Fill Out Your Kaiser Records Request Form
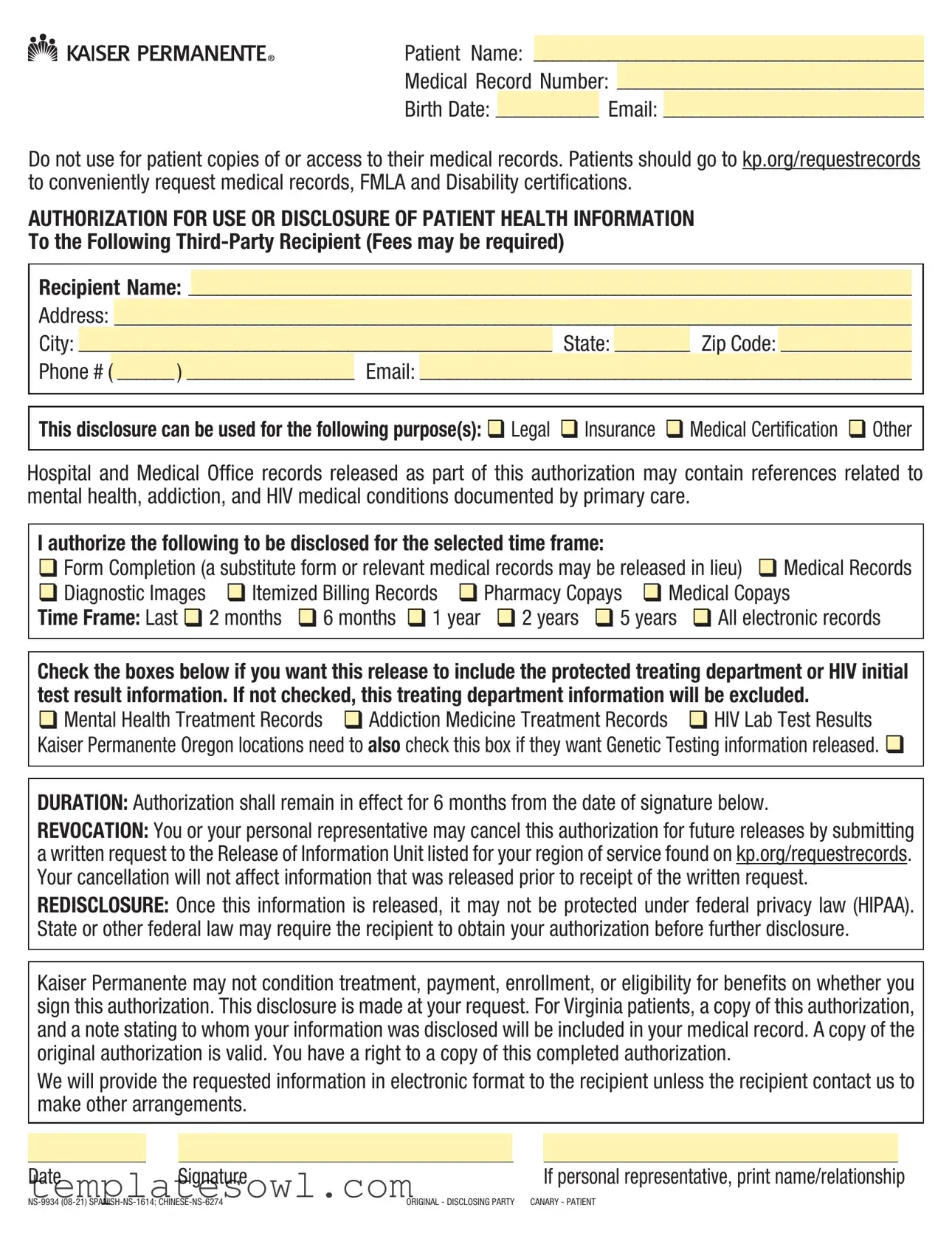
The Kaiser Records Request form plays a crucial role in managing and authorizing the release of patient health information. Designed with patient privacy in mind, it allows individuals to designate a third party to access their medical records for various purposes, such as legal reasons or insurance claims. Key elements include sections for personal identification, recipient information, and the specific types of records being requested, which can range from medical history to billing details. Importantly, patients are advised to use the kp.org platform for direct access to their medical records and certifications instead of this form. The authorization remains valid for six months, enabling patients to make informed decisions about their health information sharing. Notably, patients may request the release of sensitive information, including mental health records or HIV lab results, under strict guidelines. Understanding and correctly completing this form is essential for both patients and third parties to ensure a smooth and compliant process in obtaining necessary medical documentation.
