Fill Out Your Ihss Referral Form
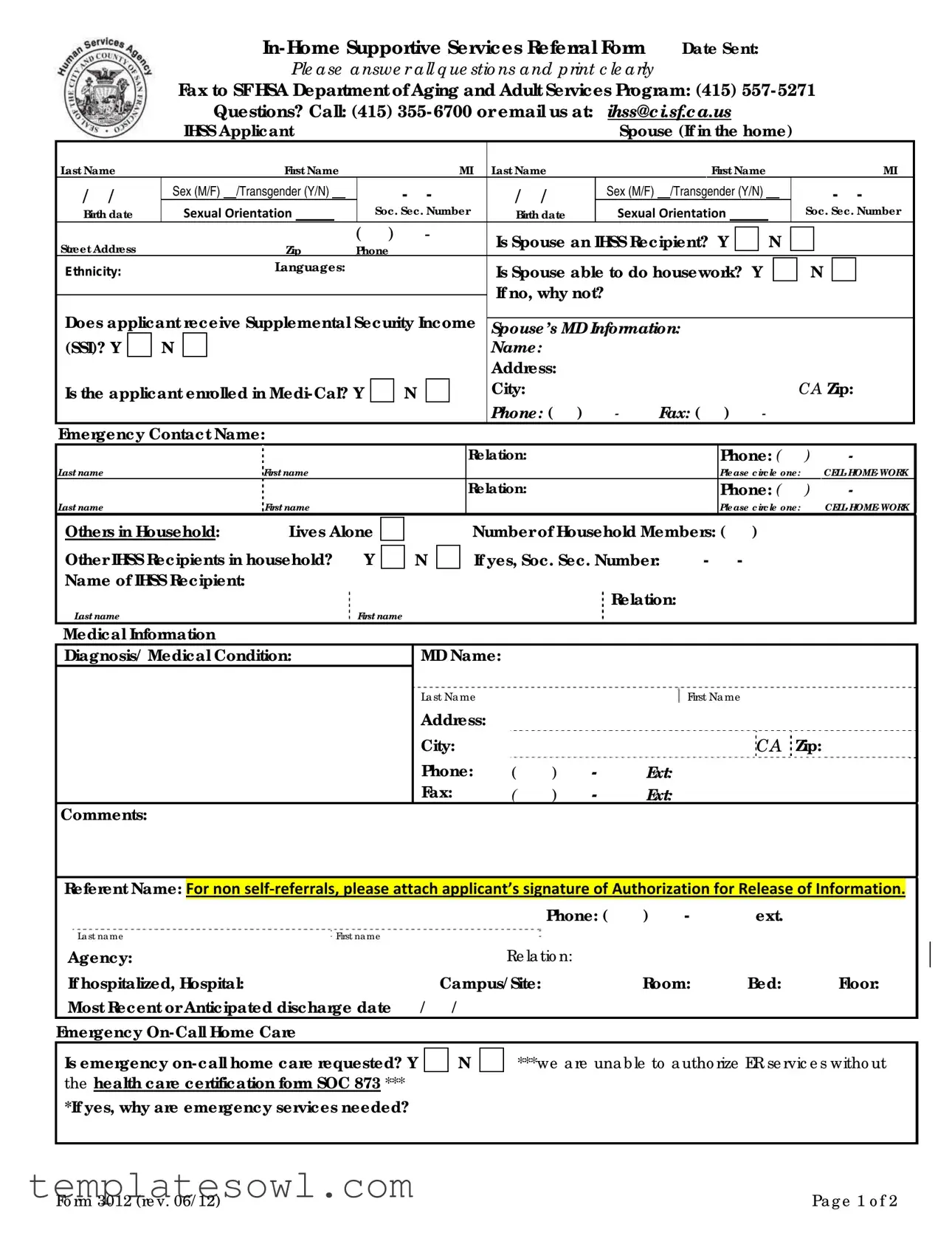
The IHSS Referral Form is an essential tool designed to facilitate access to In-Home Supportive Services for those in need of assistance. Completion of this form is the first step in the process, and it addresses various critical areas that help assess an applicant's eligibility and requirements for support. Basic personal information is requested, including names, birth dates, and contact details of the applicant and their spouse, if applicable. It inquires about eligibility for supplemental security income and Medi-Cal enrollment, as well as details regarding household members and any existing IHSS recipients. The form also explores medical conditions and functional abilities, asking about specific needs like mobility, bathing, and household tasks. Emergency on-call home care requests can be made here, although it is essential to note that additional certification may be required. Finally, the IHSS Referral Form prompts applicants to describe how their needs are currently being met and provides options for additional services, ensuring a comprehensive approach to patient care. Properly filling out this form can significantly impact the level of support that may follow, so it requires careful attention and accuracy.
