Fill Out Your Individual Service Plan Wisconsin Form
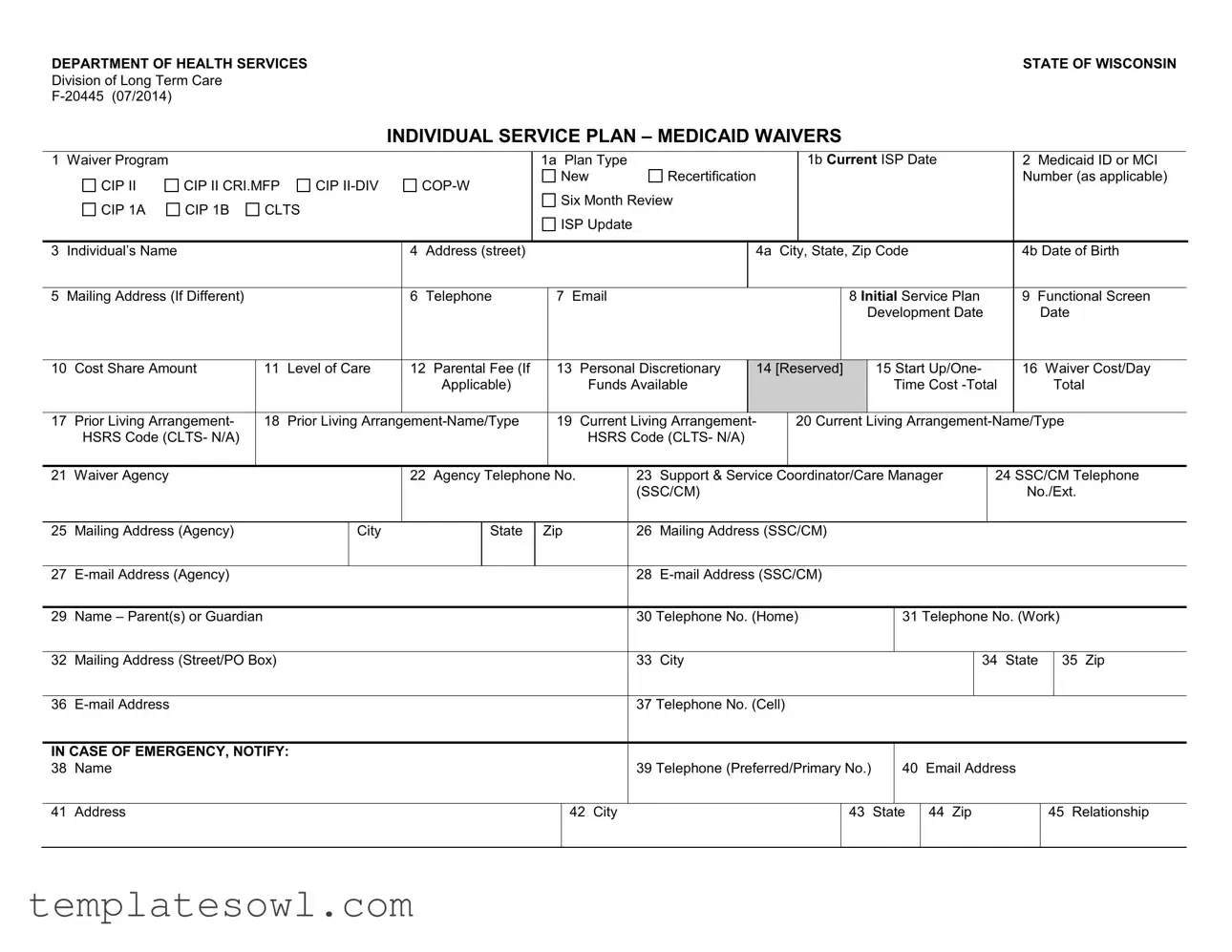
The Individual Service Plan (ISP) in Wisconsin serves as an essential framework designed to outline the tailored services and support that individuals receiving Medicaid Waivers can access. This comprehensive form captures vital information, including the individual's name, address, Medicaid ID, and contact details, ensuring easy identification and communication between all parties involved. It emphasizes informed choices by detailing the individual’s rights to choose their service providers and care settings, whether in a nursing home or the community. Key sections of the form address the specific waiver programs available, the service codes, and the outcomes anticipated from each service. The ISP also considers personal preferences through parental fees, cost-sharing amounts, and service frequency, maintaining a person-centered approach. Additionally, the document includes a verification section for six-month reviews, ensuring that the services remain aligned with the individual's evolving needs. Acknowledging the importance of oversight, the plan requires signatures from various stakeholders, including the participant, care manager, and guardians, thus validating collaborative engagement in the development and ongoing assessment of the individual's support system.
Individual Service Plan Wisconsin Example