Kaiser Records Request Example
Patient Name: __________________________________________
Medical Record Number: _________________________________
Birth Date: ___________ Email: ____________________________
Do not use for patient copies of or access to their medical records. Patients should go to kp.org/requestrecords to conveniently request medical records, FMLA and Disability certifications.
AUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT HEALTH INFORMATION
To the Following
Recipient Name: ______________________________________________________________________________
Address: ______________________________________________________________________________________
City: ___________________________________________________ State: ________ Zip Code: ______________
Phone # ( ______ ) __________________ Email: _____________________________________________________
This disclosure can be used for the following purpose(s): Legal Insurance Medical Certification Other
Hospital and Medical Office records released as part of this authorization may contain references related to mental health, addiction, and HIV medical conditions documented by primary care.
I authorize the following to be disclosed for the selected time frame:
Form Completion (a substitute form or relevant medical records may be released in lieu) Medical Records
|
Diagnostic Images |
|
|
Itemized Billing Records |
|
Pharmacy Copays |
|
Medical Copays |
||||||||||
|
|
|
||||||||||||||||
|
|
|
|
|||||||||||||||
Time Frame: Last |
|
2 months |
|
6 months |
|
1 year |
2 years |
|
5 years |
|
All electronic records |
|||||||
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|||||||||||||
Check the boxes below if you want this release to include the protected treating department or HIV initial test result information. If not checked, this treating department information will be excluded.
Mental Health Treatment Records Addiction Medicine Treatment Records HIV Lab Test Results Kaiser Permanente Oregon locations need to also check this box if they want Genetic Testing information released.
DURATION: Authorization shall remain in effect for 6 months from the date of signature below.
REVOCATION: You or your personal representative may cancel this authorization for future releases by submitting a written request to the Release of Information Unit listed for your region of service found on kp.org/requestrecords. Your cancellation will not affect information that was released prior to receipt of the written request.
REDISCLOSURE: Once this information is released, it may not be protected under federal privacy law (HIPAA). State or other federal law may require the recipient to obtain your authorization before further disclosure.
Kaiser Permanente may not condition treatment, payment, enrollment, or eligibility for benefits on whether you sign this authorization. This disclosure is made at your request. For Virginia patients, a copy of this authorization, and a note stating to whom your information was disclosed will be included in your medical record. A copy of the original authorization is valid. You have a right to a copy of this completed authorization.
We will provide the requested information in electronic format to the recipient unless the recipient contact us to make other arrangements.
|
|
|
|
|
|
|
Date |
|
Signature |
|
|
If personal representative, print name/relationship |
|
ORIGINAL - DISCLOSING PARTY CANARY - PATIENT |
||||||
Instructions:
1)Complete the patient identification information on the top
2)Complete all required information for the recipient including a valid email address
3)Check the box for purpose of disclosure
4)Check the box(es) for the type of information to be disclosed and also check the box for a timeframe
5)If you want specially protected information to be included, check the appropriate box(es)
6)Enter the date you are signing the authorization
7)Sign the form
8)If you are a personal representative, print your name and relationship. We may reach out for you to provide additional documentation if needed.
9)Submit this form to the third party you are authorizing to obtain records
10)Keep a copy for your records
“Kaiser Permanente” means both your insurance company (a Kaiser Permanente health plan) and your doctors (a Permanente medical or dental group). It also includes different groups depending on where you live.
To find contact information go to kp.org and search locations for your region/market listed below or alternatively go to kp.org/requestrecords and indicate your region/market.
All states where we do business:
•Kaiser Foundation Hospitals
•Kaiser Permanente Insurance Company
Colorado:
•Kaiser Foundation Health Plan of Colorado
•Colorado Permanente Medical Group, P.C.
Georgia:
•Kaiser Foundation Health Plan of Georgia, Inc.
•The Southeast Permanente Medical Group, Inc.
•Kaiser Foundation Health Plan of the
•
Washington:
•Kaiser Foundation Health Plan of Washington
•Washington Permanente Medical Group, P.C.
Hawaii:
•Kaiser Foundation Health Plan, Inc., Hawaii Region
•Hawaii Permanente Medical Group, Inc.
•Maui Health Systems
Northwest (Oregon/SW Washington):
•Kaiser Foundation Health Plan of the Northwest
•Northwest Permanente, P.C.
•Permanente Dental Associates, P.C.
California - North:
•Kaiser Foundation Health Plan, Inc., Northern California Region
•The Permanente Medical Group, Inc.