Ihss Referral Example
|
|
|
|
|
|
|
|
|
Date Sent: |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
Ple ase answe r all q ue stio ns and print c le arly |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
Fax to SF HSA Department of Aging and Adult Services Program: (415) |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
Questions? Call: (415) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
IHSS Applicant |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Spouse (If in the home) |
|
|
|
|
|
|
|
||||||||||||||||||||||
Last Name |
|
|
|
|
|
First Name |
|
|
|
|
|
|
|
|
|
|
|
MI |
Last Name |
|
|
|
|
|
|
First Name |
|
|
|
|
|
MI |
|
||||||||||||||||||
/ / |
|
|
Sex (M/F) |
|
/Transgender (Y/N) |
|
|
|
- |
- |
|
|
|
|
/ |
/ |
|
|
Sex (M/F) |
/Transgender (Y/N) |
|
|
- |
- |
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
Birth date |
|
Sexual Orientation |
|
|
|
Soc. Sec. Number |
Birth date |
|
|
Sexual Orientation |
|
|
|
|
|
|
|
|
|
Soc. Sec. Number |
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
|
|
|
Zip |
( |
|
) |
|
|
- |
|
|
|
|
Is Spouse an IHSS Recipient? |
|
Y |
|
|
|
N |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
Ethnicity: |
|
|
|
|
|
Languages: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Is Spouse able to do housework? Y |
|
|
|
|
|
N |
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If no, why not? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Does applicant receive Supplemental Security Income |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
Spouse’s MD Information: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
(SSI)? Y |
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Is the applicant enrolled in |
|
|
|
|
N |
|
|
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CA Zip: |
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone: ( |
) |
|
- |
|
Fax: ( |
) |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Emergency Contact Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Relation: |
|
|
|
|
|
|
|
|
Phone: ( |
) |
|
|
|
- |
|
|
|||||||||||
Last name |
|
|
|
|
|
First name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please circle one: |
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Relation: |
|
|
|
|
|
|
|
|
Phone: ( |
) |
|
|
|
- |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
Last name |
|
|
|
|
|
First name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please circle one: |
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
Others in Household: |
|
|
Lives Alone |
|
|
|
|
|
|
|
|
|
Number of Household Members: ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
Other IHSS Recipients in household? |
|
Y |
|
|
|
|
N |
|
|
If yes, Soc. Sec. Number: |
- |
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
Name of IHSS Recipient: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Relation: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Last name |
|
|
|
|
|
|
|
|
|
|
First name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Medical Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Diagnosis/ Medical Condition: |
|
|
|
|
|
|
|
MD Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
La st Na me |
|
|
|
|
|
|
|
First Na me |
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
CA Zip: |
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone: |
( |
) |
- |
|
Ext: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fax: |
|
|
( |
) |
- |
|
Ext: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Comments: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Referent Name: For non self‐referrals, please attach applicant’s signature of Authorization for Release of Information.
|
|
|
Phone: ( |
) |
- |
ext. |
|
Last name |
First name |
|
|
|
|
|
|
Agency: |
|
|
Re la tio n: |
|
|
|
|
If hospitalized, Hospital: |
|
Campus/ Site: |
Room: |
Bed: |
Floor: |
||
Most Recent or Anticipated discharge date / |
/ |
|
|
|
|
|
|
Emergency |
|
|
|
|
|
|
|
Is emergency |
N |
***we a re una ble to a utho rize ER se rvic e s witho ut |
|||||
the health care certification form SOC 873 *** |
|
|
|
|
|
|
|
*If yes, why are emergency services needed? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fo rm 3012 (re v. 06/ 12) |
|
|
|
|
|
|
Pa g e 1 o f 2 |
The information on this page will help us assess your needs and respond to your request for services. If the form is
not completed in full, your application will not be accepted.