DEPARTMENT OF HEALTH SERVICESSTATE OF WISCONSIN
Division of Long Term Care
INDIVIDUAL SERVICE PLAN – MEDICAID WAIVERS
1 Waiver Program |
|
|
|
|
|
|
|
|
1a Plan Type |
|
|
|
|
|
1b Current ISP Date |
|
|
|
|
2 Medicaid ID or MCI |
|
||||||||||||
|
CIP II |
CIP II CRI.MFP |
CIP |
|
|
New |
|
Recertification |
|
|
|
|
|
|
|
|
|
|
|
|
Number (as applicable) |
|
|||||||||||
|
|
|
Six Month Review |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
CIP 1A |
CIP 1B |
CLTS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
ISP Update |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
Individual’s Name |
|
|
|
|
|
4 |
Address (street) |
|
|
|
|
|
|
|
4a |
City, State, Zip Code |
|
|
|
|
|
4b Date of Birth |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
5 |
Mailing Address (If Different) |
|
|
|
6 |
Telephone |
|
7 |
|
|
|
|
|
|
8 Initial Service Plan |
|
9 Functional Screen |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Development Date |
|
|
Date |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
10 |
Cost Share Amount |
|
11 |
Level of Care |
12 Parental Fee (If |
|
13 |
Personal Discretionary |
14 [Reserved] |
|
15 Start Up/One- |
|
16 Waiver Cost/Day |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
Applicable) |
|
|
|
Funds Available |
|
|
|
|
|
|
|
Time Cost |
|
|
|
Total |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
17 |
Prior Living Arrangement- |
|
18 |
Prior Living |
|
19 |
Current Living Arrangement- |
|
20 Current Living |
|
|||||||||||||||||||||||
|
HSRS Code (CLTS- N/A) |
|
|
|
|
|
|
|
|
|
|
HSRS Code (CLTS- N/A) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
21 |
Waiver Agency |
|
|
|
|
|
22 Agency Telephone |
No. |
|
23 |
Support & Service |
Coordinator/Care Manager |
|
|
24 SSC/CM Telephone |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(SSC/CM) |
|
|
|
|
|
|
|
|
|
|
|
|
|
No./Ext. |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
25 |
Mailing Address (Agency) |
|
|
City |
|
|
State |
Zip |
|
|
26 |
Mailing Address (SSC/CM) |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
27 |
|
|
|
|
|
|
|
|
|
|
|
28 |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
29 |
Name – Parent(s) or Guardian |
|
|
|
|
|
|
|
|
|
|
|
30 |
Telephone No. (Home) |
|
31 Telephone No. (Work) |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
32 |
Mailing Address (Street/PO Box) |
|
|
|
|
|
|
|
|
|
|
33 |
City |
|
|
|
|
|
|
|
|
|
|
34 |
State |
35 Zip |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
36 |
|
|
|
|
|
|
|
|
|
|
|
|
|
37 |
Telephone No. (Cell) |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
IN CASE OF EMERGENCY, NOTIFY: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
38 |
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
39 |
Telephone (Preferred/Primary No.) |
|
40 |
Email Address |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
41 |
Address |
|
|
|
|
|
|
|
|
|
|
42 City |
|
|
|
|
|
43 |
|
State |
44 |
Zip |
|
|
45 Relationship |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
62 Service Code #
63 Service Name
64 |
65 |
Outcome No. |
Service Provider Name Address and |
Telephone No. |
|
|
(Email, cell phone no., if known) |
65a
Start Date
65b
End Date
66
Unit Cost ($/hr; day)
67
Authorized Units of Service and Frequency
(#/day or week or month)
68 |
69 |
Daily Cost (total |
Funding |
yearly ÷ 365 days) |
Source |
|
|

