What kind of information does the ICF Checklist capture?
The checklist captures demographic data, details about the individual’s medical conditions, and assessments of impairments in body functions and structures. It includes various qualifiers to measure the extent and nature of these impairments, ensuring a comprehensive overview of the individual’s health status.
4. What are the categories of impairments included in the form?
The ICF Checklist addresses impairments in body functions such as mental, sensory, voice, and speech functions, as well as cardiovascular, digestive, and musculoskeletal functions. Furthermore, it measures impairments in body structures ranging from the nervous system to the sensory organs. Each impairment is categorized with qualifiers that help assess severity.
5. How are impairments rated in the ICF Checklist?
Impairments are rated using a scale from 0 to 4. A rating of 0 indicates no impairment, while a rating of 4 signifies complete impairment impacting daily life significantly. The checklist also includes qualifiers for more detailed assessment, allowing for nuanced understanding of an individual’s condition.
6. Is it mandatory to fill out every section of the ICF Checklist?
While it is strongly encouraged to provide comprehensive information in the ICF Checklist, certain sections, such as name and address, are optional. Focus should be given to sections that aid in capturing the individual's health status accurately.
7. Who can assist in filling out the ICF Checklist?
Healthcare providers, social workers, and the individuals themselves can collaboratively fill out the ICF Checklist. Input from other informants, like family members or caregivers, is also valuable. The goal is to collect diverse perspectives to ensure accuracy and completeness.
8. Can the ICF Checklist be used in different settings?
Yes, the ICF Checklist is versatile and can be utilized across various settings, including clinical practice, rehabilitation centers, and social services. It is suitable for use with individuals of all ages and conditions, making it a valuable tool for a wide range of professionals.
9. What should I do if I encounter difficulties while completing the form?
If difficulties arise while completing the ICF Checklist, it is advisable to consult a supervisor or a healthcare professional familiar with the ICF framework. Guidance can also be sought from existing training materials or workshops focused on implementing the ICF methodology effectively.
Common mistakes
When filling out the ICF Checklist form, one common mistake is neglecting to gather all available information. The form instructs users to utilize written records, direct observations, and informant insights. Skipping this step can lead to incomplete or inaccurate assessments. Individuals often rely only on personal knowledge without cross-referencing other sources, which can skew the data.
Another frequent error is providing incomplete demographic information. Sections such as date of birth and sex are crucial for tracking and categorizing cases effectively. Omitting or incorrectly entering this information hampers the accuracy of the data collected. Ensuring that each field is carefully filled out helps maintain the integrity of the dataset and supports meaningful analysis.
Participants sometimes underestimate the importance of selecting the correct level of impairment in the relevant sections. Misclassifying the severity can lead to significant misunderstandings about the individual’s capabilities and needs. The extent of impairments should be evaluated thoroughly, taking into account the individual's day-to-day experiences within the past month. Careful consideration while selecting these ratings prevents misrepresentation and ensures appropriate care or interventions.
Lastly, many individuals overlook the necessity of including medical diagnosis information. If available, ICD codes should be entered to provide context regarding health conditions. This section is critical for creating a complete record of the individual's health status and understanding their specific challenges. Failing to document existing medical conditions, or inaccurately stating them, can lead to misdiagnosis or misuse of resources.
Documents used along the form
The ICF Checklist is a helpful tool in assessing an individual's functioning and disability. It is often used in conjunction with various other forms and documents to provide a comprehensive overview of a person's health status. Below is a list of documents that are commonly associated with the ICF Checklist.
- ICF Manual: This manual provides detailed guidelines on how to use the ICF Checklist effectively. It outlines the classification of health, functioning, and disability.
- Health History Form: This document collects an individual's medical history and health conditions. It helps provide context for the assessments made using the ICF Checklist.
- Assessment Report: This report summarizes findings from various assessments. It includes insights from the ICF Checklist and any other evaluations performed on the individual.
- Consent Form: A consent form is essential for obtaining permission from the individual or their guardian to collect and share information. It ensures transparency and adherence to privacy standards.
- Referral Form: This form is used to refer individuals to specialists or additional services. It typically includes relevant background information and reasons for the referral.
- Goal Setting Document: This document outlines short-term and long-term goals for the individual based on their assessment. It serves to direct interventions and track progress.
- Progress Notes: These notes are created during follow-up appointments to track the individual’s progress over time. They can include observations, changes in health status, and responses to treatment.
Utilizing these documents alongside the ICF Checklist can significantly enhance the understanding of a person's overall health. Together, they provide insights that can inform treatment and support strategies.
Similar forms
The ICF Checklist is an important tool that aligns closely with other documents utilized in health assessments and classifications. Here are four similar documents that share similarities in purpose or structure with the ICF Checklist:
- ICD-10 (International Classification of Diseases, 10th Revision): Like the ICF Checklist, the ICD-10 is a standardized tool for documenting health conditions. It classifies diseases and health-related issues, enabling healthcare providers to communicate effectively about a patient's diagnosis and treatment.
- DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition): The DSM-5 provides a framework for diagnosing mental health disorders. Similar to the ICF Checklist, it categorizes various mental health conditions to facilitate understanding and treatment planning.
- GAF Scale (Global Assessment of Functioning): The GAF Scale assesses an individual's overall functioning on a numeric scale. It serves a role akin to that of the ICF Checklist by evaluating the impact of disabilities on day-to-day functioning, aiding in treatment and support decisions.
- WHO Disability Assessment Schedule (WHODAS): This tool measures health and disability across various domains, paralleling the ICF Checklist’s comprehensive approach to assessing functioning. Both tools aim to provide a clearer picture of an individual's capabilities and needs, guiding interventions and resources.
Dos and Don'ts
When filling out the ICF Checklist form, there are certain practices to keep in mind for accuracy and efficiency. Below is a list of 10 things to do and not to do while completing the form.
- Do: Use all available information before finishing the form.
- Do: Include details from written records, interviews, and direct observations.
- Do: Ensure the demographic information is filled out completely.
- Do: Specify the medical diagnosis when possible, including ICD codes.
- Do: Mark the appropriate options for each section clearly.
- Do: If necessary, complete the Brief Health Information appendix for additional details.
- Do: Be honest and accurate when describing impairments and health conditions.
- Do: Review the form for any errors before submission.
- Do: Consult with other relevant informants if needed for clarity.
- Do: Maintain confidentiality when handling personal information.
- Don't: Skip any sections that apply to the individual being assessed.
- Don't: Use jargon or technical terms that may confuse respondents.
- Don't: Fill out the form without proper context or understanding of the individual's situation.
- Don't: Assume information without verifying facts from multiple sources.
- Don't: Leave spaces blank when a response is applicable.
- Don't: Rush through the checklist; careful assessment leads to better results.
- Don't: Share any personal information without consent.
- Don't: Forget to date and identify the case correctly at the top of the form.
- Don't: Misinterpret the definitions of impairments or body functions.
- Don't: Neglect to provide extra comments for additional explanations if necessary.
Misconceptions
Misconceptions about the ICF Checklist form can lead to confusion and misinterpretation of its purpose and use. Below are five common misconceptions:
- The ICF Checklist is only for clinicians. Some believe that only healthcare professionals can use this tool. In reality, the checklist is designed for various practitioners, including social workers and rehabilitation specialists, allowing anyone involved in assessing functioning and disability to utilize it.
- Completing the checklist requires extensive medical knowledge. It is a common thought that only someone with a medical background can fill out the ICF Checklist. However, the checklist can be completed using various sources of information such as observations and reports from individuals or family members, not just medical records.
- The ICF Checklist focuses solely on medical diagnoses. Many people mistakenly think that the checklist is only about identifying medical conditions. In truth, it assesses functioning and disability based on a broad range of factors, including abilities and personal circumstances, which can provide a holistic view of an individual’s situation.
- The ICF Checklist is used only for formal assessments. Some assume this tool is reserved for strict clinical assessments. However, it can also be beneficial in informal settings, such as discussions with clients about their functioning and needs, making it versatile in various contexts.
- All information on the ICF Checklist is mandatory. There is a misconception that every field on the checklist must be filled out for it to be valid. While comprehensive information is beneficial, certain sections, such as name and address, are optional, allowing for flexibility based on individual circumstances.
Key takeaways
Filling out the ICF Checklist form is essential for accurately documenting an individual's functioning and disability. Here are key takeaways for effective use of the form:
- The ICF Checklist is designed to record important information related to functioning and disability based on the International Classification of Functioning, Disability and Health.
- Gather comprehensive information before completion. Use written records, primary respondents, other informants, and direct observations to ensure accuracy.
- In absence of medical and diagnostic data, complete the appendix on Brief Health Information as a supplementary step.
- Ensure demographic information is as complete as possible, including the participant's name, sex, date of birth, marital status, and occupation.
- For documenting health conditions, provide specific ICD codes whenever possible, enhancing the clarity of the participant's diagnosis.
- Utilize impairment qualifiers, ranging from "no impairment" to "complete impairment," to indicate the severity of challenges faced by the participant in their daily life.
- Consider both body functions and body structures when assessing impairments, paying attention to both physiological aspects and anatomical parts.
- Use the ICF Checklist alongside the ICF Pocket version for a more holistic understanding of the participant's condition and situation.
Browse Other Templates
Argosy University Online - Requestors should check their attendance years for proper record-keeping.
Equivalent Training (ET) - Form to excuse absence from regular scheduled training.
Payment Rejected by Bank - The stop payment process is established to safeguard financial transactions.