California - South:
•Kaiser Foundation Health Plan, Inc., Southern California Region
•Southern California Permanente Medical Group
Patient Name: __________________________________________
Medical Record Number: _________________________________
Birth Date: ___________ Email: ____________________________
Do not use for patient copies of or access to their medical records. Patients should go to kp.org/requestrecords to conveniently request medical records, FMLA and Disability certifications.
AUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT HEALTH INFORMATION
To the Following
Recipient Name: ______________________________________________________________________________
Address: ______________________________________________________________________________________
City: ___________________________________________________ State: ________ Zip Code: ______________
Phone # ( ______ ) __________________ Email: _____________________________________________________
This disclosure can be used for the following purpose(s): Legal Insurance Medical Certification Other
Hospital and Medical Office records released as part of this authorization may contain references related to mental health, addiction, and HIV medical conditions documented by primary care.
I authorize the following to be disclosed for the selected time frame:
Form Completion (a substitute form or relevant medical records may be released in lieu) Medical Records
Diagnostic Images |
Itemized Billing Records Pharmacy Copays Medical Copays |
Time Frame: Last |
2 months 6 months 1 year 2 years 5 years All electronic records |
Check the boxes below if you want this release to include the protected treating department or HIV initial test result information. If not checked, this treating department information will be excluded.
Mental Health Treatment Records Addiction Medicine Treatment Records HIV Lab Test Results Kaiser Permanente Oregon locations need to also check this box if they want Genetic Testing information released.
DURATION: Authorization shall remain in effect for 6 months from the date of signature below.
REVOCATION: You or your personal representative may cancel this authorization for future releases by submitting a written request to the Release of Information Unit listed for your region of service found on kp.org/requestrecords. Your cancellation will not affect information that was released prior to receipt of the written request.
REDISCLOSURE: Once this information is released, it may not be protected under federal privacy law (HIPAA). State or other federal law may require the recipient to obtain your authorization before further disclosure.
Kaiser Permanente may not condition treatment, payment, enrollment, or eligibility for benefits on whether you sign this authorization. This disclosure is made at your request. For Virginia patients, a copy of this authorization, and a note stating to whom your information was disclosed will be included in your medical record. A copy of the original authorization is valid. You have a right to a copy of this completed authorization.
We will provide the requested information in electronic format to the recipient unless the recipient contact us to make other arrangements.
|
|
|
|
|
|
|
Date |
Signature |
|
|
If personal representative, print name/relationship |
||
ORIGINAL - DISCLOSING PARTY CANARY - PATIENT |
||||||
Form Characteristics
| Fact Name | Fact Description |
|---|---|
| Patient Identification Requirement | This form requires essential patient details including name, medical record number, and birth date for identification purposes. |
| Email Provision | The form asks for an email address for efficient communication regarding the request. |
| Purpose of Disclosure | Individuals can specify the purpose for which the health information is being shared, including legal and medical insurance matters. |
| Protected Information | Options to include sensitive health information, such as mental health records or HIV test results, are available and must be explicitly checked. |
| Time Frame Options | Patients can indicate a desired time frame for the information requested, ranging from the last two months to five years. |
| Duration of Authorization | The authorization for disclosure remains valid for six months from the date of signing. |
| Revocation Process | Patients can revoke their authorization at any time by submitting a written request, which will not affect previous disclosures. |
| Redisclosure Warning | Once the information is disclosed, it may not be protected under HIPAA, and further disclosures may require additional authorization. |
| State-Specific Regulations | In Virginia, a copy of the authorization and a disclosure note will be included in the patient's medical record, adhering to state-specific laws. |
| Submission Guidance | Patients must ensure that the form is filled out correctly before submitting it to the authorized third party and should keep a copy for their records. |
Guidelines on Utilizing Kaiser Records Request
Completing the Kaiser Records Request form accurately is essential for ensuring that your medical records are sent to the appropriate recipient. Following the steps outlined below will help streamline the process, making it easier for you to authorize the release of your health information.
- Fill in the patient identification information in the top right corner, including your name, medical record number, birth date, and email address.
- Provide all necessary details about the recipient you are authorizing to obtain your records, including their name, address, city, state, zip code, phone number, and a valid email address.
- Select a purpose for the disclosure by checking the appropriate box (Legal, Insurance, Medical Certification, or Other).
- Choose the type of information you wish to disclose by checking the corresponding boxes, and indicate a time frame for the records being released.
- If you want to include specially protected information, check the relevant boxes for Mental Health Treatment Records, Addiction Medicine Treatment Records, or HIV Lab Test Results.