70 PARTICIPANT INFORMED – R IGHTS AND CHOICE (Review REQUIRED at initial plan development and recertification.)

 I have been informed that I have a RIGHT TO CHOOSE between a nursing home or
I have been informed that I have a RIGHT TO CHOOSE between a nursing home or

 I have been informed of my CHOICES in the waiver programs, including my right to CHOOSE the TYPE OF SERVICES I receive under my service plan.
I have been informed of my CHOICES in the waiver programs, including my right to CHOOSE the TYPE OF SERVICES I receive under my service plan.

 I understand that I have CHOICES in the waiver programs, including my right to CHOOSE from available, qualified providers that will provide the services outlined in my plan.
I understand that I have CHOICES in the waiver programs, including my right to CHOOSE from available, qualified providers that will provide the services outlined in my plan.

 I have been informed verbally and in writing of my rights and responsibilities in the Medicaid Waiver Programs and I understand these rights and responsibilities.
I have been informed verbally and in writing of my rights and responsibilities in the Medicaid Waiver Programs and I understand these rights and responsibilities.

 I have been informed verbally and in writing of my RIGHT TO REQUEST A HEARING should I disagree with decisions made about my ELIGIBILITY to participate in the HCBS program.
I have been informed verbally and in writing of my RIGHT TO REQUEST A HEARING should I disagree with decisions made about my ELIGIBILITY to participate in the HCBS program.

 I have been informed verbally and in writing of my RIGHT TO REQUEST A HEARING should I disagree with decisions made that would DENY, REDUCE OR TERMINATE the services I receive.
I have been informed verbally and in writing of my RIGHT TO REQUEST A HEARING should I disagree with decisions made that would DENY, REDUCE OR TERMINATE the services I receive.

 By my signature below I indicate I have chosen to accept community services through a Medicaid Home and Community Waiver Program.
By my signature below I indicate I have chosen to accept community services through a Medicaid Home and Community Waiver Program.
71 UPDATE/REVIEW VERIIFICATION - APPLIES TO PLAN REVIEW OR ISP UPDATE ONLY

 The SIX MONTH ISP Review was completed with the participant/guardian on the date below and there are no changes to the ISP at this time.
The SIX MONTH ISP Review was completed with the participant/guardian on the date below and there are no changes to the ISP at this time.

 The SIX MONTH ISP Review was completed with the participant/guardian on the date below and agreed upon changes to the ISP are included herein.
The SIX MONTH ISP Review was completed with the participant/guardian on the date below and agreed upon changes to the ISP are included herein.

 The ISP was UPDATED on the date below to reflect changes (additions, increases or reductions) to planned services or providers or to units/frequency of service.
The ISP was UPDATED on the date below to reflect changes (additions, increases or reductions) to planned services or providers or to units/frequency of service.
SIGNATURES: ISP Signature Requirements apply at the time of plan development, review and recertification.
SIGNATURE - Participant |
Date Signed |
SIGNATURE – Support and Service Coordinator/Care Manager |
Date Signed |
|
|
|
|
SIGNATURE – Guardian/Authorized Representative/Parent |
Date Signed |
SIGNATURE - Guardian/Authorized Representative/Parent |
Date Signed |
|
|
|
|
SIGNATURE - Witness |
Date Signed |
SIGNATURE – Witness |
Date Signed |
|
|
|
|
DISTRIBUTION: Original – DHS; Copy - County Care Manager/Support and Service Coordinator; Copy – Individual; Copy - Authorized Representative