*We a re unab le to autho rize e me rg e nc y o
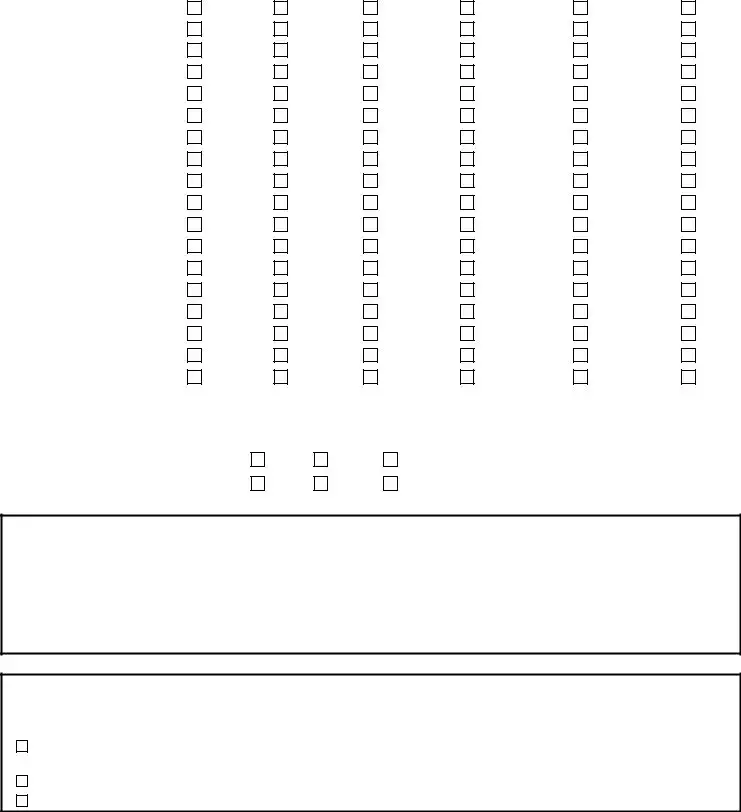
Functional Ability
|
Unknown |
Independent |
|
Verbal |
|
Some human |
Lots of human |
Dependent |
||||
|
|
|
|
|
|
Assist |
|
|
help |
help |
|
|
Transfer mobility |
|
|
|
|
|
|
|
|
|
|
|
|
Bathing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dressing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Toileting |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Eating |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Grooming |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ambulating (walking) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mobility indoors |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Stair climbing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Managing medicines |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Shopping |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Meal prep & clean up |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Transportation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Managing money |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Light housework |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Heavy housework |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Laundry |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Risks |
|
|
|
|
|
|
|
|
|
|
||
Does the client currently exhibit |
|
Active |
Past |
|
Unknown |
|
|
Explain |
|
|||
or have history of… |
|
|
History |
|
|
|
|
|
|
|
||
Violent Behavior |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Financial management/ Eviction |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Support System |
|
|
|
|
|
|
|
|
|
|
||
How are your service needs currently being met? Please be as specific as possible and include information about current caregiver(s) and areas of need.
How will you be able to meet your service needs until IHSS eligibility and services are established?
Services
Please list any services you currently receive:
Are you interested in learning more about the following services?