- Write the date you are signing the authorization in the specified space.
- Sign the form to authorize the release of your information.
- If you are completing the form as a personal representative, print your name and your relationship to the patient.
- Submit the completed form to the recipient you specified.
- Keep a copy of the signed form for your records.
What You Should Know About This Form
What is the Kaiser Records Request form?
The Kaiser Records Request form is used to authorize the release of your medical information to a third party. This might include legal representatives, insurance providers, or other designated individuals. It's important to note that this form should not be used by patients to request their own records. For that, you should visit kp.org/requestrecords.
Who can I authorize using this form?
You can authorize any individual or organization that you trust to handle your medical information. This could include lawyers, insurance companies, or other service providers. Just ensure you provide their complete contact information on the form.
What types of information can I request to be disclosed?
The form allows you to select various types of information for disclosure, such as medical records, diagnostic images, itemized billing records, and more. You can also choose to include sensitive information, like mental health or HIV-related records, if needed. Just be sure to check the appropriate boxes on the form.
How long is the authorization valid?
Your authorization will stay valid for six months from the date you sign the form. After this period, the third party will no longer be able to access your medical records without a new request from you.
What if I change my mind?
If you decide you no longer want to authorize the release of your medical records, you can revoke the authorization. To do this, you need to submit a written request to the Release of Information Unit for your region. Keep in mind that any information released before your cancellation can’t be undone.
Can I obtain my own medical records using this form?
No, you cannot use this form to request your own medical records. If you're looking to access your personal medical records, please visit kp.org/requestrecords for assistance. That site provides a convenient way for patients to get their own information directly.
What happens after I submit the request?
Once you submit the Kaiser Records Request form, Kaiser Permanente will process your request and send the specified information directly to the designated recipient. If the recipient prefers a different format or arrangement, they can contact Kaiser to discuss other options.
Do I need to keep a copy of the form?
Yes, it's a good idea to keep a copy of the completed authorization for your records. This way, you have a reference for what information was requested and when, in case you need it later.
Common mistakes
When filling out the Kaiser Records Request form, one common mistake is leaving out essential patient information. Missing the Patient Name, Medical Record Number, or Birth Date can lead to delays in processing the request. Make sure to provide complete and accurate identification details to ensure your request is not held up.
Another frequent error is not providing all required information for the third-party recipient. Omitting the Recipient Name, Address, or Email renders the request incomplete. Without these details, the records cannot be properly sent, which can frustrate all parties involved.
Some individuals overlook the importance of checking the appropriate purpose for disclosure. This section is critical and must be filled out correctly to specify why the records are needed. Whether it’s for Legal, Insurance, or Medical Certification, checking the right boxes helps streamline the process.
Failure to indicate the type of information requested is another mistake that can impede the process. It is crucial to check all relevant boxes, including Medical Records, Diagnostic Images, and any others that apply to your situation. Skipping this step may lead to incomplete disclosures.
Choosing the Time Frame for the records is equally important. If this section is left blank or incorrectly filled, it may cause confusion. Always verify that you have selected a specific period for which you wish to obtain health information.
An additional error is neglecting to check the boxes related to specially protected information, such as Mental Health Treatment Records or HIV Lab Test Results. If you want this sensitive information included, failing to check these boxes means it will be excluded from your request.
People sometimes forget to sign the form or indicate the date of signature. Without this information, the authorization is not valid. Make sure to take a moment to sign and date the document before submitting it.
Lastly, retaining a copy of the completed authorization is often overlooked. Keeping this copy is vital for your records, as it allows you to track your request and provides crucial information if follow-up is needed later.
Documents used along the form
The Kaiser Records Request form serves as a critical instrument for patients needing to access their health information. However, several other forms and documents often accompany or complement it during the records request process. Below is a brief overview of these documents, which play important roles in ensuring the efficiency and legality of obtaining medical records.
- Patient Authorization Form: This document grants permission to a healthcare provider to share a patient's health information with a specified third party. It outlines what information can be shared and for what purpose.
- Release of Information Form: Similar to the authorization form, this document is specifically used to allow a healthcare provider to release certain medical records upon request, often required by insurers or legal representatives.
- Medical History Form: This form collects vital background information about the patient's health, including previous conditions and treatments. It aids in providing context for the records being requested.
- Request for Copies of Medical Records: Utilized by patients seeking a physical copy of their records, this form outlines the specific documents requested and may include a small fee for processing.
- Release for Psychological Records: This specialized release form is required for sharing sensitive mental health records, ensuring additional protections for particularly private information.