CIP

 A variance to the
A variance to the

 A variance to allow waiver funding for an individual that is elderly to reside in a CBRF connected to a nursing home
A variance to allow waiver funding for an individual that is elderly to reside in a CBRF connected to a nursing home
BY SIGNING BELOW, THE SUPPORT AND SERVICE COORDINATOR / CARE MANAGER ATTESTS TO THE FOLLOWING:
1.The environment is
2.The facility is the preferred residence of the applicant/participant or his/her legal representative.
SIGNATURE - Participant |
Date Signed |
SIGNATURE – Support and Service Coordinator/Care Manager |
Date Signed |
|
|
|
|
SIGNATURE – Guardian/Authorized Representative/Parent |
Date Signed |
SIGNATURE - Guardian/Authorized Representative/Parent |
Date Signed |
|
|
|
|
SIGNATURE - Witness |
Date Signed |
SIGNATURE – Witness |
Date Signed |
|
|
|
|
DISTRIBUTION: Original – DHS; Copy - County Care Manager/Support and Service Coordinator; Copy – Individual; Copy - Legal Representative
Form Characteristics
| Fact Name | Description |
|---|---|
| Governing Law | The Individual Service Plan is governed by Wisconsin's Medicaid Waiver programs and applicable state and federal laws. |
| Form Version | This form is F-20445, with a version date of July 2014. |
| Purpose | The Individual Service Plan outlines personalized services for participants of Medicaid waiver programs. |
| Personal Information | Includes fields for the individual's name, address, and contact details, ensuring accurate identification and communication. |
| Service Provider Details | Providers must be listed with contact information, facilitating easy access for service-related inquiries. |
| Rights & Choices | The document emphasizes the participant's rights to choose between facilities and services as part of their care. |
| Signature Requirements | Signatures from the participant, service coordinator, and a witness are required at several points, ensuring accountability and consent. |
Guidelines on Utilizing Individual Service Plan Wisconsin
Filling out the Individual Service Plan form is an important step in ensuring that you receive the appropriate services and support. This document outlines your needs and preferences as you prepare to engage with the available Medicaid waiver programs. The process is straightforward. Follow the instructions carefully to ensure accurate completion.
- Identify the Waiver Program you are applying for. Select from options such as CIP II, CRI, or others as relevant to your situation.
- Specify the Plan Type: New Recertification, Six Month Review, or Update.
- Enter the current ISP date in the designated area.
- Fill in your Medicaid ID or MCI if applicable.
- Provide your full name, complete address, date of birth, and contact details including telephone and email address.
- If your mailing address differs from your residence, list it under the designated section.
- Record the date of the Functional Screen development and indicate any cost share amount.
- Document the Level of Care and any parental fee if applicable.
- Provide details about your previous and current living arrangements, including the HSRS code.
- Enter information regarding the Waiver Agency, including their name, telephone number, and care manager details.
- List the names and contact information of your parent(s) or guardian.
- Include an emergency contact's name, relationship, and full details.
- For each service required, list the Service Code, Service Name, and the Provider's contact information. Specify the start and end dates as well as unit costs and authorized frequency.
- Confirm that you understand your rights and choices related to the Medicaid waiver programs. Sign and date where required.
- If applicable, complete the UPDATE/REVIEW section to note any changes or updates to your ISP.
- Finally, gather required signatures from you, your support coordinator, guardian, and any witnesses as necessary.
After filling out the form, ensure all information is accurate before submitting it to the Department of Health Services or your county care manager. Keep copies for your records. If you have any questions while completing the form, consider reaching out to a support coordinator or a legal representative for assistance.
What You Should Know About This Form
What is the purpose of the Individual Service Plan (ISP) in Wisconsin?
The Individual Service Plan (ISP) serves as a personalized blueprint for individuals receiving services through Medicaid waiver programs in Wisconsin. It outlines the specific needs, preferences, and goals of the individual based on a functional assessment. By creating this document, care teams can ensure that the services provided align with the individual's unique circumstances and support their overall well-being and independence.
Who is responsible for developing the ISP?
The ISP is developed in collaboration between the individual, their family or guardian, and a Support and Service Coordinator or Care Manager. This person plays a crucial role in facilitating discussions, ensuring the individual's voice is heard, and coordinating the services that are necessary for the individual's care. The involvement of various stakeholders helps to craft a comprehensive plan that addresses all facets of the individual's needs.
How often should the ISP be reviewed and updated?
The ISP must be reviewed at least every six months, but it can be updated more frequently if there are changes in the individual's needs or circumstances. During these reviews, the individual and their team will evaluate the effectiveness of current services, make necessary adjustments, and set new goals as appropriate. This ongoing process is essential for ensuring that the services remain relevant and effective.