On Lok Lifeways/ PACE program (a comprehensive
Adult Day Health Care thro ug h
Other services:
***Please note that in order to receive IHSS you must be on
Fo rm 3012 (re v. 06/ 12) |
Pa g e 2 o f 2 |
Form Characteristics
| Fact Name | Description |
|---|---|
| Date Sent | The form must include the date when it is sent to the relevant department. |
| Contact Information | If you have questions about the form, you can call (415) 355-6700 or email ihss@ci.sf.ca.us. |
| Spouse Information | The form requires details about the applicant's spouse, including their health status and Social Security number. |
| Emergency Contact | Applicants must provide an emergency contact name, relation, and phone number for quicker assistance. |
| Functional Ability Assessment | The form assesses the applicant's functional abilities such as mobility, grooming, and medication management. |
| Emergency Home Care | Applicants must indicate whether emergency on-call home care is requested, with reasons for the request. |
| Governing Law | This referral form operates under California's In-Home Supportive Services Program regulations. |
Guidelines on Utilizing Ihss Referral
After completing the In-Home Supportive Services (IHSS) Referral Form, the next step involves submitting it to the appropriate department. This submission allows the relevant authorities to assess the information provided and respond accordingly. Ensure that every section of the form is filled out correctly, as incomplete forms may cause delays in processing your application.
- Fill in the Date Sent at the top of the form.
- Complete the applicant's information, including their last name, first name, middle initial, sex, birth date, sexual orientation, and social security number.
- Provide the spouse's information, if applicable, by entering their last name, first name, middle initial, sex, birth date, sexual orientation, and social security number.
- Input the street address, city, state, and zip code for the applicant and spouse.
- Include the phone number for the applicant and indicate if the spouse is an IHSS recipient.
- Answer whether the spouse can perform housework and provide reasons if they cannot.
- State if the applicant receives Supplemental Security Income (SSI) and if they are enrolled in Medi-Cal.
- Fill out the emergency contact information including name, relation, and phone number.
- Indicate the number of household members and whether there are any other IHSS recipients in the household.
- Provide medical information including diagnosis and the name of the medical doctor, along with their contact details.
- Complete the referral information, including the name of the referent and their agency or relation to the applicant.
- Answer questions regarding emergency on-call home care and provide details if services are needed.
- Describe the applicant’s functional ability and any risks related to their behavior or financial management.
- Detail how current service needs are being met and specify any services currently received.
- Express interest in additional services, if applicable, including On Lok Lifeways/ PACE program and Adult Day Health Care.
After completing these steps, ensure the form is signed and submit it via fax to the San Francisco Human Services Agency Department of Aging and Adult Services at the designated fax number. Reach out for assistance if needed.
What You Should Know About This Form
What is the IHSS Referral Form used for?
The IHSS Referral Form is a document designed for individuals seeking In-Home Supportive Services. It helps assess the unique needs of the applicant, along with any relevant information about their caregiver or home situation. Completing the form correctly is crucial for determining eligibility for the program and ensuring that the necessary support can be provided.
How do I submit the IHSS Referral Form?
To submit the form, please ensure all sections are filled out clearly. Once completed, fax it to the San Francisco Human Services Agency's Department of Aging and Adult Services at (415) 557-5271. If you have any questions during the process, you can also reach out via phone at (415) 355-6700 or email at ihss@ci.sf.ca.us.
What information do I need to provide about the applicant?
You will need to provide various details about the applicant, such as their full name, birth date, sex, Social Security number, and contact information. Additionally, you should disclose any relevant medical conditions, current service needs, and whether the applicant receives Supplemental Security Income or is enrolled in Medi-Cal.
Is my spouse’s information required on the form?
If the applicant lives with a spouse, the form requires the spouse's details. This includes their name, birth date, Social Security number, and whether they are also an IHSS recipient. The inclusion of this information helps provide a more comprehensive understanding of the household's needs.
What happens if the form is not fully completed?
Completing the IHSS Referral Form in its entirety is essential. If any questions are left unanswered, the application may be deemed incomplete and could be rejected. It's important to provide as much accurate information as possible to avoid delays in processing.
Can I request emergency on-call home care through this form?