- FMLA Certification Form: This document is used to certify a patient's need for Family and Medical Leave Act leave. It often requires medical information directly from a healthcare provider.
- Disability Certification Form: Patients must complete this form to apply for disability benefits. It typically requests information on the patient’s medical condition as verified by their healthcare provider.
- Privacy Practices Acknowledgment: Patients must acknowledge receipt of the healthcare provider's privacy practices, ensuring they understand their rights regarding their medical information.
- Notice of Privacy Practices: This document provides patients with a detailed explanation of how their health information may be used and disclosed, safeguarding their understanding of privacy rights.
- Power of Attorney for Health Care: This legal document designates someone to make medical decisions on a patient’s behalf, often necessary when the patient is not in a position to make decisions themselves.
Each of these forms and documents plays a significant role in the overall process of managing and retrieving health records. Understanding their importance can empower individuals to navigate the healthcare system more effectively, ensuring that their rights and needs are respected.
Similar forms
The Kaiser Records Request form shares similarities with several other documents used for requesting and authorizing the release of medical information. Below are four documents similar to the Kaiser Records Request form:
- HIPAA Authorization Form: This document allows patients to authorize the release of their medical records per HIPAA regulations. Like the Kaiser form, it requires patient identification, recipient information, and purpose for disclosure.
- Patient Medication Records Release Form: This form is specific for obtaining a patient’s medication history from pharmacies or clinics. It includes sections for patient demographic information and recipient details, similar to the format of the Kaiser form.
- Insurance Medical Records Request Form: Insurance companies often require a form to request specific medical records for claims processing. This document outlines requested records and requires similar authorizations as the Kaiser Records Request form.
- Disability or Family Medical Leave Act (FMLA) Certification Form: This form is used to request documentation for leave purposes. It requires patient information, recipient details, and specifies the type of records needed, reflecting aspects seen in the Kaiser request form.
Dos and Don'ts
When filling out the Kaiser Records Request form, it's important to follow certain guidelines. Here are some dos and don'ts to keep in mind:
- Do complete the patient's identification information clearly.
- Do provide a valid email address for the recipient.
- Do specify the purpose of the disclosure by checking the appropriate box.
- Do indicate the type of information you wish to release.
- Do ensure you check the box for a timeframe.
- Don’t forget to sign and date the form before submitting it.
- Don’t leave any required fields blank; this can cause delays.
- Don’t use this form for personal copies of your medical records.
- Don’t submit the form without making a copy for your records.
Misconceptions
There are several misconceptions about the Kaiser Records Request form. Clarifying these can help ensure a smooth process for obtaining necessary medical records.
- It can be used by patients to request their own medical records. This form is specifically for authorizing the release of records to a third-party recipient. Patients should visit kp.org/requestrecords for personal requests.
- All requests are free of charge. Some requests may involve fees, depending on the nature of the request and the information being disclosed.
- You can request records for any time frame without limitation. The form allows you to choose a specific time frame, such as the last two months, up to five years, or all electronic records.
- Signing the form is sufficient for immediate action. The form must be submitted to the designated third-party recipient, not Kaiser Permanente, for action to be taken.
- The authorization lasts indefinitely. The authorization remains valid for only six months from the date of signature. After this period, a new authorization is required.
- Medical information will be fully protected after disclosure. Once the information is shared, it may no longer be protected under federal privacy laws, except as dictated by state or other federal laws.
- Patients cannot revoke their authorization. Patients may cancel future releases at any time by submitting a written request to the Release of Information Unit.
- This form applies to all medical information. While it allows for the release of many types of records, specially protected information like mental health or HIV records require specific boxes to be checked for inclusion.
Understanding these points can streamline the records request process and ensure that all parties have the information they need.
Key takeaways
- The Kaiser Records Request form is strictly for authorizing the release of medical information to third parties, not for personal access to medical records.
- Patients should visit kp.org/requestrecords for direct requests regarding their own medical records, FMLA, or disability certifications.
- It is necessary to provide complete recipient details, including name, address, and email, as this information ensures the authorized release is sent to the correct party.
- Specific purposes for the disclosure must be checked, including options like legal, insurance, and medical certification, which clarify why the records are needed.
- The duration of the authorization is valid for 6 months, after which a new request will be necessary; however, previously disclosed information cannot be retracted.
Browse Other Templates
Which Credit Reference Agency Do Volkswagen Finance Use - The form requires signatures from both the applicant and co-applicant, indicating a desire for joint credit if applicable.
Fsbp - Sign and date the form to certify the truthfulness of the information provided.
Urolith - Fax information helps facilitate communication regarding test results.