What information is included in the ISP?
The ISP includes a wealth of information such as the individual's Medicaid ID, current living arrangements, service provider details, and personal preferences regarding care. Additionally, it outlines specific goals, expected outcomes, and the type and frequency of services covered under the plan. This comprehensive approach facilitates better coordination among service providers and promotes a person-centered strategy for care.
What rights does an individual have regarding their ISP?
Individuals have several rights related to their ISP. They have the right to choose between different service options, including nursing homes and home-based community services. They are also informed about their rights to request hearings if they disagree with decisions related to their eligibility or if services are denied, reduced, or terminated. Understanding these rights empowers individuals to take an active role in their care planning.
What is the process for signing the ISP?
Signing the ISP is a collaborative process that involves several parties. The individual, their guardian (if applicable), and the Support and Service Coordinator or Care Manager must all sign the document, indicating their agreement with the plan. Witnesses may also sign to confirm the authenticity of the agreement. This step is critical as it establishes commitment from all involved and ensures accountability in executing the services outlined in the ISP.
Where can I find the Individual Service Plan form?
The Individual Service Plan form can be obtained through the Wisconsin Department of Health Services or from local agencies involved in the Medicaid waiver programs. The form is available online and can typically be accessed through the respective agency's website. It is important for individuals and their families to ensure they are using the most current version of the form when developing their service plan.
Common mistakes
Filling out the Individual Service Plan (ISP) form in Wisconsin can be a requirement for individuals seeking assistance through Medicaid Waivers. However, many people make common mistakes that can hinder the process and create unnecessary complications. One prevalent mistake involves incomplete personal information. Omitting details such as the participant's full name, address, or date of birth can result in delays or miscommunication between service providers and the individual.
Another frequent error is the failure to specify the correct Waiver Program or Plan Type. Each waiver program has different eligibility criteria and service options. Confusing these categories can lead to misallocation of resources and ultimately unfavorable outcomes for the participant. Clarity is crucial at this initial stage, and selecting the appropriate program helps ensure that the individual receives the intended support.
The third mistake often seen is neglecting to include updated information during the six-month reviews. The ISP needs to reflect any changes in the individual’s circumstances, living arrangements, or provider information. Failing to update these details may result in the continuation of outdated services that no longer meet the individual's needs adequately.
Fourth, individuals sometimes overlook the section on participant rights and choices. This part of the form is vital as it outlines the rights of the participant regarding the services they can choose. Not acknowledging or signing this section can lead to misunderstandings about the available options and consequences regarding service decisions.
Lastly, neglecting proper signatures during the review process is a common oversight. Each signature carries legal weight in confirming that the appropriate parties have reviewed and agreed upon the plan. Incomplete signatures—whether from the participant, care manager, or guardian—render the document invalid, which may require resubmission and further delays in receiving services.
Documents used along the form
The Individual Service Plan (ISP) in Wisconsin is an essential document for individuals participating in Medicaid Waivers. Along with the ISP, several other forms and documents help ensure that individuals receive the services and support they need. Here’s a look at some of these forms.
- Functional Screen Document: This document assesses the individual’s needs and determines their eligibility for the waiver program. It provides a comprehensive overview of the person's functional abilities, supporting decisions about the services required.
- Cost Share Agreement: This agreement outlines any financial participation the individual may have toward their care. It clarifies how much the individual or their family will contribute towards the total cost of services.
- Emergency Contact Form: This form enables important contact information to be readily available in case of emergencies. It ensures that assistance can be quickly provided by listing key contacts and their relationship to the individual.
- Service Authorization Request: This document is used to request approval for specific services outlined in the ISP. It helps providers and payers to confirm that the proposed services are covered by the Medicaid waiver program.
- Participant Rights and Responsibilities Document: This form informs individuals about their rights within the Medicaid Waiver programs. It includes information on choices, privacy, and the process for requesting hearings if they disagree with any decisions made.
Each of these documents plays a vital role in the service planning process. Together, they help create a supportive and responsive system that prioritizes the needs and rights of individuals.