Yes, you can request emergency on-call home care when filling out the form. However, it is important to provide a reason for the request. Please note that emergency services cannot be authorized without the health care certification form SOC 873. This requirement exists to ensure appropriate and timely care based on individual circumstances.
What if I need assistance with Medi-Cal coverage?
The form mentions that individuals applying for IHSS must be on full-scope Medi-Cal. If you do not currently have coverage or are unsure about your eligibility, staff can assist you with the application process for Medi-Cal. Seeking this help early can streamline your access to necessary services.
How will I know if my application for IHSS has been accepted?
Common mistakes
Filling out the In-Home Supportive Services (IHSS) Referral Form is an important step for individuals seeking assistance. However, there are common mistakes that can hinder the application process. One significant error is failing to complete the entire form. Each section has specific questions that help assess needs and determine eligibility. Leaving questions unanswered may result in delays or even rejection of the application.
Another frequent mistake involves incorrect personal information. Applicants sometimes miswrite their names, addresses, or Social Security numbers. The accuracy of this information is crucial as it ensures proper identification and prevents future complications. Even minor errors can lead to misunderstandings or delays in processing the application, so it is essential to double-check all entries.
Some applicants overlook the importance of detailing medical conditions. The section asking about diagnosis or medical conditions requires careful attention. Providing vague or incomplete descriptions can weaken the case for needing assistance. Thoroughly describing the medical situation helps the reviewing agency understand the applicant's specific needs and may increase the chances of approval.
A lack of communication regarding additional household members is another mistake. When filling out the form, applicants must specify the number of household members and whether there are any other IHSS recipients living at the same address. This information can influence eligibility and available services. If not properly reported, it may lead to complications or misassessment of the applicant's needs.
Lastly, applicants sometimes neglect to provide contact information for their doctors or emergency contacts. This information is vital for follow-up during the assessment process. By ensuring that all necessary contacts are included, applicants can facilitate communication and expedite the eligibility determination process. Remembering these five key points can greatly assist individuals in completing the IHSS Referral Form correctly and efficiently.
Documents used along the form
When applying for In-Home Supportive Services (IHSS), several other forms accompany the IHSS Referral form to provide a comprehensive view of the applicant's needs and circumstances. Understanding these documents can facilitate a smoother application process. Here are some of the key forms often used in conjunction with the IHSS Referral form:
- IHSS Authorization for Release of Information: This form must be signed by the applicant to permit the sharing of personal information needed for evaluating their eligibility for services.
- Medi-Cal Application: Since eligibility for IHSS is linked to Medi-Cal, this application assesses whether the applicant meets the income and asset criteria for this healthcare program.
- Health Care Certification Form (SOC 873): This document provides verification of the applicant's medical condition and need for assistance, crucial for approving emergency on-call home care services.
- Functional Assessment Form: This form evaluates the applicant's daily living skills and levels of independence, helping to determine the type and amount of services required.
- Emergency Contact Information: Collecting details about emergency contacts ensures that family members or friends can be reached if urgent situations arise concerning the applicant's care.
- Caregiver Information Form: If the applicant currently has a caregiver, this form gathers information about them, including their qualifications and the type of care they provide.
- Medical History Form: This form captures relevant medical history and current conditions, which assists in assessing the applicant's overall health and care needs.
- Household Member Questionnaire: This document provides valuable insight into the living situation, including other individuals in the household who may impact the applicant’s care needs.
- Service Preferences Form: This optional form allows the applicant to express preferences for particular types of services or providers they feel comfortable with.
Completing all these forms can feel overwhelming, but each one plays a crucial role in ensuring that applicants receive the appropriate support tailored to their unique situations. Taking the time to understand and properly fill out each document will facilitate a smoother process in obtaining the necessary in-home support services.
Similar forms
- Medicaid Application Form: This document collects personal information and financial details to determine eligibility for Medicaid, similar to how the IHSS Referral Form assesses an individual’s qualifications for in-home supportive services.
- Social Security Disability Insurance (SSDI) Application: Both forms require information about the applicant’s medical history, diagnosis, and personal details, aiming to establish a need for government assistance.
- Supplemental Security Income (SSI) Application: Each form asks for demographic data and details regarding income, disability, and living situation, establishing criteria for support from governmental programs.
- Personal Care Attendant (PCA) Evaluation Form: This document evaluates an individual's care needs, similarly to the IHSS Referral Form, focusing on functional abilities and specific assistance requirements.
- Long-Term Care Referral Form: This form requests information about the applicant’s health status and social situation, paralleling the questions in the IHSS Referral Form to assess long-term care needs.
Dos and Don'ts
When filling out the IHSS Referral Form, there are important dos and don'ts to keep in mind to ensure your application is processed smoothly.
- Do fill out all sections completely. Incomplete forms may result in rejection.
- Do print your answers clearly. This helps avoid misunderstandings.
- Do include all necessary phone numbers and contact information for all parties involved.
- Do check for accuracy. Ensure that names, dates, and Social Security numbers are correct.
- Do provide details about any medical conditions or diagnoses. This information is crucial for assessing service needs.
- Don't leave any required fields blank. This can delay your application significantly.
- Don't provide incomplete or vague information about your service needs.
- Don't forget to sign the form if you are not completing it as the applicant.
- Don't assume that additional documents are not necessary. Always inquire if more information is needed.
- Don't hesitate to reach out for help if you're unsure how to complete a section. Support is available.
Misconceptions
Misconceptions about the IHSS Referral Form can lead to confusion. Here are some common misunderstandings:
- It’s optional to complete all sections. Many people think they can skip questions, but the form must be filled out completely to be accepted.
- Emergency services are automatically authorized. Some believe that if they request emergency on-call home care, it will be granted. However, authorization requires a specific health care certification.
- Anyone can fill out the form. While family and friends can assist, the applicant must sign the form if they are not self-referring.
- Providing personal information is unnecessary. Some individuals hesitate to share personal details, but this information is essential to assess eligibility for services.
- You must be a homeowner to qualify. Many think homeownership is a requirement, but it's not a factor in eligibility for IHSS services.
- Receiving other services disqualifies you. Some assume that being on other support programs like SSI means they can't apply for IHSS. This is not true, and multiple services can be accessed concurrently.
- Only seniors can apply. A common myth is that only elderly individuals are eligible for IHSS, but people of all ages with qualifying needs may qualify.
- Your referral will be processed quickly without follow-up. It is a misconception that the process is automatic. Following up can help clarify any issues or expedite your application.
Key takeaways
Understanding the In-Home Supportive Services (IHSS) Referral Form is crucial for applicants and their families. Here are seven key takeaways to simplify the process:
- Complete All Sections: Fill out every part of the form clearly. Incomplete forms may be rejected, delaying your application.
- Emergency Services Certification: If you need emergency on-call home care, ensure you provide the necessary health care certification form (SOC 873) for approval.
- Information Accuracy: Review your answers for accuracy, particularly names, contact details, and Social Security numbers. Mistakes can lead to application issues.
- Medical Information: Provide detailed medical information, including diagnoses and the appropriate physician’s contact details. This helps address your specific needs.
- Service Needs: Clearly describe how your service needs are currently being met and what additional support you require. This information aids in proper assessment.
- Eligibility Requirements: Remember that to qualify for IHSS, you must be enrolled in full-scope Medi-Cal, even if you have a potential share of costs.
- Contact for Assistance: If you have questions, reach out to the IHSS support team via phone or email. They can provide guidance and clarification.
Filling out the IHSS Referral Form accurately and thoroughly will help ensure a smoother process in obtaining necessary services.
Browse Other Templates
Ibc Customer Service Phone - The bank uses this form to assess potential candidates.
Florida Medicaid Provider Agreement 2023 - Complying fully with state and federal laws is a key aspect of this provider agreement, highlighting the legal obligations involved.
Net 30 Payment Terms - The credit application includes sections for both purchasing and billing contact details.