Similar forms
- Individualized Education Program (IEP): Similar to the ISP, the IEP outlines specific educational goals and services for students with disabilities. Both documents are tailored to meet individual needs.
- Personal Support Plan (PSP): This document provides an overview of the support an individual needs to live successfully in the community. Like the ISP, it focuses on personal preferences and goals.
- Family Support Plan: Created for families with children who have disabilities, this plan addresses the family's needs for support and resources, akin to how the ISP addresses individual needs.
- Health and Safety Plan: This plan includes measures to ensure a person's safety and health. Both the ISP and this plan evaluate risks and supports necessary to maintain well-being.
- Behavior Intervention Plan (BIP): Used for individuals needing guidance on managing behaviors, the BIP shares similarities with the ISP in its tailored approach to achieving specific outcomes.
- Transitional Living Plan: For youth transitioning to adulthood, this plan outlines necessary supports and services. Like the ISP, it is designed to facilitate a smooth transition based on individual preferences.
- Service Coordination Plan: This document details services provided to individuals with complex needs. It aligns closely with the ISP in its focus on coordinating various supports for an individual.
- Case Management Plan: Focused on addressing an individual's broader needs, this plan shares the goal of promoting overall well-being, similar to what is intended in the ISP.
- Comprehensive Assessment and Plan: Used to determine an individual’s strengths, needs, and goals, this document complements the ISP's purpose of personalized planning.
- Community Living Plan: Designed for individuals seeking to live independently, it mirrors the ISP in emphasizing personal choice and support services required for success.
Dos and Don'ts
Do's:
- Ensure all personal information such as name, address, and date of birth are accurately filled out.
- Reach out to the appropriate waiver agency if there are questions regarding the form.
- Review the Individual Service Plan with the participant to confirm accuracy and understanding.
- Document any changes made to the ISP during the six-month review period.
- Include all necessary signatures before submitting the form.
Don'ts:
- Do not leave any sections of the form blank; fill out each applicable field.
- Avoid using abbreviations that may not be understood by all parties reviewing the form.
- Do not submit the form without confirming that the participant's rights have been reviewed and acknowledged.
- Refrain from altering any provided agency information without proper confirmation.
- Do not overlook the distribution requirements; ensure copies are given to all relevant parties.
Misconceptions
Misconception 1: The Individual Service Plan (ISP) is just a formality.
Many individuals believe that the ISP is simply a bureaucratic requirement that does not significantly impact their care. In reality, the ISP is a detailed plan tailored to a person's needs, outlining the services they require and the manner in which those services will be provided. It's a vital tool for ensuring that participants receive appropriate care and support.
Misconception 2: The ISP is only useful for Medicaid beneficiaries.
Some people think that the ISP only serves those on Medicaid, but this is not the case. While the ISP is often associated with Medicaid Waivers, it can be relevant for anyone receiving long-term care services. It helps to coordinate care across various service providers and ensures that everyone involved understands the individual’s needs.
Misconception 3: Once completed, the ISP cannot be changed.
Contrary to popular belief, the ISP is not set in stone. It is designed to be a living document that can be updated as needs change. Reviews are conducted regularly, often every six months, allowing for adjustments in services or providers based on the individual's evolving circumstances.
Misconception 4: Participants have no say in their ISP.
Another common misconception is that participants are merely recipients of the ISP without any input in the planning process. In truth, individuals possess the right to actively participate in discussions about their services. They are encouraged to voice their preferences, choices, and needs, thereby ensuring that the plan reflects their personal goals and desires.
Key takeaways
Filling out the Individual Service Plan Wisconsin form is crucial for ensuring that individuals receive the support they need through Medicaid programs. Here are key takeaways to consider:
- Accurate Information is Essential: Ensure all personal details, including name, address, and date of birth, are correctly entered. Inaccuracies can delay service provision.
- Understand Your Rights: Participants have the right to choose between nursing home services and community-based options. Familiarize yourself with these rights to make informed decisions.
- Documentation of Changes: Any updates to the service plan should be documented during the six-month review. Changes may include adjustments to service providers or frequency of services.
- Signatures are Required: Ensure all necessary signatures are obtained at the time of plan development or updates. This ensures that everyone involved acknowledges and agrees to the contents of the plan.
Browse Other Templates
Aarp Claim Form - This form also outlines options for claim payment, including a Continued Interest Account.
Tflnnnj - Keep in mind deadlines for claims submissions to avoid complications.